An Unusual Case of Genital Myiasis in Nicaragua: A Multidisciplinary Approach in a Patient With Stage IV Pelvic Organ Prolapse
María Esther Suárez Garcia, Andres Rivera, Jasser Logo Cabrera, Ramon Roque, Jorge Cristhian Ocon Espinoza, Christopher Kaleb Romero Ríos

TL;DR
A rare case of genital myiasis in a patient with severe pelvic organ prolapse is managed through surgery, antibiotics, and hygiene education.
Contribution
This case report presents a multidisciplinary approach to managing myiasis complicated by stage IV pelvic organ prolapse.
Findings
Surgical debridement and tailored antibiotics effectively treated myiasis and secondary infections.
Definitive surgery resolved the underlying pelvic organ prolapse.
Multidisciplinary care and hygiene education are crucial for managing such complex cases.
Abstract
Myiasis, a parasitic infestation caused by fly larvae in necrotic tissue, is rare in urban settings but can complicate conditions like advanced pelvic organ prolapse (POP). This report highlights the diagnostic and therapeutic challenges of myiasis in a patient with grade IV POP. An 85-year-old postmenopausal woman presented with a four-year history of vaginal mass protrusion, recent bleeding, foul discharge, and necrotic tissue. Examination revealed grade IV POP with left-sided necrotic tissue (4 × 4 cm) infested with larvae. Laboratory findings showed leukocytosis (17.57 × 10³/µL), elevated CRP (28.03 mg/dL), and a hemoglobin level of 14 g/dL. Management included surgical debridement, saline/chlorhexidine lavage, ivermectin, and broad-spectrum antibiotics (ceftriaxone/clindamycin), later adjusted to cefepime after cultures grew Escherichia coli and Sphingomonas paucimobilis. Imaging…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2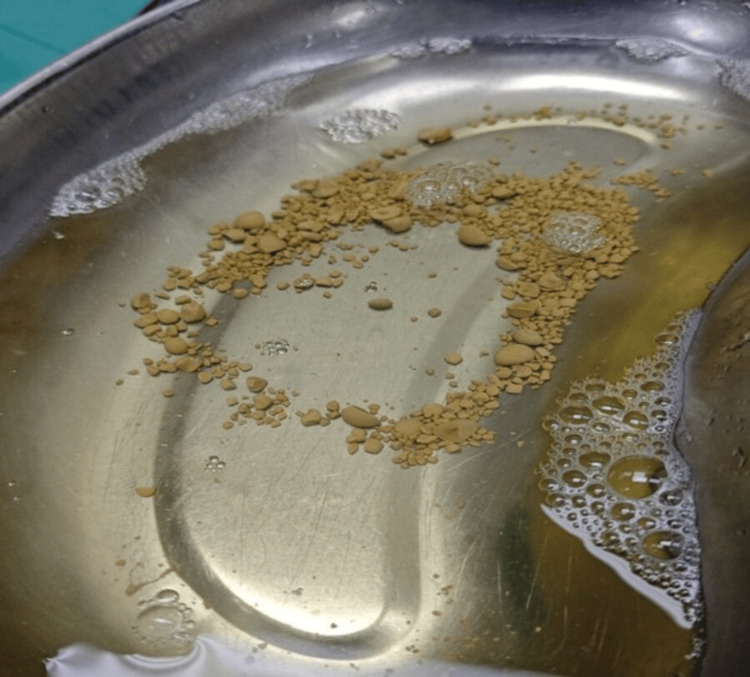 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForensic Entomology and Diptera Studies · Climate Change and Health Impacts · Diptera species taxonomy and behavior
Introduction
Myiasis, the parasitic infestation of human tissues by fly larvae, primarily occurs in necrotic or decomposing tissue [1]. Although more prevalent in tropical regions, urban cases are increasingly reported, especially among populations with open wounds, suboptimal hygiene practices, or immunosuppressive conditions [2]. While cutaneous manifestations dominate clinical reports, genital and pelvic myiasis remains exceptionally rare, with only sporadic cases associated with advanced pelvic organ prolapse (POP) [3]. Grade IV uterine prolapse, defined by complete extrusion of the uterus beyond the vaginal introitus, generates a microenvironment of chronic tissue ischemia, mucosal ulceration, and bacterial colonization, creating a nidus for secondary infections [4]. Reports of myiasis complicating POP are strikingly limited, and current management protocols lack standardization, often requiring multimodal strategies such as mechanical larval extraction, antimicrobial therapy, and definitive surgical correction of anatomical defects [5]. The confluence of prolonged tissue exposure, inadequate wound care, and environmental factors (e.g., warm climates or poor sanitation) heightens susceptibility to infestation; nonetheless, fewer than 10 cases of POP-associated myiasis have been documented worldwide, reflecting its status as a medical rarity [3,6].
