Reporting the Impact of Pelvicalyceal System (PCS) Anatomy on Clinical Outcomes in Retrograde Intrarenal Surgery (RIRS) Studies: Can We Do Better? – Methodological Review from the Section of EAU Endourology
Ali Talyshinskii, Yerkebulan Mukhambetov, Ulanbek Zhanbyrbekuly, Lazaros Tzelves, Patrick Juliebø-Jones, Theodoros Tokas, Giorgio Bozzini, Wissam Kamal, Bhaskar Kumar Somani

TL;DR
This paper reviews studies on kidney stone surgery to see if they properly consider kidney anatomy, finding that important anatomical factors are often overlooked.
Contribution
The study identifies significant gaps in how pelvicalyceal anatomy is reported in RIRS clinical trials.
Findings
Only 8 out of 27 studies analyzed hydronephrosis in PCS anatomy.
Morphometric measurements were limited to the lower pole in 4 studies.
Key anatomical features like renal pelvis position and calyx orientation were not compared.
Abstract
To analyze available randomized clinical trials (RCTs) comparing retrograde intrarenal surgery (RIRS) with other modalities for urinary stone treatment to determine the extent of comparing the pelvicalyceal system (PCS) anatomy between patients. In December 2024, a search was conducted in databases and was limited to publications that describe comparisons of experimental and control groups in the context of RIRS for stones only in the kidney (PCS). Only RCTs comparing RIRS with other modalities without publication date restriction were included due to their highest level of evidence in the hierarchy of primary research. The parameters used in the selected studies were analyzed to compare the differences between the groups, focusing on PCS anatomy. The final analysis included 27 publications from 2421 articles. The presence and/or degree of hydronephrosis were analyzed in 8 studies.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1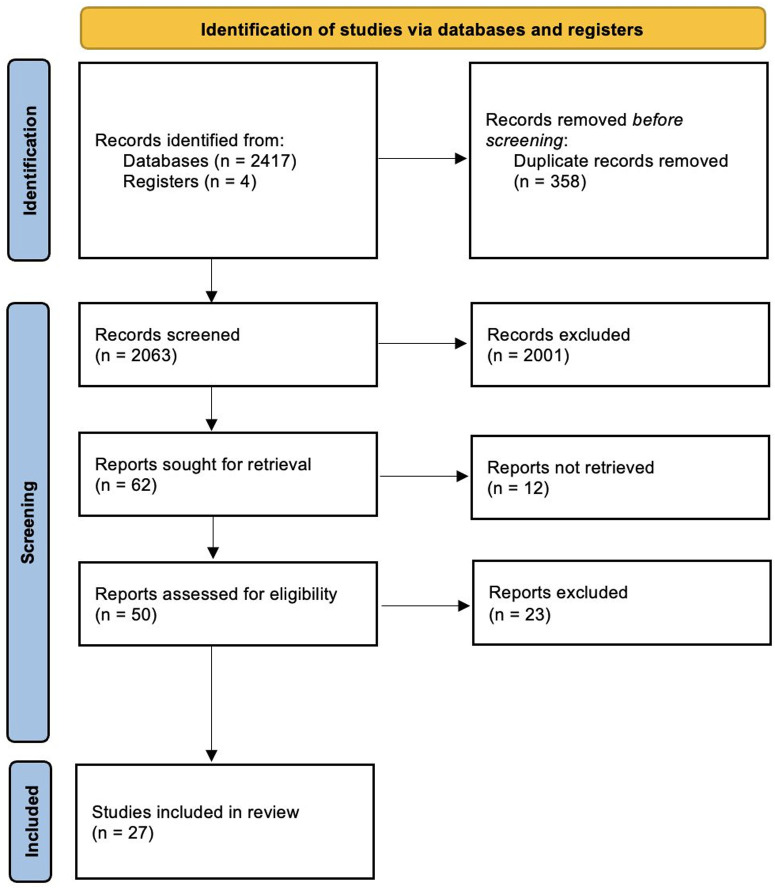 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Aortic aneurysm repair treatments · Advanced X-ray and CT Imaging
Introduction
Retrograde intrarenal surgery (RIRS) is integral to kidney stone treatment. Despite the constant modernization of flexible ureteroscopes and the expansion of their indications, many factors, including operator-related, intervention-related, and patient-related factors, contribute to the success of this procedure.1^,^2 The latter, in turn, are divided into modifiable and non-modifiable factors, which are not unique to RIRS and underlie medical practice as a whole.3 The pelvicalyceal system (PCS) is a highly variable anatomical zone and one of the non-modifiable factors, the analysis of which is fundamental in choosing a surgical strategy and predicting the success of treatment of renal calculi and associated complications.4 On the other hand, according to the latest guidelines, RIRS is recommended as a first-line approach when treating ≤2 cm stones, especially those located in the lower pole with unfavorable anatomy for extracorporeal shockwave lithotripsy (ESWL).5 Among primary studies, randomized controlled trials (RCTs) are the most reliable and determine the level of evidence for specific statements in clinical recommendations. Randomized controlled trials are based on the randomization of patients to minimize selection biases; therefore, special attention in all original studies is given to comparing various factors between groups.6 Despite the importance of this step, there is no attempt to analyze the methodology of RIRS-related RCTs, namely the comparison of patients’ PCS anatomy, before stating the absence of any differences between patients. Considering the above, the purpose of this methodological review is to analyze available RCTs comparing RIRS with other treatment modalities, to determine the extent of comparison of PCS anatomy between patients.
