Systematic Review and Meta‐Analysis of Audiometric Parameters for Assistive Hearing Technology for Adults and Children With Tympanic Membrane Perforation
Thomas Hampton, Alan Sanderson, Kevin Mortimer, Mahmood Bhutta

TL;DR
This study reviews hearing loss data in people with eardrum perforations to guide the development of hearing aids and other assistive technologies.
Contribution
The study provides the first systematic review and meta-analysis of audiometric data for hearing technology rehabilitation in tympanic membrane perforation.
Findings
Adults with eardrum perforations have an average air conduction hearing threshold of 48.3 dB HL.
Children with eardrum perforations have better hearing thresholds compared to adults, both in air and bone conduction.
Most individuals with eardrum perforations can benefit from either air or bone conduction hearing devices.
Abstract
Tympanic membrane perforation can cause hearing impairment with detrimental effects on communication and quality of life, and is a problem affecting an estimated 250 million people. To date, there is little analysis to inform public policy on options for assistive hearing technology rehabilitation in this group. We undertook a systematic review and meta‐analysis of six electronic databases registered with PROSPERO and reported in accordance with PRISMA 2020 standards. The primary outcome was the mean air and bone conduction hearing threshold associated with tympanic perforation. Of 720 studies identified, 16 contained data for meta‐analysis. Mean air conduction threshold was 48.3 dB HL in adults and 31.9 dB HL in children. Mean bone conduction was 26.6 dB HL in adults and 9.5 dB HL in children. The prediction interval was −1.7 to 46.7 dB HL for bone conduction and 15.0–70.5 dB HL for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
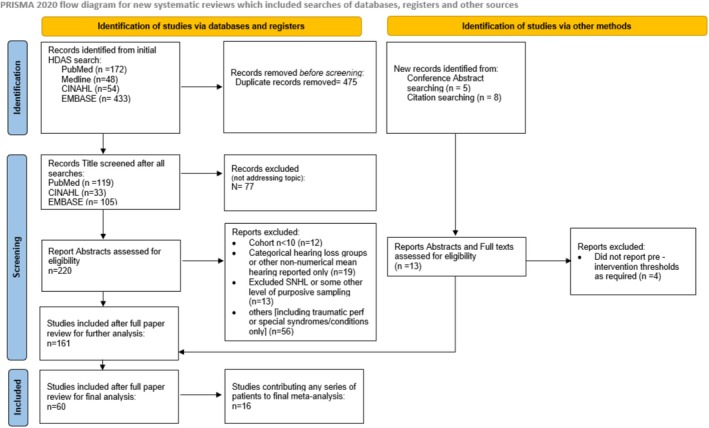 FIGURE 1
FIGURE 1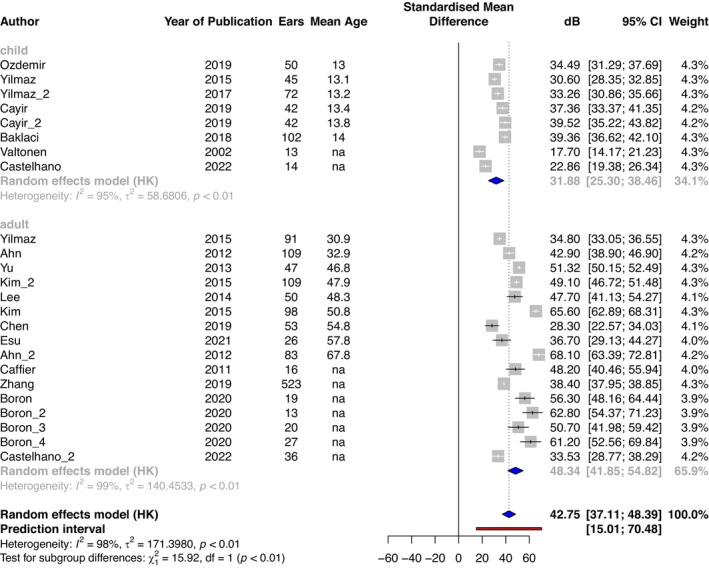 FIGURE 2
FIGURE 2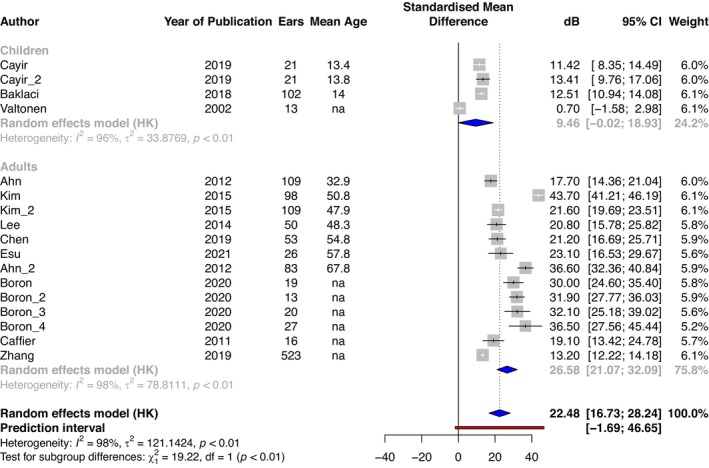 FIGURE 3
FIGURE 3| 1 | 2 | 3 | 4 | |
|---|---|---|---|---|
| Concept | Tympanic membrane perforation | Hearing threshold | Hearing loss | Chronic suppurative otitis media, otitis media and cholesteatoma |
