Psychometric evaluation and measurement invariance of the Sexual and Relationship Distress Scale in cancer and nonclinical general reproductive-age populations
Yanfei Jin, Yang Li, Lina Xiong, Chulei Tang, Hongwen Ma

TL;DR
This study translated and validated a Chinese version of the Sexual and Relationship Distress Scale, showing it works well for cancer patients and general populations.
Contribution
The study provides the first evidence of measurement invariance of the SaRDS across cancer patients, nonclinical populations, and gender groups.
Findings
The Chinese SaRDS has good convergent validity, reliability, and criterion-related validity.
Measurement invariance was confirmed across clinical cancer and nonclinical populations, as well as gender groups.
The 14 domains of the SaRDS enable targeted assessment of distress areas in sexual and relationship dysfunction.
Abstract
The Sexual and Relationship Distress Scale (SaRDS) is a validated instrument developed in English to assess intra-personal and inter-personal distress experienced by individuals and their partners in the context of sexual dysfunction. However, it has not yet been translated into Chinese nor psychometrically evaluated within Chinese clinical cancer and nonclinical populations. This study aimed to translate the SaRDS into Chinese and assess its psychometric properties and measurement invariance across different populations (colorectal cancer [CRC] patients vs. nonclinical general reproductive-age adults) and across gender groups (male vs. female). Three phases were undertaken: (a) transcultural adaptation, (b) pre-testing, and (c) psychometric evaluation. Transcultural adaptation included translations and expert panels, the pre-testing was conducted in 20 participants. The psychometric…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
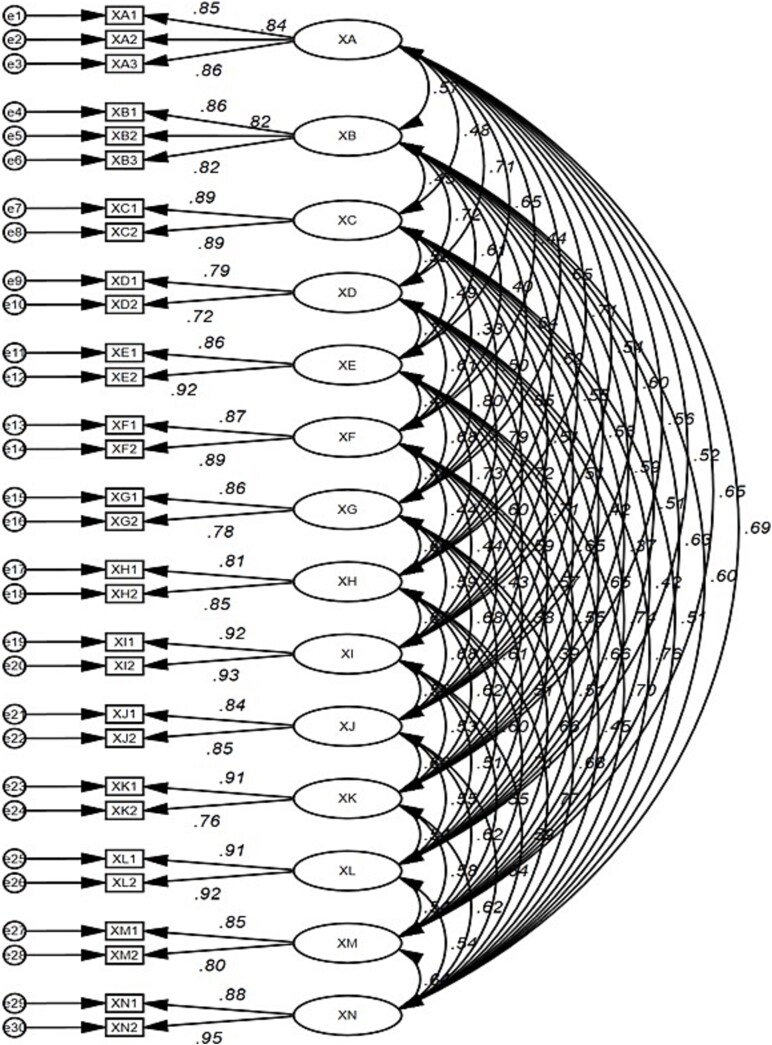 Figure 1
Figure 1|
|
|
|
|---|---|---|
|
| 37.124 ± 3.1110 | 34.978 ± 4.970 |
| Gender | ||
| Male | 287 (59.05) | 214 (39.93) |
| Female | 199 (40.95) | 322 (60.07) |
|
| ||
| Primary or blew | 45 (9.26) | 109 (20.34) |
| Junior high school | 155 (31.89) | 176 (32.84) |
| Senior high school | 196 (40.33) | 181 (33.77) |
| College and above | 90 (18.52) | 70 (13.06) |
|
| ||
| Primary or blew | 83 (17.08) | 73 (13.62) |
| Junior high school | 176 (36.21) | 167 (31.16) |
| Senior high school | 148 (30.45) | 210 (39.18) |
| College and above | 79 (16.26) | 86 (16.04) |
|
| ||
| <3000 | 104 (21.40) | 135 (25.19) |
| 3001-5000 | 296 (60.91) | 244 (45.52) |
| >5000 | 86 (17.70) | 157 (29.29) |
|
| ||
| Rural | 306 (62.96) | |
| City | 180 (37.04) | |
|
| ||
| None | 75 (15.43) | |
| ≥1 | 411 (84.57) | |
|
| ||
| Yes | 58 (11.93) | |
| No | 428 (88.07) | |
|
| ||
| Yes | 327 (67.28) | |
| No | 159 (32.72) | |
|
| ||
| Yes | 321 (66.05) | |
| No | 165 (33.95) | |
|
| ||
| Yes | 132 (27.16) | |
| No | 354 (72.84) | |
|
| ||
| Yes | 198 (40.74) | |
| No | 288 (59.26) | |
|
|
|
|
|
|
|
|---|---|---|---|---|---|
| 1. Anxiety | 1 | 11.64 | 4.44 | 12.84 | <.001 |
| 2 | 8.66 | 2.88 | |||
| 2. Conflict | 1 | 12.00 | 4.03 | 15.24 | <.001 |
| 2 | 8.66 | 2.92 | |||
| 3. Initiation | 1 | 8.21 | 3.19 | 13.32 | <.001 |
| 2 | 6.01 | 2.03 | |||
| 4. Guilt | 1 | 8.21 | 2.71 | 14.70 | <.001 |
| 2 | 6.13 | 1.75 | |||
| 5. Infidelity | 1 | 8.74 | 2.54 | 23.31 | <.001 |
| 2 | 5.45 | 1.96 | |||
| 6. Security | 1 | 8.12 | 3.23 | 11.74 | <.001 |
| 2 | 6.17 | 1.97 | |||
| 7. Predictability | 1 | 8.76 | 2.68 | 18.18 | <.001 |
| 2 | 6.20 | 1.78 | |||
| 8. Communication | 1 | 8.92 | 2.46 | 23.46 | <.001 |
| 2 | 5.72 | 1.89 | |||
| 9. Body image | 1 | 8.62 | 3.14 | 16.01 | <.001 |
| 2 | 6.00 | 2.02 | |||
| 10. Physical affection | 1 | 7.78 | 3.34 | 11.31 | <.001 |
| 2 | 5.84 | 2.04 | |||
| 11. Hopelessness | 1 | 8.27 | 3.18 | 11.35 | <.001 |
| 2 | 6.46 | 1.78 | |||
| 12. Self-esteem | 1 | 8.21 | 3.29 | 11.95 | <.001 |
| 2 | 6.16 | 2.11 | |||
| 13. Normalness | 1 | 8.72 | 2.97 | 16.62 | <.001 |