Materials and Methods
Search
In December 2024, a search was conducted in databases including PubMed, Google Scholar, Scopus, and clinicaltrials.gov using Boolean operators and the following search terms: “retrograde intrarenal surgery,” “RIRS,” “Flexible ureteroscopy,” “fURS,” and “Ureteroscopy.” The search was limited explicitly to publications that describe comparisons of experimental and control groups in the context of RIRS for stones only in the kidney (PCS).
Inclusion Criteria
We searched for English-language papers with full article accessibility, randomized studies, descriptions of pre-procedural set-up and preoperative imaging modalities used, and surgery-related metrics (stone-free rate (SFR), operative time, fluoroscopy time, complication rate, retreatment rate, auxiliary procedure rate). To reduce the search volume without losing the representativeness of the results, only RCTs comparing RIRS with other modalities without publication date restriction were included due to their highest level of evidence in the hierarchy of primary research.
Exclusion Criteria
Non-English written and inaccessible papers, non-RCTs and other study designs, and a lack of information about surgery-related metrics.
Studies Process
Two reviewers (A.T. and E.M.) independently identified all papers. All studies fitting the inclusion criteria were selected for full review. If there was a disagreement or discrepancy, the senior author (B.K.S.) made the final decision.
Data Extraction and Analysis
We analyzed the parameters used in the selected studies to compare the differences between the groups, focusing on PCS anatomy. These parameters were taken either from the “Materials and methods” section or related tables and grouped according to the specific characteristics of PCS as a whole or its separate compartments, namely: presence and/or stage of hydronephrosis, pelvic branching, and position (intrarenal, extrarenal) related to the parenchyma, whether a literature classification system was used, the number and orientation of minor calyces, the level of their grouping, and direct measurements (angles, length, width, etc.). The use of specialized nomograms was also analyzed based on the stone’s location in specific PCS. Finally, if there were any indications in the articles that the authors studied the anatomy of the PCS of recruited patients (e.g., exclusion of cases with anomalous kidneys, intraoperative characterization), then this fact was noted in a separate column in the table. The review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure transparency and comprehensive examination of the topic.
Results
Following the inclusion criteria in the literature search, the final analysis included 27 publications from 2421 articles (Figure 1). Among them, RIRS was compared only with ESWL, only with 1 percutaneous modality, with different percutaneous modalities, with both ESWL and a percutaneous modality, and in combination with other modalities in 5,9^,^12^,^14^,^15^,33^ 17,7^,^8^,^13^,^16^-^ 18^,^20^-^ 23^,^25^,^27^-32^ 1,^24^ 3,11^,^19^,^26 and 1^10^ studies, respectively (Table 1). 12 studies were focused on inferior pole calculi.9^,^11^,^12^,^17^-^ 20^,^21^,^23^,^24^,^30^,^33 The number of participants in the RIRS arm varied from 11 to 207.19^,26^ Pros and cons of RIRS over other modalities were found to be controversial. Operative time was better, non-inferior, or worse than ESWL or different percutaneous approaches in 0/3/3 and 5/10/4 studies, respectively. Fluoroscopy time was better, non-inferior, or worse in 1/0/1 and 8/1/1 studies. SFR rate was better, non-inferior, or worse in 5/3/0 and 1/12/8 studies.