| Actual term searched | ‘tympanic membrane perforation’ OR ‘ear drum perforation*’ OR ‘perforation*’ | Hearing threshold* OR hearing level* OR audiogram* OR ‘hearing test*’ | ‘Hearing loss’ OR Deaf* OR ‘Hearing impair*’ | ‘Chronic suppurative otitis media’ OR ‘Chronic supporative otitis media’ OR ‘CSOM’ OR ‘Chronic otitis media’ OR ‘Otitis media’ OR ‘Otitis media with effusion’ OR ‘glue ear’ OR ‘Cholesteatoma*’ |
| Audiological parameter | Assistive technology option | Predicted candidates |
|---|---|---|
| Air conduction thresholds up to 80 dB | Air conduction aid | Majority of adults and children |
| Bone conduction thresholds up to 60 dB | Implanted bone conduction aid | Majority of adults and children |
| Bone conduction thresholds up to 30 dB | Non‐implanted bone conduction aid | Majority of adults and children up to (at least) age 58 |
- —Wellcome Trust 10.13039/100010269
- —TWJ Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEar Surgery and Otitis Media · Hearing Loss and Rehabilitation · Hearing, Cochlea, Tinnitus, Genetics
Summary
- Question: What hearing threshold level would you expect for adults and children with tympanic membrane perforation, and what type of assistive technology could help them?
- Findings: In this systematic review and meta‐analysis that assessed 720 studies, adults with a tympanic perforation had a mean air conduction threshold of 48.3 dB HL and children of 31.9 dB HL.
- Additional findings: Mean bone conduction thresholds in adults were 26.6 dB HL and in children 9.5 dB HL.
- Meaning: Most children and adults could benefit from air conduction devices, and most children and adults up to age 58 years could also benefit from bone conduction devices.
- Future: These findings can guide the provision and further development of affordable assistive hearing technology for adults and children with tympanic membrane perforation.
Introduction
1
Tympanic membrane (TM) or ear drum perforation is a condition with reported prevalence from 0.45% to 3% across the world [1, 2]. Such perforations may be associated with hearing loss or with recurrent or persistent ear discharge, with the latter termed chronic suppurative otitis media (CSOM) [3]. CSOM has been modelled to have a global prevalence of 250 million people and disproportionately affects socioeconomically disadvantaged populations, with those in high‐income settings typically having a prevalence of one in 200, but countries with lower socio‐economic status reportedly having as much as 25 times higher [4].