| 2 | 6.10 | 2.01 | |||
| 14. Relationship quality | 1 | 8.95 | 2.98 | 17.44 | <.001 |
| 2 | 6.12 | 2.18 | |||
| Total score | 1 | 125.15 | 28.22 | 22.91 | <.001 |
| 2 | 89.69 | 20.16 |
|
|
|
|
|
|
|
|---|---|---|---|---|---|
| 1. I worry about sex even when I am not with my partner | Anxiety | 0.848 | <.001 | 0.886 | 0.722 |
| 2. I feel anxious when I think about our sexual relationship | 0.838 | <.001 | |||
| 3. I am stressed about sex | 0.863 | ||||
| 4. My partner and I get angry with each other | Conflict | 0.858 | <.001 | 0.871 | 0.693 |
| 5. My partner and I regularly argue | 0.820 | <.001 | |||
| 6. My partner and I get annoyed with each other over little things | 0.819 | ||||
| 7. I do not initiate sex with my partner anymore | Initiation | 0.887 | <.001 | 0.881 | 0.787 |
| 8. I rarely bother to approach my partner for sex | 0.887 | ||||
| 9. I feel guilty because I cannot sexually satisfy my partner | Guilt | 0.789 | <.001 | 0.729 | 0.574 |
| 10. I feel guilty for letting my partner down | 0.725 | ||||
| 11. I am worried that my partner has been unfaithful | Infidelity | 0.865 | <.001 | 0.887 | 0.797 |
| 12. I am worried that my partner will be unfaithful | 0.920 | ||||
| 13. I feel undesirable to my partner | Security | 0.870 | <.001 | 0.872 | 0.773 |
| 14. I feel unattractive to my partner | 0.889 | ||||
| 15. Our sex is routine or predictable | Predictability | 0.859 | <.001 | 0.803 | 0.671 |
| 16. There is not much variety when we have sex | 0.778 | ||||
| 17. My partner and I do not talk about sex | Communication | 0.809 | <.001 | 0.815 | 0.689 |
| 18. I avoid talking about sex with my partner | 0.850 | ||||
| 19. I am worried that our relationship might end | Body image | 0.922 | <.001 | 0.923 | 0.857 |
| 20. I am questioning the strength of our relationship | 0.930 | ||||
| 21. We don’t hug and kiss as much as we used to | Physical affection | 0.843 | <.001 | 0.835 | 0.716 |
| 22. We are not as physically affectionate as we used to be | 0.849 | ||||
| 23. I wish more effort was made to fix our sexual problems | Hopelessness | 0.914 | <.001 | 0.829 | 0.709 |
| 24. I feel frustrated that I can’t fix our sexual problems | 0.764 | ||||
| 25. I have lower confidence because of our sexual problems | Self-esteem | 0.909 | <.001 | 0.911 | 0.837 |
| 26. I have lower self-esteem because of our sexual problems | 0.920 | ||||
| 27. My relationship has become more like a friendship | Normalness | 0.846 | <.001 | 0.810 | 0.681 |
| 28. My partner and I feel more like flat mates or colleagues | 0.804 | ||||
| 29. I worry there is something wrong with me sexually | Relationship quality | 0.876 | <.001 | 0.910 | 0.835 |
| 30. I do not feel normal when I compare myself sexually to others | 0.950 | <.001 |
|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| 1. Configural invariance | 970.342 | 628 | 0.980 | 0.972 | 0.033 | |||
| 2. Metric invariance | 980.998 | 644 | 0.979 | 0.973 | 0.034 | 10.657 | 16 | .830 |
| 3. Scalar invariance | 1119.763 | 660 | 0.973 | 0.964 | 0.037 | 149.421 | 32 | .000 |
|
| ||||||||
| 1. Configural invariance | 1114.435 | 628 | 0.977 | 0.968 | 0.039 | |||
| 2. Metric invariance | 1137.120 | 644 | 0.978 | 0.969 | 0.038 | 22.685 | 16 | .122 |
| 3. Scalar invariance | 1119.763 | 660 | 0.981 | 0.970 | 0.036 | 12.358 | 16 | .719 |
|
|
|
|
|
|---|---|---|---|
| SaRDS | .230*** | −.625*** | 0.865 |
| 1. Anxiety | 0.870 | ||
| 2. Conflict | 0.881 | ||
| 3. Initiation | 0.702 | ||
| 4. Guilt | 0.892 | ||
| 5. Infidelity | 0.885 | ||
| 6. Security | 0.798 | ||
| 7. Predictability | 0.711 | ||
| 8. Communication | 0.813 | ||
| 9. Body image | 0.925 | ||
| 10. Physical affection | 0.833 | ||
| 11. Hopelessness | 0.806 | ||
| 12. Self-esteem | 0.912 | ||
| 13. Normalness | 0.810 | ||
| 14. Relationship quality | 0.958 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Sexual function and dysfunction studies · Attachment and Relationship Dynamics
Introduction