According to the analysis, ultrasound (US), kidney-ureter-bladder (KUB) X-ray, intravenous urography (IVU), non-enhanced and enhanced computed tomography (CT) were preoperatively performed in 7, 6, 7, 21, and 5 studies, respectively (Table 2). Based on them, hydronephrosis presence and/or degree were analyzed in 8 studies. In 13 studies, authors compared stone localization between groups and indicated PCS compartments as pelvis, superior, middle, and inferior poles. Moreover, in 2 studies, authors compared the Seoul National University Renal Stone Complexity (S-reSC) scores between groups, which is also based on stone location in different PCS compartments.34 The authors investigated and excluded cases with anomalous kidney anatomy in 18 studies. In 1 study, authors excluded cases with unfavorable lower pole anatomy among patients with stones in this location; however, a direct comparison between the control and experimental groups was missed.19 Direct morphometric measurements were compared in 4 studies and were focused on the lower pole only, namely the infundibulopelvic angle (IPA), infundibular length (IL), and infundibular width (IW). Features such as the position of the renal pelvis in relation to the kidney parenchyma (intrarenal or extrarenal), the number and orientation of calyces, and the existing PCS classifications were not compared or used.
Discussion
Currently, endourological interventions have almost completely replaced open surgery in the treatment of kidney stone disease.35 Improved imaging techniques, instruments, and experience within the urological community have undoubtedly facilitated this.36 Many factors determine the outcome of the intervention and the reliability of the results obtained, such as sample size of patients,7 single-center performance,14 variability of equipment used in different centers,19 performance by the same operator,27 various types and timing of postoperative imaging,31 stone composition,9 and others. However, the specific characteristics of the patients themselves are also important, which directly influence potential differences between groups and may themselves determine the results obtained.13^,^16^,^29
The anatomy of any organ is a non-modifiable aspect, unlike other potential risk factors for failure during surgery. The importance of the surgical anatomy of the collecting system may favor 1 procedure over others, especially in the context of Mini PCNL and RIRS, when comparing results.31 According to this review, 25 studies (92.6%) generally investigated renal anatomy, and the remaining 2 articles assessed the treatment results of staghorn stones or isolated upper pole stones.10^,^32 In the latter study, the anatomical assessment would be helpful given the presence of upper-pole-based morphometric features and the possibility of visualizing the rest of the non-affected PCS, especially in the case of the presence of pelvic division into 2 or more separate branches.37
In most studies, the authors looked at the outcomes by excluding renal anomalies or abnormal renal anatomy (18, 66.7% papers). However, this leads to a slight bias in reporting and comparing studies. One study, when looking at the results of Mini PCNL and RIRS in the management of solitary 1-2 cm stones, found inferior SFR among lower pole calculi and attributed it to intraoperatively defined unfavorable factors like IPA, IW, and IL.^27^ Moreover, the study is 1 of 5 in which the authors preoperatively used contrast-enhanced CT.
Another feature of PCS anatomy is its division into compartments such as the pelvis, upper, middle, and lower poles to describe the location of the stone. Of 14 studies that analyzed endourological outcomes, 11 had this description, but none provided any details about the number and orientation of minor calyces. While this detailed characterization of the PCS could be time-consuming, it would help to understand the outcomes better. Also, considering the various movements and muscles of the wrist and hand, these factors can directly affect the ergonomics and results of RIRS.
Guglielmetti et al^38^ spoke about parameters extracted from CT that could predict renal calyceal access during PCNL, and the only independent predictive factor was the angle between the entrance calyx and the desired calyx. Ricapito et al^39^ stated that anterior and posterior accesses in supine PCNL offer similar safety and efficacy, and access is usually decided by surgeons when investigating PCS anatomy, which confirms subjectivity in this aspect and requires an objective comparison of at least anterior and posterior minor calyces between groups.