The TM has an integral role in transforming sound pressure from acoustic energy in the air into ossicular vibration [5], hence tympanic perforation causes conductive hearing loss. Human cadaveric studies report that if the whole TM is missing, this is associated with 27 dB hearing loss [6], but real‐world studies report variable severity. A third of hospital patients with CSOM in India had hearing loss better than 40 dB HL, a third had hearing loss 40–60 dB HL and a third had loss > 60 dB HL [7]. In some cases, hearing loss can also be due to erosion of the ossicles, middle ear mucosa thickening or fibrosis or the presence of middle ear effusion [8]. Those with a perforated TM may have additional sensorineural hearing loss, for example, because of presbyacusis or because the presence of CSOM has caused cochlear damage [9] (presumed to be due to inflammatory toxins) [3].
Options for rehabilitation of hearing in those with a tympanic perforation include myringoplasty (with or without ossiculoplasty), conventional air conduction hearing aids, or bone conduction hearing aids. A review of outcomes of myringoplasty in children found that (where measured) 89% achieved functional hearing (thresholds better than 30 dB HL) [10]. However, the majority of the population affected by CSOM lacks access to surgery, due to a complex array of factors, including affordability and availability of surgical expertise [11, 12].
Air conduction hearing aids can rehabilitate hearing loss of any cause and severity up to typically 80 dB thresholds [13], but tend to have low availability in low‐resource settings (largely because of poor availability of audiologists [12] to programme such aids and the affordability of the devices) [14]. Air conduction aids are also relatively contraindicated in the presence of a TM perforation because otorrhoea may prevent their use, or conversely, their use may precipitate or perpetuate otorrhoea [15].
Bone conduction hearing aids are used less often, particularly in low‐income settings, because traditionally such aids have been costly and require surgical implantation. However, recent availability and pilot data have shown the effectiveness of low‐cost non‐implanted bone conduction devices (BCD) such as personal music players or headsets for chronic middle ear effusion in children [16]. This has created an opportunity for this technology to be expanded for use in those with a perforated TM, including in low‐income settings [17]. BCD do not necessarily require programming in those with a purely conductive hearing loss, and so may preclude the need for an audiologist, but are less effective when sensorineural hearing loss is present. Implanted BCDs may be rendered ineffective when bone conduction thresholds are worse than 60 dB HL. For non‐implanted devices, function may be compromised if contact of the device with the skull is suboptimal because of loose fitting or thick overlying soft tissue [18], which can cause up to 20 dB loss of functional gain in high frequencies, and a difference in speech reception threshold of up to 7 dB [19].
To date, there are no data to inform national or international policy or strategy for assistive technology (air or bone conduction hearing aids) for the rehabilitation of hearing loss in people with a perforated TM. Data on the degree and type of hearing loss in the global population with CSOM are limited to individual case series. Here, we undertook a systematic review and meta‐analysis of published literature to evaluate air and bone conduction thresholds in children and adults with a perforated TM.
Methods
2
Literature Review of Hearing in Tympanic Perforation: Study Inclusion
2.1
The study was registered with PROSPERO (CRD42022255652) [20] and reported in accordance with the PRISMA 2020 standard [21].
We systematically searched published literature on hearing threshold with tympanic perforation on six electronic databases from inception until 1 December 2023: EMBASE, MEDLINE, CINAHL, WHO International Clinical Trial Registry Platform, the Cochrane library and the ISRCTN registry. Medical Subject Headings (MeSH terms) used to interrogate each database were synonyms of ‘hearing loss’, ‘hearing threshold’, ‘chronic suppurative otitis media’ and ‘tympanic membrane perforation’ (Table 1). There were no restrictions on year or language of publication. We included data from non‐English language papers if translated contents could be verified by a professional speaker/reader in that language. We consulted subject matter experts and manually searched reference lists of included publications to identify additional studies that may have been missed by the initial search.
We included studies of adults and/or children (those aged < 18) with TM perforation of whatever cause, from systematic reviews, randomised controlled trials, controlled (non‐randomised) clinical trials or cluster trials, cohort studies, case–control or nested case–control studies, cross‐sectional studies and case series (but excluding case series with fewer than 10 patients). We excluded animal or experimental studies, studies of individuals with otitis media or hearing loss due to named congenital disorders or chemotherapy or radiation‐induced damage and studies of tympanic perforation related to trauma, blast injury or acute otitis media. We excluded studies not reporting audiometric data.