Personal distress is a necessary condition to diagnose most mental health problems in clinical practice. To make a diagnosis, it is required that there should be not only the presentation of a series of corresponding symptoms and signs but also the individual’s experience of distress to accompany these symptoms and signs.1 Sexual dysfunctions (eg, female genito-pelvic pain/penetration disorder, male erectile disorder/premature ejaculation, etc.) constitute a spectrum of sexual function problems whose core characteristic is the experience of sexual distress alongside sexual functioning. Therefore, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), makes the presence of “clinically significant distress” central to the definition and diagnosis of sexual dysfunction.2
It is important to note that clinically significant distress associated with sexual dysfunction and sexual distress more broadly are related but distinct constructs. Clinically significant distress, as defined by DSM-5, specifically refers to the individual's distress directly linked to the presence and perceived severity of sexual dysfunction symptoms, and it is a requisite criterion for diagnosing sexual dysfunction. In contrast, sexual distress can include a wide range of negative emotional experiences related to sexuality, intimacy, and relational contexts, which may or may not directly result from specific sexual dysfunction symptoms.
Sexual distress is one of the most important factors in the etiology, maintenance, and treatment of sexual dysfunction. Neglecting sexual distress may lead to inaccurate measurement of sexual dysfunction, and reduction in functional symptoms alone is not sufficient to reduce individual distress about sexual dysfunction. However, not all studies have considered sexual distress caused by sexual dysfunction, which is not only reflected in the fact that many researchers have not strictly distinguished between sexually impaired function (distress is not present) and sexual dysfunction (both impaired function and distress are present) according to the requirements of the DSM,3 but also in the lack of tools to measure sexual distress. Measures that assess sexual distress in a comprehensive, valid, and precise manner are necessary to evaluate and compare sexual outcomes and to develop interventions for those who experience or are at risk for sexual dysfunction. Indeed, the need for high-quality patient-reported outcome measures (PROMs) of sexual distress has been repeatedly emphasized by relevant international sexual function research panels and society.4^,^5
Sexual functioning occurs most commonly in a dyadic context. According to the interdependence theory, individuals influence each other’s experiences (emotions, motivations, behaviors, and outcomes) through interactions.6 This theory emphasizes that relationship factors and processes play a crucial role in the quality of sexual response. Being in a partnership appears to be an important factor in explaining the presence of distress from sexual dysfunction.7 Still, the relational context has historically been ignored by most research on the causes and treatments of sexual dysfunction. Research has confirmed that relationship is one of the strongest predictors of sexual distress, meaning that individuals with high relationship satisfaction experience lower levels of sexual distress.8^,^9 Moreover, in intervention studies, there is evidence to suggest that taking a couples approach to the treatment of sexual dysfunction is beneficial and relationship satisfaction is a significant moderator of sexual distress.10^,^11 Given that impaired sexual function has historically been difficult to treat, reducing sexual distress alone may be an achievable treatment goal that is effective in promoting sexual outcomes.12 Thus, it is important to develop a measure of sexual distress that both members of the couple can use in research and clinical settings.