Despite the main focus of this review on RIRS, a significant part of the work was compared with percutaneous surgery. A potential solution to this problem was mentioned in 2 works, where the authors used the S-reSC when comparing patient characteristics. This is based on stone location coupled with the orientation of affected calyces using the frontal plane of the kidney.13^,^25 In turn, the problem of comparing the number of minor calyces is more evident in studies involving patients with multiple stones, especially within various locations. In the literature, controversies also exist on this question. Demirbas et al40 concluded that RIRS is a more effective and reliable procedure than PCNL, with higher SFRs and lower complication rates in treating multi-calyceal and multiple stones in the same renal unit. In contrast, Baran and Aykac stated the opposite opinion.41 As was shown by several included studies in this review, such a scenario is an independent risk factor for intervention failure.22^,^29 Despite this, such studies often lack clarification regarding the number and location of multiple stones. Only 1 study indicates different percentages of multiple stones and multiple localizations of stones, which directly confirms the hypothesis of the possibility of including patients with the same stone burden but different complexity in a single group.14
The next most common anatomical sign is the presence and/or grade of hydronephrosis. Wang et al^42^ showed that in the presence of severe hydronephrosis, the postoperative urinary sepsis rate in the RIRS group was as high as 15.4%, which was much higher than the 1.5% rate observed in the S-PCNL group. Ergani et al^44^ concluded that the success of FURS will decrease as the grade of hydronephrosis increases to grade 2 or more, whereas Özman et al^43^ reported the opposite results. These contradictions make it difficult to rule out the impact of hydronephrosis on endourological outcomes definitively. It seems prudent, therefore, to analyze this in future studies to clearly understand its effect on the results of RIRS outcomes. Among the analyzed studies, only 8 (29.6%) are provided with a comparison of hydronephrosis between groups, while 5 of these relate to studies related to lower pole calculi (41.7%). In an overwhelming 96.3% of studies (26/27), a pre-operative CT scan was used to determine the hydronephrosis grade. One study was conducted using US and IVU.^7^ Also, some studies argue that CT are not always needed for PCS anatomy, while others argue that they are helpful for anatomy and predicting outcomes.45^,^46
In addition to the qualitative characteristics mentioned earlier, there are also quantitative parameters for assessing PCS based on determining the IPA, IL, and IW. Only 4 of the included studies, all focusing on lower pole calculi, provided such a comparison between groups. However, the remaining 8 out of 12 studies (66.7%) did not include these features. Some studies acknowledged the lack of this data or correlation analysis.9^,^23 Another study used specific cut-offs for IPA, under 45 degrees, when comparing RIRS and ESWL for lower pole stones between 1 and 2 cm.^33^ However, they did not investigate IL and IW, which affected outcomes. Bozzini et al^19^ excluded cases with unfavorable lower pole anatomy (IPA <30°, IL >10 mm, and IW<5 mm), leaving their influence on results uncertain.
Some authors directly cite steep IPA for converting RIRS to percutaneous surgery. However, they do not have any direct measurements and are based only on their subjective opinion.8^,^20 According to other studies, the SFR following RIRS for managing lower pole calculi was worse than ultra-mini PCNL and mini PCNL.16^,^27 However, these studies did not compare anatomical factors and grade of hydronephrosis. Moreover, the RIRS group contained significantly more patients with multiple stones in 1 study.^16^
A recent meta-analysis demonstrated that IPA is an independent factor influencing the success of RIRS.47 However, the authors state that high heterogeneity characterizes the analyzed studies, partly due to different measurement approaches. All of the studies in this review that compare IPA between patients or use it to exclude patients with steep angles lack information regarding the measurement method used. Notably, these morphometric measurements extend beyond the lower poles, enabling the determination of angles between various calyceal levels. As was shown by Aminsharifi et al,^48^ significant hydronephrosis coupled with an upper calyx-lower calyx infundibular angle was associated with a greater likelihood of stone scattering, which could potentially affect the outcome of PCNL.
Finally, none of the studies used the different classifications of PCS based on its branching or division site related to the kidney parenchyma. Literature suggests that these factors are of prognostic significance. According to the Sampaio and Mandarim-De-Lacerda nomenclature,49 systems with crossed calyces draining the kidney midzone (type A2) showed lower accessibility to minor calyces during flexible ureteroscopy.50 Kirecci et al51 drew similar conclusions, finding that after RIRS, SFR was significantly lower in subgroup A2 (30.4%) and considerably higher in the subgroup with independent drainage of midzone calyces to the pelvis (type B2). Type A2 type also exhibited increased operative and fluoroscopy time.