Duplicates studies were identified and removed, and title, abstract and full‐text screening for relevance was independently undertaken by two reviewers (T.H., A.S.) using Endnote (version 20.2.1, Clarivate 2020). Where consensus was not achieved, arbitration was carried out by a third reviewer (M.B.). Studies were assessed for risk of bias using the Murad et al. [22] methodological quality tool and excluded where appropriate.
Review of Hearing in Tympanic Perforation: Data Extraction and Analysis
2.2
We recorded data on the characteristics of the study and participants, including age, sex, self‐reported ethnicity, active otorrhea, cause of perforation and disease laterality.
We extracted data on air and bone conduction hearing thresholds, and where this was from interventional studies, we used only pre‐intervention data. We contacted original study authors for clarification or for missing data where needed and possible.
We separated extracted data into that from children and from adults. Where studies included both adult and child participants and data could not be separated, data were excluded (because the differing prevalence of sensorineural hearing loss in adults vs. children could confound results).
We analysed aggregate data on hearing thresholds for mean average, median and inter‐quartile range. Where individual participant data were not available, we used aggregate parameters if these were reported by study authors. We performed a meta‐analysis of extracted data with the ‘meta’ and ‘metaphor’ package for R Studio (RStudio, PBC, Boston, MA) using a random effects model [23], assessing heterogeneity using I ^2^ and 𝜏 ^2^ tests, and calculating prediction intervals [24]. The prediction interval can help clinical interpretation of heterogeneity by estimating what true treatment effects or measures might be expected in future settings [25].
A priori subgroup analysis was planned and undertaken for age (paediatric < 18 years and adult ≥ 18 years) and for studies which reported perforation due to CSOM versus other causes, and for income status (World Bank ranking) of the country of study.
Results
3
Our search recovered 720 studies, with 235 remaining after de‐duplication, and 141 after screening abstracts and titles (Figure 1). After full‐text review, 60 studies were potentially informative, but on further analysis, only 16 studies included discrete data on hearing thresholds. No studies were excluded due to risk of bias.
PRISMA diagram of included and excluded studies in review of hearing in tympanic perforation. Source: Page et al. [21]. For more information, visit: http://www.prisma‐statement.org/ .
In the 16 included studies [26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40], data for 82 subgroups of patients with hearing thresholds were extracted, comprising 34 adult‐only series, eight child‐only series and 40 mixed‐age series. Differences in how hearing thresholds were recorded (e.g., recorded at each individual frequency or pooled average; measuring bone conduction, air conduction or only air‐bone gap and whether standard deviation was or was not reported) meant that only a few case series were informative for the final meta‐analysis: 16 series measuring adult air conduction thresholds, 13 measuring adult bone conduction, eight child air conduction and four child bone conduction. Data included in the final analysis comprised 1303 bone conduction thresholds and 1700 air conduction thresholds taken from 1394 ears of adults and 380 ears of children.
Overall mean air conduction threshold where reported was 42.8 dB (Figure 2), with a mean in adults of 48.3 dB (95% CI: 41.9–54.8 dB, n = 1320 ears, I ^2^ = 99%, p < 0.01), and in children of 31.9 dB (95% CI: 25.3–38.5 dB, n = 380 ears, I ^2^ = 95%, p < 0.01). Mean bone conduction threshold where reported was 22.5 dB HL (95% CI: 16.7–28.2 dB) (Figure 3), with a mean in adults of 26.6 dB (95% CI: 21.1–32.1 dB, n = 1146 ears, I ^2^ = 98%, p < 0.01), and in children of 9.5 dB (95% CI: 0.0–18.9 dB, n = 157 ears, I ^2^ = 96%, p < 0.01). The prediction interval (estimates where the true effects would be expected for 95% of similar (equivalent) studies that could be conducted in the future [25]) had bounds of −1.7 to 46.7 dB for bone conduction and 15.0–70.5 dB for air conduction (Figures 2 and 3).
Mean air conduction thresholds (dB) of adults and children with tympanic membrane perforation. Mean of respective series = blue diamond, pooled mean of all included studies = dashed line and diamond, prediction interval = red line. Individual study series are ordered by mean age (years). Where such data were not available (na), the series is at the bottom of the plot.