Previously, due to a lack of attention to sexual distress at both intra-personal and inter-personal levels, there were limited measurement tools for sexual and relationship distress, with the only available and validated tool being the Sexual Desire and Relationship Distress Scale (SDRDS).13 However, the SDRDS is only specifically applicable to women with low sexual desire. To expand sexual distress from the intra-personal to the relationship level, Frost and Donovan constructed the Sexual and Relationship Distress Scale (SaRDS) to accurately capture both the intra-personal and inter-personal distress experienced by individuals in a relationship partner with sexual dysfunction.14 The SaRDS includes multiple dimensions to quantify different types of distress; while also can use a total score to provide more information on the outcome efficacy. It was developed rigorously and has shown acceptable internal consistency, convergent validity, discriminant validity, and construct validity.
Given that clinically significant distress associated with sexual dysfunction is central to the diagnosis and clinical management of sexual dysfunction, and recognizing the broader role that sexual and relationship distress play in affecting sexual outcomes, we believe that effective measurement of these forms of distress is of great significance. To our knowledge, there is currently no comprehensive, valid, and reliable instrument in China capable of capturing sexual and relationship distress simultaneously among adult men and women. To promote clinical research and practice addressing sexual dysfunction and related distress in China, the current study aimed to translate the SaRDS into Chinese and evaluate its psychometric properties among Chinese adults.
As the third largest cancer in the world, colorectal cancer (CRC) has a unique treatment combination of abdominoperineal resection, pelvic radiotherapy, and chemotherapy, which significantly increases the incidence and severity of sexual dysfunction in CRC patients compared to other cancer types.15–17 Notably, the incidence of CRC among reproductive-aged adults (15–49 years old) is increasing rapidly.18^,^19 Compared with elderly CRC patients and normal peers, patients of reproductive age face more severe challenges, with more than 50% of CRC patients of reproductive age reporting that sexual dysfunction had a serious negative impact on their own and their partners’ intimate relationships and quality of life.15^,^20
Aims
Therefore, it is crucial to develop and validate instruments that can reliably assess sexual and relationship distress across diverse populations and genders. To verify the broad applicability and robustness of the SaRDS, the overall objective of the present study was to evaluate the psychometric properties and measurement invariance of the Chinese version of the SaRDS among CRC patients and nonclinical reproductive-aged adults, and across gender groups. Specifically, this study aimed to address two primary research questions: (1) Does the Chinese version of the SaRDS demonstrate adequate psychometric properties (validity and reliability) among CRC patients and nonclinical reproductive-aged adults? (2) Does the Chinese version of the SaRDS exhibit measurement invariance across population groups (CRC patients vs. nonclinical reproductive-aged adults) and across gender groups (male vs. female)?
Methods
Design
This study was designed as a cross-sectional survey and three distinct phases were undertaken: (1) transcultural adaptation, (2) pre-testing, and (3) psychometric evaluation. The reporting of this study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, and a completed STROBE checklist has been submitted with this manuscript.
Phase 1: Transcultural adaptation
The standardization procedure of the transcultural adaptation was guided by the World Health Organization’s Process of Translation and Adaptation of Instrument.
Forward translation
Permission to translate and validate the SaRDS was obtained from the copyright holder. Forward translation of the SaRDS was separately delegated to two bilingual translators to translate the original SaRDS from English to Chinese. Both of them had a medical background, one translator was aware of the purpose of the SaRDS translation, whereas the other was not. After the two translators finished the initial translation, item discrepancies between the two versions were identified and resolved, and the two versions were merged into a single version.
Backward translation
Subsequently, another two bilingual translators (who were unaware of the study’s purposes and measures) did a back translation from the Chinese version of the SaRDS into English. The back-translated version was remarkably similar to the original SaRDS. Then, the pre-final version was developed.
Expert panels
Five psychologists served as the expert group that assessed the SaRDS in its pre-final form. Three questions were addressed, namely: (1) Is the Chinese word that has been translated exactly the same as the English word? (2) Is there a better Chinese word to utilize as an alternative if the translated word is not exactly the same? (3) How likely is it that those who speak Chinese and fill out the questionnaire will be able to understand the substitute word that is selected? The purpose of this step is to review discrepancies in the meanings of the scale items and evaluate the cultural and linguistic equivalence of each item until a consensus is achieved.
