Novel multielectrode mapping catheter for targeting left ventricular summit derived premature ventricular contractions within the great cardiac vein: first-in-man
Christian-H Heeger, Henning Rolfes, Martin W Bergmann, Maxim Didenko

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
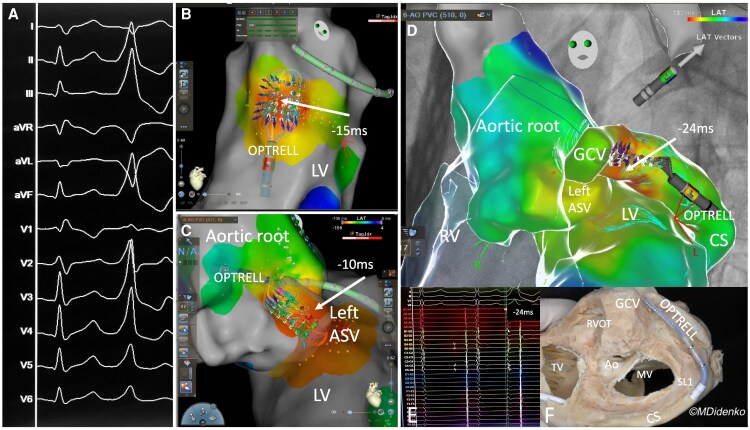 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Cardiac pacing and defibrillation studies · Cardiac electrophysiology and arrhythmias
Case description
A 20-year-old male patient presented with symptomatic monomorphic premature ventricular contractions (PVC) (34% PVC burden). The 12 lead electrocardiogram showed an inferior axis, positive concordant chest leads, a slurred QRS-complex onset and an QS configuration in Lead I, suggestive for an origin within the left ventricular (LV)-summit.^1,2^ The patient was scheduled for a catheter ablation procedure with a novel high density multielectrode (HDME) (n = 36 electrodes) grid-shape mapping catheter (OPTRELL, J&J MedTech). After transseptal puncture the mapping catheter was positioned at the endocardial LV-summit and a 3D map was generated (Carto 3; V8.2, J&J MedTech) with an earliest activation of 15 ms preceding QRS-complex onset. Additionally, the aortic root was mapped with an earliest activation of 10 ms at the left sinus of valsalva.^3^ Due to the slurred QRS-complex onset and insufficient activation an epicardial origin was suspected and the OPTRELL was positioned within the distal coronary sinus and was further advanced to the great cardiac vein (GCV) via a SL1 sheath. High density multielectrode mapping revealed the earliest activation at the distal GCV, preceding the QRS-complex onset by 24 ms. A contact force sensing ablation catheter (STSF, J&J MedTech) was advanced to the GCV and irrigated ablation (17 mL/min, 25W, AI 600) was performed. The PVC terminated immediately and the patient was discharged on the next day without any issues. With HDME mapping PVC beats can be captured automatically and activation and conduction can be visualized live by each individual electrode. This ability might be an advantaged to conventional mapping strategies. Although manoeuvring the HDME catheter to the GCV was feasible without any complications in this single case operators should be cautious. Here we are presenting the first case report of an epicardial LV-summit derived PVC targeted via the GCV. The PVC was rapidly and precisely located and targeted utilizing a novel HDME grid shaped mapping catheter suggestive for a feasible approach (Figure 1).
(A) Twelve lead electrocardiogram with frequent monomorphic premature ventricular contractions: Inferior axis, positive concordant chest leads, a slurre QRS-complex onset and a QS configuration in lead I: suggestive for an origin within the left ventricular-summit. (B) OPTRELL mapping catheter during 3D mapping (Carto 3; V8.2, J&J MedTech) of the left ventricular-summit. Please notice the conduction velocity vectors (colourful arrows) diverting from the center of the grid of the OPTRELL catheter precisely detecting the origin of the premature ventricular contractions (−15 ms preceding QRS-complex onset, earliest activation time). (C) OPTRELL mapping catheter during 3D mapping of the aortic root within the left coronary cusp. Please notice the conduction velocity vectors (colourful arrows) diverting from the left coronary cusp precisely detecting the origin of the premature ventricular contractions (−10 ms preceding QRS-complex onset, earliest activation time). (D) Merged 3D map of right ventricle, left ventricular, aortic root and coronary sinus/great cardiac vein: OPTRELL mapping catheter during 3D mapping within the great cardiac vein. Please notice the conduction velocity vectors (colourful arrows) diverting from the great cardiac vein precisely detecting the origin of the premature ventricular contractions. The target ablation area lies in the triangle between left coronary cusp, left ventricular, and great cardiac vein. The successful ablation site was in the distal great cardiac vein. (E) Intracardiac electrograms from the HDME catheter with the earliest activation time (−24 ms preceding QRS-complex onset). (F) Corresponding anatomical specimen with the OPTRELL mapping catheter within the distal great cardiac vein via a SL1 sheath. LCC, left coronary cusp; RV, right ventricle; GCV, great cardiac vein; PVC, premature ventricular contractions; LV, left ventricular.
Consent: The patient consent was obtained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heeger C-H, Hayashi K, Kuck K-H, Ouyang F. Catheter ablation of idiopathic ventricular arrhythmias arising from the cardiac outflow tracts– recent insights and techniques for the successful treatment of common and challenging cases. Circ J 2016;80:1073–1086.27074752 10.1253/circj.CJ-16-0293 · doi ↗ · pubmed ↗
- 2Ouyang F, Mathew S, Wu S, Kamioka M, Metzner A, Xue Y, et al Ventricular arrhythmias arising from the left ventricular outflow tract below the aortic Sinus cusps: mapping and catheter ablation via transseptal approach and electrocardiographic characteristics. Circ Arrhythmia Electrophysiol 2014;7:445–455.10.1161/CIRCEP.114.00169024795340 · doi ↗ · pubmed ↗
- 3Anderson RH, Mori S. Nomenclature of the components of the aortic root. Eur J Cardiothorac Surg 2019;55:1020.10.1093/ejcts/ezy 35830428026 · doi ↗ · pubmed ↗