Mean bone conduction thresholds (dB) of adults and children with tympanic membrane perforation. Mean of respective series = blue diamond, pooled mean of all included studies = dashed line and diamond, prediction interval = red line. Individual study series are ordered by mean age (years). Where such data were not available (na), the series is at the bottom of the plot.
There was an apparent and expected trend of worse hearing with increasing age, but regression demonstrated only weak correlation for both air (p = 0.8) and bone conduction (p = 0.9). In subgroup analysis, 38 series included perforations associated with CSOM, totalling 2365 ears. There was only one series in children and one in adults evaluating air conduction thresholds in perforations without CSOM, meaning there were insufficient studies for subgroup analysis on this variable. There were also insufficient data to allow analysis on country or regional income status.
Discussion
4
We sought to define parameters for air and bone conduction aids as options for the rehabilitation of hearing loss in children and adults with a perforated TM.
For air conduction thresholds, our meta‐analysis included case series for children and adults up to a mean age of 68, and here the upper range of the prediction interval was 70 dB. This implies that 95% of adults up to age 68 years with a perforated TM can potentially benefit from air conduction aids able to amplify to this level. Contemporary air conduction hearing aids can easily provide linear amplification up to a hearing threshold of 60–65 dB [41] and a highest peak gain of 87 dB [42] with average functional gains of 39 dB [43].
For bone conduction thresholds, the meta‐analysis included case series for children and adults also up to a mean age of 68, and here the upper range of the prediction interval was 47 dB. This implies that 95% of adults up to age 68 with a perforated TM can be rehabilitated with a bone conduction aid able to amplify to this level. Implanted bone conduction aids can be effective for those with bone conduction thresholds of up to 60 dB [44]. However, it is noteworthy that in all the case series for children (Figure 3), the maximum upper 95% confidence interval for bone conduction thresholds was 17 dB, and in the case series for adults (where mean age was reported) up to the age of 58, the maximum upper 95% confidence interval limit was 30 dB. This implies that 95% of adults up to age 58 with a perforated TM will be rehabilitated with bone conduction aids able to amplify to this level. External (non‐implanted) bone conduction aids are also likely to be able to amplify to this level, but this is yet to be proven.
These audiological parameters and options for hearing rehabilitation are summarised in Table 2.
Heterogeneity (I ^2^) was as high as 99% for adult bone conduction thresholds. We explored this by calculating 95% prediction intervals, which were calculated with bounds of −1.7 to 46.7 dB for bone conduction and 15.0–70.5 dB for air conduction (see Figures 2 and 3). If there were an absence of any between‐study heterogeneity, this prediction interval would coincide with the respective confidence intervals [25]. However, here, even though our prediction interval covers a wider range, importantly, even with these boundaries, our analysis implies that most adults and children with a perforated TM are likely to benefit from a BCD.
We are cognisant that the majority of the global population with perforated TMs live in low‐ and middle‐income countries. Access to assistive technology for such populations is limited, for example, in some areas of Africa, air conduction aids have been estimated to reach only 3% of those who may benefit [45], although recent legislative changes in the United States to enable over‐the‐counter sales of such technology [46] may improve availability.
The option for non‐implanted bone conduction aids is particularly relevant for low‐resource settings, where such options could be inexpensive and not require the presence of a medical professional. Additional research should seek to clarify differences in head and skull morphology and soft tissue depth measurements to inform the future design of such devices for different age groups. The impact on sound conduction of external BCD from soft tissue thickness and pressure at contact points is also an area for future research.
At present, extrinsic BCD are largely offered as a pre‐implantation trial for those patients considering implanted bone‐anchored hearing devices [47], and their sound transmission is not as good as implanted devices [48], with studies showing up to 20%–40% lower speech recognition [19]. Any proposed external device would need real‐world evaluation of candidacy and performance.