The face validity and content validity of the SaRDS were then assessed by a second expert panel, which was made up of three sexual and reproductive doctors, three associate professors, and four nursing specialists. Wording, grammar, and item placement were used to evaluate face validity, while a Content Validity Index (CVI) was used to evaluate content validity. The CVI was completed by the item relevance ratings (1 = not relevant; 4 = highly relevant) of the expert panel,21 which included content validity scores for each item-level (I-CVI) and a scale-level CVI/average (S-CVI/Ave). The I-CVI is the proportion of experts who rate an item as relevant, whereas the S-CVI/Ave is the proportion of items rated as relevant by all raters. For a scale to be judged as having excellent content validity, it should contain only items with an I-CVI of ≥.78 and a S-CVI/Ave of ≥.90.22
Phase 2: Pre-testing
The pre-final version was pre-tested in 20 participants (10 CRC and 10 nonclinical general reproductive-age adults each). The inclusion criteria for patients were as follows: (1) Diagnosed with CRC, with a duration of at least 3 months after surgery; (2) aged 18-49 and married, (3) were able to complete the questionnaire independently, and (4) were willing to participate. The inclusion criteria for nonclinical populations were as follows: (1) Aged 18-49 and married, (2) were able to complete the questionnaire independently, and (3) were willing to participate. The exclusion criteria for both CRC patients and nonclinical populations were cognitive or psychiatric impairments and suffering from severe heart, liver, kidney, and other serious complications. Participants were asked to comment on their understanding of the wording and report on the clarity of the items.
Phase 3: Psychometric evaluation
Setting and participants
The CRC and nonclinical general reproductive-age populations were recruited from tertiary hospitals and communities in Tianjin and Jiangxi, China, from March 2024 to June 2024, respectively. The inclusion and exclusion criteria for participants are the same as those for pre-testing.
Measures
Demographics and clinical information
Demographic and clinical information were obtained from the participants using a questionnaire designed by the researcher that yielded information about age, gender, education, marital status, number of children, and clinical relevance.
The SaRDS
The SaRDS is a 30-item, 14-factor PROM of individual and relationship distress within the context of sexual dysfunction.14 All items are rated on a 7-point Likert scale (“not at all true” to “completely true”). The total scores range from 0 to 180 and reflect the standard of individual and relationship distress within the context of sexual dysfunction, with high values indicating more distress. In the original version of the study, the SaRDS showed good psychometric properties, and the subsequent studies also reported the strong internal consistency of the SaRDS (Cronbach α = .95 for the total score with individual subscales ranging from .70 to .96).
The Arizona Sexual Experience Scale
The Arizona Sexual Experience Scale (ASEX) is a 5-item scale that quantifies sex drive, arousal, vaginal lubrication/penile erection, ability to reach orgasm, and satisfaction from orgasm.23 All items are rated on a 6-point Likert scale (“extremely strong” to “no sex drive”). Total scores range from 5 to 30, and higher scores denote more sexual dysfunction. The internal consistency of the Chinese version of ASEX was α = .855.
The Quality of Relationship Index
The Quality of Relationship Index (QRI) is a 6-item measure to assess the quality of relationships in married and cohabiting couples.24 All items are rated on a 7-point Likert scale (“extremely dissatisfied” to “extremely satisfied”). The total scores range from 7 to 42, and higher scores denote greater relationship satisfaction. The internal consistency of the Chinese version of QRI was α = .782.
Data collection
The research team consists of an associate professor as the leader, two master students, and two registered nurses as research assistants, all of whom have been systematically trained. Recruitment was conducted by research members who approached the potential participants when they entered the hospitals (outpatient or inpatient departments) and communities. In both locations, research members presented the content and purpose of the research to potential participants, assessed them to determine whether they met the inclusion and exclusion criteria, and assured that participation was voluntary. After obtaining written consent, the researcher distributed the questionnaires to the participants. Once they completed the questionnaire, the researcher immediately checked their questionnaire to ensure the integrity of the data. If there were missing values, the questionnaires were returned to the participants so that they could fill in the missing items. Generally, the questionnaires were completed within 10–15 min.
Ethical considerations
This study was approved by the Institutional Review Board of Nanjing Medical University (Ethics No. 2024-749). All participants provided written informed consent prior to participation, and they were explicitly informed of their right to withdraw from the study at any point without any prejudice or consequences.
Statistical analyses
The data analysis was performed using IBM SPSS Statistics Version 26.0 (IBM Corp., Armonk, NY, USA) and Analysis of Moment Structure Version 23.0 (IBM Corp., Armonk, NY, USA).
First, descriptive statistics (frequency, percentages, means, and standard deviations) were used to describe the demographic characteristics of participants. Prior to conducting analyses, data were carefully screened for missing values. In our dataset, the proportion of missing data was very small (<5% per variable), and the missing pattern appeared completely at random (MCAR). Therefore, missing data were handled using expectation–maximization imputation, which is considered a robust and recommended method for addressing missing values under the assumption of MCAR.