This case contributes to the sparse literature by detailing a multidisciplinary approach to managing myiasis in grade IV POP, a scenario with unique anatomical and logistical challenges. It highlights the critical need for early recognition, aggressive debridement, and tailored surgical planning to mitigate life-threatening complications such as sepsis or systemic larval migration. By synthesizing existing evidence with novel clinical insights, this report aims to inform future guidelines for high-risk populations and reinforce the importance of integrating parasitological management into gynecologic care.
Case presentation
An 85-year-old woman with infected grade IV POP type C presented to the ED with a five-day history of scant vaginal bleeding, a protruding genital mass (present for four years), throbbing pelvic pain, severe perineal itching, and foul-smelling discharge. She lived in an urban area, denied trauma or insect bites, and had no significant medical history. Her gynecological background included menarche at age 14, multiple pregnancies, menopause at 52, and no prior cervical cancer screenings.
On examination, she was hemodynamically stable and alert. Gynecological evaluation revealed a grade IV POP with complete cervical protrusion (+6 cm beyond the vaginal introitus) and a 4 × 4 cm area of necrotic, malodorous tissue on the left side (Figure 1). Laboratory findings included leukocytosis (17.57 × 10³/µL, 82.1% neutrophils), elevated CRP (28.03 mg/dL), and normal renal, coagulation, and electrolyte panels.
Myiasis (larval infestation) in necrotic prolapsed tissue
She underwent urgent surgical debridement. Intraoperatively, grade IV POP with myiasis (fly larvae infestation) was confirmed, alongside extensive left-sided necrotic tissue. Secretion cultures and a Pap smear were collected. Necrotic tissue was excised, followed by rigorous irrigation with saline and 4% chlorhexidine to remove larvae. Minimal bleeding was noted. Postoperatively, she received broad-spectrum antibiotics (ceftriaxone and clindamycin) and oral ivermectin, managed by a multidisciplinary team. A second debridement revealed persistent necrotic tissue (7 × 4 cm), which was irrigated again (Figure 2).
Grade IV POP with fibrin deposits post-debridementPOP, pelvic organ prolapse
Microbial cultures identified *Escherichia coli *and Sphingomonas paucimobilis, prompting a switch to cefepime as antibiotic therapy. Initial management did not include hysterectomy due to suspicion of vesical myiasis suggested by pelvic MRI, which revealed bladder prolapse and multiple rounded calcifications (2-18 mm). Subsequent cystoscopy confirmed the presence of bladder stones, with the largest calculus measuring 15 mm in diameter, treated via pneumatic lithotripsy and Foley catheter placement (Figure 3). Post-procedure, a 7 × 5 cm fibrinous tissue in the prolapsed area was irrigated.
Bladder stones removed via lithotripsy
Twice-daily wound care with chlorhexidine, saline, and ketanserin gel promoted healing, resolving infection and larval presence but leaving residual fibrin. After two surgical lavages, definitive surgery - vaginal hysterectomy, colpectomy, and perineoplasty - was performed. Intraoperatively, friable scar tissue and fibrosis (7 × 4 cm) were noted (Figure 4).
Severe prolapse prior to definitive surgery
The patient recovered well post-surgery (Figure 5). Her postoperative course was marked by steady improvement, including stable hemodynamics and optimal wound healing. Based on these positive outcomes, she was cleared for discharge 72 hours after the procedure. A follow-up evaluation was arranged within 48 hours via the outpatient clinic to monitor recovery, evaluate anatomical repair, and address any emerging concerns, reinforcing a patient-centered transition from hospital to home care.
Postoperative anatomical restoration
Discussion
Severe uterine prolapse in postmenopausal women leads to ischemia, ulceration, and secondary infection, conditions that may attract insect vectors of myiasis [2]. Myiasis, a parasitic infestation caused by fly larvae in living tissues, typically occurs in settings of poor hygiene, open wounds, or tissue necrosis. Its manifestation in the genital tract is rare and poses diagnostic and therapeutic challenges. In this case, a patient with grade IV POP developed superimposed myiasis, complicating her clinical course and necessitating multidisciplinary intervention [7].