There are limitations to our analysis. Although our search yielded community and observational studies, all studies included in the meta‐analysis were exclusively hospital populations, and it is possible disease severity in this group is greater than in the community. Factors such as lower socio‐economic status and the presence of otorrhoea may also associate with disease and hearing severity [49], but in our dataset were poorly recorded, precluding analysis on such variables. We have not reported frequency‐specific mean and median hearing thresholds because of the poor granularity of data in included studies. Related to this, it is possible that bone conduction levels may be artificially elevated (particularly at 2 kHz frequency) due to the Carhart effect [50], although this would be unlikely to affect our conclusions by an appreciable amount.
Conclusion
5
Our analysis has demonstrated the prediction interval for expected hearing thresholds for adults and children with a perforated TM. The findings suggest that preserved cochlear function is likely in children, and the mean hearing threshold in both adults and children suggests the majority of people in both groups will benefit from air or bone conduction assistive technology. The parameters and options we have outlined should help in the implementation of assistive technology to rehabilitate hearing loss and improve quality of life in the millions of children and adults across the world affected by a perforated TM.
Author Contributions
T.H. and M.B. conceptualised the article. T.H. developed the search strategy. T.H. and A.S. appraised papers. T.H. analysed the data and wrote the original draft of the article. T.H., K.M. and M.B. acquired funding. T.H., A.S., K.M. and M.B. provided critical appraisal and editorial contributions. All authors approved the final submitted version. T.H. agreed to be accountable for all aspects of the work.
Ethics Statement
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1H. Kaftan , M. Noack , N. Friedrich , H. Voelzke , and W. Hosemann , “Prevalence of Chronic Tympanic Membrane Perforation in the Adult Population,” HNO 56, no. 2 (2008): 145–150.17476471 10.1007/s 00106-007-1574-0 · doi ↗ · pubmed ↗
- 2M. C. Phanguphangu , “Otoscopic Examinations Reveal High Prevalence of Outer and Middle Ear Pathologies in Paediatrics in Limpopo, South Africa,” International Journal of Audiology 56, no. 4 (2017): 215–218.27783901 10.1080/14992027.2016.1244868 · doi ↗ · pubmed ↗
- 3M. F. Bhutta , A. J. Leach , and C. G. Brennan‐Jones , “Chronic Suppurative Otitis Media,” Lancet 403, no. 10441 (2024): 2339–2348, 10.1016/s 0140-6736(24)00259-9.38621397 · doi ↗ · pubmed ↗
- 4J. Acuin , Chronic Suppurative Otitis Media ‐ Burden of Illness and Management Options (World Health Organization, 2004), https://citeseerx.ist.psu.edu/document?repid=rep 1&type=pdf&doi=041789 aafa 9dc 73fdb 91c 1091 ca 2b 873bebb 35cd.
- 5H. Tang , P. Psota , J. J. Rosowski , C. Furlong , and J. T. Cheng , “Analyses of the Tympanic Membrane Impulse Response Measured With High‐Speed Holography,” Hearing Research 410 (2021): 108335.34450569 10.1016/j.heares.2021.108335 PMC 8484071 · doi ↗ · pubmed ↗
- 6N. Bevis , B. Sackmann , T. Effertz , M. Lauxmann , and D. Beutner , “The Impact of Tympanic Membrane Perforations on Middle Ear Transfer Function,” European Archives of Oto‐Rhino‐Laryngology 279, no. 7 (2022): 3399–3406, 10.1007/s 00405-021-07078-9.34570265 PMC 9130167 · doi ↗ · pubmed ↗
- 7A. K. Rana , D. Upadhyay , A. Yadav , and S. Prasad , “Correlation of Tympanic Membrane Perforation With Hearing Loss and Its Parameters in Chronic Otitis Media: An Analytical Study,” Indian Journal of Otolaryngology and Head & Neck Surgery 72, no. 2 (2020): 187–193.32551276 10.1007/s 12070-019-01740-9PMC 7276457 · doi ↗ · pubmed ↗
- 8K. K. Pannu , S. Chadha , D. Kumar , and Preeti , “Evaluation of Hearing Loss in Tympanic Membrane Perforation,” Indian Journal of Otolaryngology and Head & Neck Surgery 63, no. 3 (2011): 208–213.22754796 10.1007/s 12070-011-0129-6PMC 3138953 · doi ↗ · pubmed ↗