Confirmatory factor analysis (CFA) was used as a critical step in refining the instrument and identifying the factorial structure of individual and relationship distress within the context of sexual dysfunction in the SaRDS. The CFA was conducted using the Maximum Likelihood estimation method, which is the most widely used method for parameter estimation in CFA due to its robustness and accuracy when data meet assumptions of approximate multivariate normality. Four fit indices were employed to examine the adequacy of model fit: a Chi-square to degrees of freedom ratio (χ^2^/df < 3), the comparative fit index (CFI ≥ 0.90), the Tucker–Lewis index (TLI ≥ 0.90), and the root mean square error of approximation (RMSEA ≤ 0.05).25 In CFA, the convergent validity of the SaRDS was verified through the factor loading of each item (≥0.50),26 the composite reliability (CR) value (≥0.70), and the average variance extracted (AVE) of the 14 factors (≥0.50).27
Then, to establish whether the 14-factor model is stable and can be replicated across different groups (CRC and nonclinical general populations), measurement invariance was further evaluated using multiple-group CFA. To examine whether the 14-factor model structure of the SaRDS is stable and replicable across different populations (CRC patients vs. nonclinical general populations) and across gender groups (male vs. female), we conducted multi-group CFA to systematically evaluate measurement invariance. The significance test of the change in Chi-square for two nested models was evaluated as a criterion for measurement invariance. If the Chi-square is not significant, it is determined that factor loadings are equivalent and thus evidence of weak metric invariance and scalar invariance.28
Furthermore, criterion-related validity was measured by the Pearson correlation between SaRDS and ASEX and the Pearson correlation between SaRDS and QRI, respectively. Last, to evaluate the internal consistency of the SaRDS, Cronbach’s α was measured. Internal consistency was considered adequate when α ≥ .70.29
Result
Phase 1: Transcultural adaptation
Forward translation
In the step of forward translation, the English version was translated into Chinese. The two translators only had discrepancies in the translation of the two items under “Dimension 6: Security” and reached an agreement after discussion.
Backward translation
In the step of backward translation, the Chinese version was translated back into English. The back-translated version was remarkably similar to the original SaRDS.
Expert panels
The first expert panel unanimously approved the translation and original review of SaRDS. However, the experts thought that items 13 and 14 were ambiguous, so the wording of items 13 and 14 was modified after discussion. In addition, the experts thought that item 15 was difficult to understand, so item 15 was also appropriately modified. In the second panel, the 10 experts gave their comments on the scale and rated each item’s understandability, clarity, sensitivity, and relevance. The I-CVIs ranged from 0.87 to 1.00, and the calculated S-CVI was 0.95, indicating that the SaRDS content was valid.
Phase 2: Pre-testing
In this step, some patients pointed out that the description of item 20 was unclear. After discussion, the wording of item 20 was modified. After the revision, the 20 participants reported that all items were clear, understandable, and acceptable. Thus, the final Chinese version of the SaRDS was generated (The 30 SaRDS items (English and Chinese versions) are available in Supplementary Table S1).
Phase 3: Psychometric evaluation
Sample characteristics
Of the 1211 potential participants that were approached, 104 did not meet the inclusion criteria, 64 declined to participate for various reasons, and 1043 were eligible for the study and consented to participate. Finally, 1022 remained (486 CRC and 536 nonclinical general population) after the invalid questionnaires were removed, with no missing values. Characteristics of the participants are presented in Table 1, and descriptive statistics of SaRDS in the CRC and nonclinical general reproductive-age populations are presented in Table 2.
Confirmatory factor analysis
The CFA model with 14 latent subscales demonstrated an adequate fit across multiple fit indices. Final fit statistics were all optimal as follows: Chi-square (χ^2^/df = 2.496, P < .001), TLI = 0.971, CFI = 0.979, RMSEA = 0.037. Figure 1 shows the results of the factor structure and model fit of the SaRDS using CFA.
Factor structure of the refined model of the SaRDS. XA = anxiety; XB = conflict; XC = initiation; XD = guilt; XE = infidelity; XF = security; XG = predictability; XH = communication; XI = body image; XJ = physical affection; XK = hopelessness; XL = self-esteem; XM = normalness; XN = relationship quality; SaRDS = Sexual and Relationship Distress Scale.
The convergent validity of the SaRDS was examined by CFA as well as AVE and CR. The results showed that the factor loadings of all items ranged from 0.725 to 0.950, the AVE values of 14 factors ranged from 0.574 to 0.857, and the CR values ranged from 0.729 to 0.923. As described earlier, all of the criteria displayed good acceptability, supporting that the SaRDS has satisfactory convergent validity (Table 3).
Furthermore, we conducted multi-group confirmatory factor analyses to examine the measurement invariance of the SaRDS across different population groups and gender groups. As shown in Table 4, all tested invariance models exhibited moderate-to-good fit indices. Specifically, the SaRDS demonstrated satisfactory configural, metric, and scalar invariance both across different population groups and across gender groups. These findings indicate that the factor structure, factor loadings, and item intercepts of the SaRDS are equivalent across populations and genders, supporting the robustness and generalizability of the scale.
Criterion-related validity
We used ASEX and QRI as gold standards to test the criterion-related validity of SaRDS. The results showed that SaRDS had a significant weak positive correlation with ASEX (r = 0.230, P < .001); and a significant moderate negative correlation with QRI (r = −0.625, P < .001), indicating adequate criterion-related validity of the SaRDS (Table 5).
Internal consistency
To determine internal consistency, Cronbach’s α values were calculated individually for the subscales of the SaRDS. Cronbach’s α values for the 14 subscales ranged from .702 to .958, indicating that the SaRDS has good internal consistency (Table 5).
