Widespread Encephalitis Following Acute Sinusitis in a Pediatric Patient
Elif Gozgec, Muhammed Mukremin Bugdaci

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
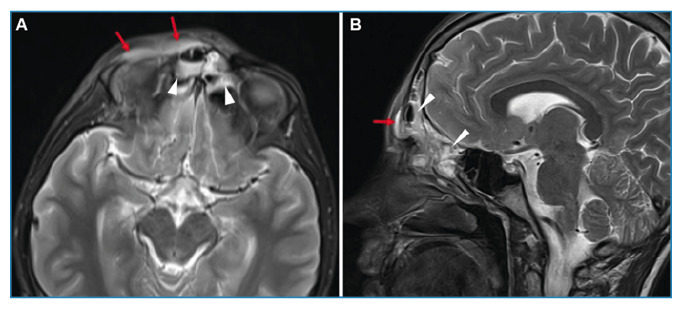 Figure 1
Figure 1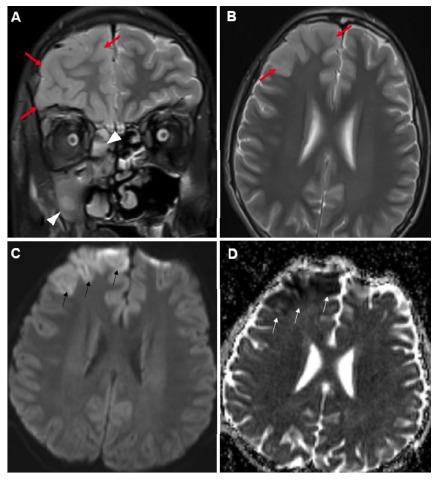 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Encephalopathies and Encephalitis · Sinusitis and nasal conditions · Bacterial Infections and Vaccines
A 16-year-old boy was admitted to our clinic with a complain of headache, fever, rhinorrhea, and erythema of the right eye for 3 days with no known history of disease or surgery. Physical examination revealed tonsillar hyperemia and tenderness in the right frontal region. Hyperemia and ptosis were observed in the right eye. Neurological examinations revealed no abnormalities. The white cell count was 8.7×10^3^/µL; C-reactive protein concentration was 68.6 mg/dL; and sedimentation rate was 64 mm/h. Magnetic resonance imaging (MRI) showed pansinusitis and inflammation signs in the right periorbital region (Figure 1). T2-weighted images revealed greater thickness and intensity in the grey matter of the right frontal lobe of the brain. These areas exhibited marked restrictions on diffusion-weighted images and minimal contrast enhancement (Figure 2). Intravenous ceftriaxone, metronidazole, and vancomycin treatment was initiated under the diagnosis of encephalitis. Controlled MRI performed on the 14th day of treatment revealed significant regression of encephalitis.
FIGURE 1:Axial (A) and sagittal (B) section T2-weighted brain MRI show diffuse intensity increases (arrowheads) of sinusitis in the ethmoid cells and frontal sinus. Additionally, greater intensity and thickness (red arrows) are observed in the right periorbital area.
FIGURE 2:Coronal (A) and axial (B) section T2-weighted brain MRI scans show greater intensity in the right maxillary sinus and ethmoid cells consistent with sinusitis (arrowheads) and diffuse thickness and greater intensity in the gray matter in the right frontal lobe (red arrows). Axial diffusion-weighted images show greater intensity in the B-1000 series (C) and hypointense appearance (arrows) in apparent diffusion coefficient mapping (D) in the frontal lobe.
Encephalitis, a rare intracranial complication of sinusitis, is associated with high risks of mortality and morbidity1. Complications are more common in the frontal region due to the high frequency of frontal sinusitis in adolescents, high blood flow in the frontal sinuses, and the high density of diploic veins in this region2. Diagnosis can be difficult owing to the potential for symptoms similar to sinusitis. Radiological imaging is crucial for diagnosis and monitoring.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Germiller JA Monin DL Sparano AM Tom LW Intracranial complications of sinusitis in children and adolescents and their outcomes Arch Otolaryngol Head Neck Surg 2006132996997610.1001/archotol.132.9.96916982973 · doi ↗ · pubmed ↗
- 2Hakim HE Malik AC Aronyk K Ledi E Bhargava R The prevalence of intracranial complications in pediatric frontal sinusitis Int J Pediatr Otorhinolaryngol 20067081383138710.1016/j.ijporl.2006.02.00316530852 · doi ↗ · pubmed ↗