Therapeutic management of myiasis involves larval removal, surgical debridement of necrotic tissue, and empiric antibiotics to prevent secondary bacterial infections [8]. Here, initial treatment included broad-spectrum antibiotics, later adjusted after cultures identified E. coli and *S. paucimobilis *- opportunistic pathogens capable of causing severe infections in immunocompromised patients or those with devitalized tissue [9].
A notable finding in this case was bladder lithiasis, detected by MRI, which raised suspicion of vesical myiasis. Although rare, larval infestation of the urinary tract has been reported in patients with immunosuppression or poor hygiene. Surgical resolution through cystolithotripsy ruled out bladder larvae and improved the patient’s prognosis [10].
Definitive treatment included vaginal hysterectomy, colpectomy, and perineoplasty - well-established techniques for advanced uterine prolapse. Vaginal hysterectomy is a safe and effective procedure for prolapse correction, minimizing surgical trauma and accelerating recovery [11]. The Rouhier colpocleisis technique, combining vaginal hysterectomy with vaginal closure, is used to manage POP associated with uterine pathology [12].
In this 85-year-old patient with grade IV POP and myiasis, colpohysterectomy effectively resolved the prolapse and associated complications. The procedure enabled necrotic tissue removal and pelvic anatomy restoration, enhancing the patient’s quality of life [13]. It is important to highlight that the choice of surgical technique should be individualized, taking into account factors such as the patient’s age, comorbidities, desire to preserve sexual function, and the presence of other medical conditions. In elderly patients or those at high surgical risk, colpocleisis, which involves the partial or total closure of the vaginal cavity, may be an appropriate alternative [14,15].
Medical literature on myiasis complicating uterine prolapse remains scarce. This case underscores the need to document and study such rare presentations to refine clinical and preventive strategies. Hygiene education and regular medical follow-up in women with advanced POP are critical to preventing this condition [12].
Conclusions
Myiasis in the context of advanced POP is a rare yet potentially severe complication. In this case, prompt identification and multidisciplinary management ensured a favorable outcome, underscoring the critical role of timely diagnosis and definitive surgical intervention. The presence of secondary bacterial infections and suspected vesical myiasis (bladder involvement) highlights the complexity of such cases and the necessity for rigorous clinical vigilance.
Given the limited literature on this condition, this case enriches clinical understanding and emphasizes the importance of preventive measures, including proper hygiene and regular medical follow-up in patients with severe uterine prolapse. Documenting such cases is vital to refining future clinical management and enhancing care protocols, ensuring optimized outcomes for similar presentations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Myiasis Clin Microbiol Rev Francesconi F Lupi O 791052520122223237210.1128/CMR.00010-11PMC 3255963 · doi ↗ · pubmed ↗
- 2Wound myiasis in urban and suburban United States Arch Intern Med Sherman RA 200420141602000 https://pubmed.ncbi.nlm.nih.gov/10888974/1088897410.1001/archinte.160.13.2004 · doi ↗ · pubmed ↗
- 3Myiasis in an urban setting: a case report Can J Infect Dis Predy G Angus M Honish L E Burnett C Stagg A 51521520041815944310.1155/2004/978427 PMC 2094924 · doi ↗ · pubmed ↗
- 4Prevention and management of pelvic organ prolapse F 1000 Prime Rep Giarenis I Robinson D 77620142534303410.12703/P 6-77PMC 4166938 · doi ↗ · pubmed ↗
- 5Myiasis in uterine prolapse [Article in Spanish]Rev Peru Ginecol Obstet Au AS Peñaranda W 143145552015
- 6Myiasis in grade IV genital prolapse [Article in Spanish]Investig Desarro Mena B Ramos D 10110452022
- 7Myiasis in humans—a global case report evaluation and literature analysis Parasitol Res Bernhardt V Finkelmeier F Verhoff MA Amendt J 38939711820193045649010.1007/s 00436-018-6145-7 · doi ↗ · pubmed ↗
- 8Acute and chronic wound in myasis management. Cases report and bibliography review [Article in Spanish]Rev Argent Dermatol Mengarelli RH Cevallos MV 932012 https://www.scielo.org.ar/scielo.php?script=sci_arttext&pid=S 1851-300X 2012000300004