Discussion
Given the growing body of research viewing distress from sexual dysfunction as an issue that often exists within the context of a relationship, an adequate tool for measuring sexual and relationship distress is of great significance. This study translated the SaRDS into Chinese and evaluated the psychometric properties of the Chinese version of the SaRDS in both CRC and nonclinical reproductive-age samples in China. The translation of SaRDS in this study involves two languages from different linguistic groups. The source language was English, which belongs to Indo-European, while the target language was Chinese, a Sino-Tibetan language. Due to the huge differences in cultural background, these two languages differ semantically, morphologically, and syntactically.30 Factors such as cultural context, emotionality, untranslatability, and translators need to be considered in cross-language translation.31 In this study, we strictly followed the guidance of the World Health Organization’s Process of Translation and Adaptation of Instruments to minimize the impact of the aforementioned factors. Through the translation–back translation process, evaluation by expert panels, and pre-testing, we translated the SaRDS into Chinese with functional equivalence to the original text.
In this study, the translated Chinese version of SaRDS was tested for content validity and face validity in expert panels, and the results showed that the Chinese version of SaRDS was valid and reliable with strong consistency. In the pre-testing, the Chinese version of SaRDS demonstrated good feasibility and took participants about 5 min to complete, suggesting its low response burden. In the psychometric evaluation, this study recruited the CRC and nonclinical general populations. The scores of the CRC population on the 14 subscales and the total score were significantly higher than those of the nonclinical general population, suggesting that the combination treatment of CRC indeed increases the incidence and severity of sexual dysfunction in CRC reproductive-age patients, with a corresponding increase in sexual distress at the intra-personal and relationship levels. In addition, compared with the English version of SaRDS,14 the scores of the Chinese nonclinical general population were slightly higher than those of the Australian nonclinical general population. The variations in SaRDS scores between our and previous study may be due to differences in the characteristics of the study samples: the samples in the original SaRDS study were all community-based and skewed toward highly educated and high-functioning individuals.
The CFA showed that the Chinese version of SaRDS contained 14 factors, consistent with the English version of SaRDS. Sexual distress is multi-dimensional and reflects multiple types of distress.32 The subscales of the SaRDS cover both intra-personal distress as well as inter-personal distress, including negative cognitions of self (self-esteem, body image, and normalness), negative cognitions of their relationship (security, infidelity, predictability, and relationship quality), inter-personal distress (anxiety, guilt, and hopelessness), and behavioral change in the relationship (conflict, initiation, communication, and physical affection), which provides more extensive information than previous scales with only total scores, such as the SDRDS13 and the Female Sexual Distress Scale-Revised.33 Since sexual function most often occurs in a dyadic context, relationship factors and processes play a role in sexual outcome,7 which suggests that when measuring the distress caused by sexual dysfunction, it is not comprehensive to focus only on the distress at the intra-personal level, and the relationship level also should be considered.
Furthermore, to determine whether the 14-factor structure of the SaRDS is stable and equivalent across different populations and genders, we conducted multi-group confirmatory factor analyses evaluating measurement invariance. Our findings indicated that the SaRDS exhibited satisfactory configural, metric, and scalar invariance across both CRC and nonclinical general populations, as well as across gender groups (male vs. female). These results demonstrate that the factor structure, item loadings, and item intercepts are consistent and meaningful across populations and genders. Thus, the SaRDS can reliably be applied to assess and meaningfully compare sexual and relationship distress across cancer patients, general populations, and across male and female respondents, further supporting its broad utility and robustness as a psychometric tool.
To assess criterion-related validity, the SaRDS was correlated with both the ASEX and QRI, as they are current gold standard measures of sexual distress and relationship satisfaction. The SaRDS had a positive correlation with ASEX and a negative correlation with QRI, which is consistent with the findings in the English version of the SaRDS. As expected, the SaRDS was significantly correlated with existing measures of sexual and relationship distress, indicating that SaRDS is reliable. Finally, the α value of the Chinese version of the SaRDS was .865, and the α values of the 14 subscales were above .70, indicating good internal consistency.
However, it is important to acknowledge that the correlation between the SaRDS and ASEX in our study was relatively weak (r = .230). One plausible explanation for this modest correlation is that the two instruments measure related yet distinct constructs. Specifically, the ASEX primarily evaluates the severity of sexual dysfunction symptoms and associated clinical distress directly linked to these symptoms, whereas the SaRDS assesses broader dimensions of sexual and relationship distress, encompassing emotional and relational aspects that extend beyond specific sexual dysfunction symptoms. Previous research has consistently highlighted that sexual distress involves emotional experiences related to intimacy, relationship dynamics, and subjective perceptions of one's sexuality, which may not always align closely with measures focused solely on symptom severity of sexual dysfunction.34 Therefore, the moderate-to-low correlation observed in our study likely reflects conceptual differences between these two instruments rather than a limitation inherent to the SaRDS itself. Future research is needed to further elucidate the nuanced relationship between the severity of sexual symptoms and broader sexual and relationship distress constructs.