To the authors’ knowledge, this is the first review to analyze PCS-related anatomical factors in randomized studies that compare RIRS with other endourological modalities. Most studies frequently overlook independent risk factors such as the anatomy of the PCS. While some exclude cases with abnormal anatomy and stone location, studies also missed the degree of hydronephrosis and morphometric measurements. Aspects such as pelvic division and branching, calyceal number, and orientation were missed despite data in the literature confirming their influence on RIRS outcomes. Among studies on lower pole calculi, only 4 of 12 compared the anatomy. Moreover, some authors use these parameters to exclude patients with unfavorable anatomy or associate it with conversion from RIRS to percutaneous surgery but fail to give objective measurements.
Future studies comparing or presenting data on outcomes of RIRS should use a standardized protocol for assessing PCS anatomy to highlight risk factors for surgical failure and reduce heterogeneity in the reporting of studies, as well as when conducting meta-analyses and updating the guidelines.
However, this review also has several limitations that should be mentioned. First, strict inclusion criteria were established, potentially leading to the omission of similar RCTs. Secondly, randomized studies were included regardless of blinding, which could affect study quality. Finally, other patient and stone-related features may also be varied among studies but were not analyzed here and should be investigated in future studies.
This review shows gaps in the literature while assessing and reporting on PCS anatomy in studies with RIRS. Essential factors such as pelvic division, branching patterns, and calyceal orientation are broadly not mentioned. Despite influencing procedural outcomes, the presence and degree of hydronephrosis and morphometric measurements are often missed. Unless studies mention these anatomical factors without excluding certain groups of patients, it is difficult to compare outcomes between modalities and in between studies. Standardized protocols for evaluating and reporting on PCS will improve reporting and comparison while helping clinicians make better treatment choices and informed decision-making with patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Akgül M Çakır H ÇinarÖ The efficacy and safety of retrograde intrarenal surgery: a multi-center experience of the RIR Search group study. J Urol Surg. 2023;10(2):119 128. (doi: 10.4274/jus.galenos.2023.2022.0039) · doi ↗
- 2Silva THCD Passerotti CC Pontes Júnior J Maximiano LF Otoch JP Cruz JASD. The learning curve for retrograde intrarenal surgery: a prospective analysis. Rev Col Bras Cir. 2022;49:e 20223264. (doi: 10.1590/0100-6991 e-20223264-en) PMC 1057885735946637 · doi ↗ · pubmed ↗
- 3Alwan NA Stannard S Berrington A Risk factors for ill health: how do we specify what is ‘modifiable’? P Lo S Glob Public Health. 2024;4(3):e 0002887. (doi: 10.1371/journal.pgph.0002887) PMC 1091160038437177 · doi ↗ · pubmed ↗
- 4Karim SS Hanna L Geraghty R Somani BK. Role of pelvicalyceal anatomy in the outcomes of retrograde intrarenal surgery (RIRS) for lower pole stones: outcomes with a systematic review of literature. Urolithiasis. 2020;48(3):263 270. (doi: 10.1007/s 00240-019-01150-0) 31372691 PMC 7220875 · doi ↗ · pubmed ↗
- 5Geraghty RM Davis NF Tzelves L Best practice in interventional management of urolithiasis: an update from the European Association of Urology guidelines panel for urolithiasis 2022. Eur Urol Focus. 2023;9(1):199 208. (doi: 10.1016/j.euf.2022.06.014) 35927160 · doi ↗ · pubmed ↗
- 6Kahan BC Rehal S Cro S. Risk of selection bias in randomised trials. Trials. 2015;16(1):405. (doi: 10.1186/s 13063-015-0920-x) PMC 456630126357929 · doi ↗ · pubmed ↗
- 7Bryniarski P Paradysz A Zyczkowski M Kupilas A Nowakowski K Bogacki R. A randomized controlled study to analyze the safety and efficacy of percutaneous nephrolithotripsy and retrograde intrarenal surgery in the management of renal stones more than 2 cm in diameter. J Endourol. 2012;26(1):52 57. (doi: 10.1089/end.2011.0235) 22003819 · doi ↗ · pubmed ↗
- 8Sabnis RB Ganesamoni R Doshi A Ganpule AP Jagtap J Desai MR. Micropercutaneous nephrolithotomy (microperc) vs retrograde intrarenal surgery for the management of small renal calculi: a randomized controlled trial. BJU Int. 2013;112(3):355 361. (doi: 10.1111/bju.12164) 23826843 · doi ↗ · pubmed ↗