Study limitations
Although our findings provide important support for the psychometric properties of the Chinese version of SaRDS, some methodological limitations may reduce its scope for general applicability. First, we gathered the sample exclusively in the urban areas of Tianjin and Jiangxi, and the clinical samples were only from the CRC population, so whether the results may be generalizable to other locations in China and other clinical samples needs further exploration; a larger and more diverse sample is needed in future research. Second, regarding the validation method, we did not perform test–retest reliability and sensitivity tests. Hence, future investigations should include further evaluation of the psychometric properties of the Chinese version. Third, this study only captured individuals’ responses and couldn’t reflect the sexual and relationship distress of partners. Future research should implement measurements of SaRDS for both members of a couple to determine whether scores can be combined to provide more information. Fourthly, our inclusion criteria restricted participation exclusively to married individuals, thereby excluding unmarried couples from the study. Considering that the original SaRDS was specifically calibrated for couples who had been in a relationship for at least 6 months, and that the QRI was developed primarily for married or cohabiting individuals, this decision to exclude unmarried couples may limit the broader generalizability of our findings. This limitation is particularly noteworthy given the increasing prevalence of stable, committed, and nonmarital relationships in contemporary Chinese society. Future research should therefore aim to include unmarried couples in stable, committed relationships (eg, cohabiting or long-term partnerships) to further enhance the applicability and external validity of the findings. Finally, clinicians should consider the impact of response bias when using SaRDS in applied settings, as individuals may not answer truthfully if they are concerned that their partners may view their answers. Therefore, ensuring that responses to individual items are kept confidential in the clinical context is critical.
Clinical implications
According to our findings, the Chinese version of the SaRDS is a valid and reliable instrument with robust psychometric properties for assessing individual and relationship distress related to sexual dysfunction in both clinical cancer and nonclinical general populations. Our analyses further demonstrated measurement invariance across different populations (cancer and general populations) and gender groups (male and female). This indicates that the SaRDS measures the same underlying constructs in a consistent manner across diverse groups, allowing clinicians to confidently interpret and compare scores regardless of population type or gender. The 14 domains identified by the SaRDS provide clinicians with detailed and practical insights, enabling more accurate and personalized interventions for individuals and couples experiencing sexual and relationship distress.
Conclusion
This study translated the SaRDS into Chinese and comprehensively evaluated its psychometric properties and measurement invariance. Our findings demonstrated that the Chinese version of the SaRDS exhibits strong reliability, validity, and responsiveness in non-English-speaking contexts. Furthermore, multi-group confirmatory factor analyses supported the stability and measurement invariance of the SaRDS structure across clinical cancer and nonclinical general populations, as well as across gender groups. These results provide robust evidence that the SaRDS is a reliable and valid instrument for assessing sexual and relationship distress, enabling meaningful comparisons across different populations, genders, and within couples. Therefore, SaRDS can be confidently utilized in real-world clinical practice and research settings, facilitating accurate assessment and tailored interventions for individuals and couples experiencing sexual and relationship distress.
Supplementary Material
supporting_information_qfaf041
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pascoal PM, Raposo CF, Roberto MS. A transdiagnostic approach to sexual distress and sexual pleasure: a preliminary mediation study with repetitive negative thinking. Int J Environ Res Public Health. 2020;17(21):7864. 10.3390/ijerph 17217864 PMC 766370533121015 · doi ↗ · pubmed ↗
- 2First, M. B., American Psychiatric, A. 2022. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR, American Psychiatric Association Publishing, Edited by: American Psychiatric Association. 10.1176/appi.books.9780890425787 · doi ↗
- 3Parish SJ, Hahn SR. Hypoactive sexual desire disorder: a review of epidemiology, biopsychology, diagnosis, and treatment. Sex Med Rev. 2016;4(2):103–120. 10.1016/j.sxmr.2015.11.00927872021 · doi ↗ · pubmed ↗
- 4Kim NN, Goldstein I, Simon JA, Freedman MA, Parish SJ. ISSWSH special report on the US Food and Drug Administration draft guidance on low sexual desire and arousal: a new hope or old habits die hard? Sexual Medicine Reviews. 2017;5(2):131–134. 10.1016/j.sxmr.2017.01.00428343481 · doi ↗ · pubmed ↗
- 5Basson R, Berman J, Burnett A, et al. Report of the international consensus development conference on female sexual dysfunction: definitions and classifications. J Urol. 2000;163(3):888–893. 10.1016/S 0022-5347(05)67828-710688001 · doi ↗ · pubmed ↗
- 6Van Lange P, Rusbult C. Interdependence theory. In Van Lange PA, Kruglanski AW, Higgins ET, eds. Vol 2. SAGE Publications Ltd; 2012:251–272. 10.4135/9781446249222.n 39 · doi ↗
- 7Mccool-Myers M, Theurich M, Zuelke A, Knuettel H, Apfelbacher C. Predictors of female sexual dysfunction: a systematic review and qualitative analysis through gender inequality paradigms. BMC Womens Health. 2018;18(1):108. 10.1186/s 12905-018-0602-429929499 PMC 6013982 · doi ↗ · pubmed ↗
- 8Hamzehgardeshi Z, Sabetghadam S, Pourasghar M, Khani S, Moosazadeh M, Malary M. Prevalence and predictors of sexual distress in married reproductive-age women: a cross-sectional study from Iran. Health Sci Rep. 2023;6(9):e 1513. 10.1002/hsr 2.151337655267 PMC 10468024 · doi ↗ · pubmed ↗