Successful Management of Pregnancy in a Patient With Fabry Disease Receiving Continuous Enzyme Replacement Therapy: A Case Report and Literature Review
Yuka Kido, Mariko Nakahara, Katsutoshi Takahashi, Saya Nagasawa, Yojiro Maruyama, Daiki Ogishima

TL;DR
A woman with Fabry disease successfully managed her condition and pregnancy while continuing enzyme replacement therapy, with generally good outcomes for both mother and baby.
Contribution
This case report and literature review provide evidence that enzyme replacement therapy can be safely continued during pregnancy in Fabry disease patients.
Findings
Patients on enzyme replacement therapy during pregnancy had lower rates of proteinuria compared to those without the therapy.
Common symptoms like limb pain and proteinuria often worsened during pregnancy despite ongoing treatment.
Pregnancy complications such as preeclampsia and preterm delivery occurred in a small percentage of cases, but no congenital anomalies were observed in newborns.
Abstract
Fabry disease is an X-linked lysosomal storage disorder characterized by deficient or reduced α-galactosidase A activity, resulting in the progressive accumulation of globotriaosylceramide in vascular endothelial cells. Although traditionally considered an X-linked recessive disorder predominantly affecting the male population, the heterozygous female population frequently develops significant clinical manifestations. Pregnancies complicated by Fabry disease are associated with an increased risk of hypertensive disorders of pregnancy and exacerbation of Fabry disease-specific symptoms. While enzyme replacement therapy and chaperone therapy have revolutionized disease management, the rarity of Fabry disease has precluded the establishment of consensus guidelines for pregnancy management. We present a case of successful maternal and perinatal management in a pregnant woman with Fabry…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
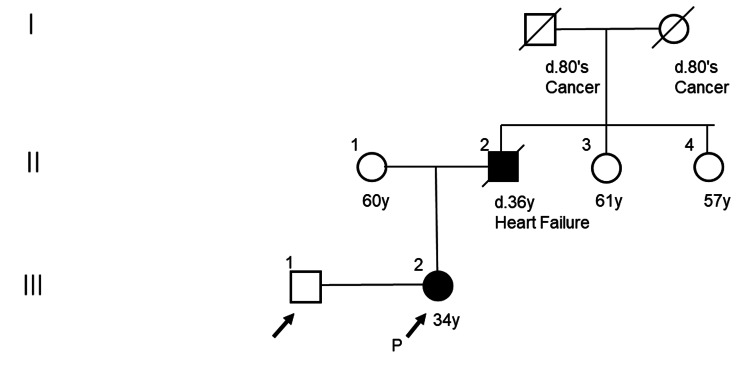 Figure 1
Figure 1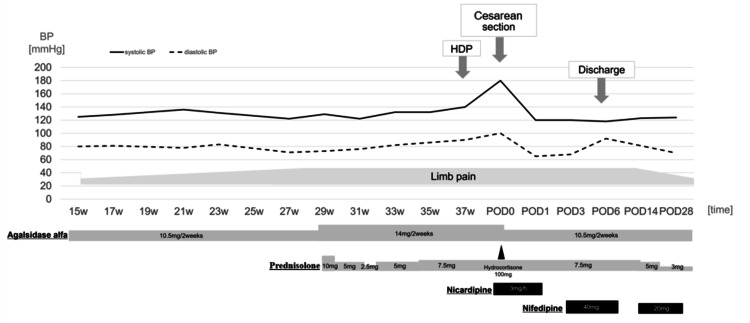 Figure 2
Figure 2| No. | Authors, year | Age at pregnancy (years) | Age at diagnosis (years) | Variant | Fabry signs and symptoms | Drugs during pregnancy | Worsening symptoms of FD during pregnancy | Pregnancy complications |
| 1 | Wendt et al. [ | 34 | 15 | NA | Joint pain, diarrhea and cramps, proteinuria, fatigue | Agalsidase alfa | - | - |
| 2 | Kalkum et al. [ | 33 | 30 | p.Ala143Thr | Burning pain, hypohidrosis, angiokeratoma, migraine, tinnitus, depression, proteinuria | Agalsidase alfa | Pain in the legs | Gestational diabetes, preterm PROM |
| 3 | Kalkum et al. [ | 38 | 34 | p.Asn320Ile | Acroparesthesia, abdominal pain, chronic neuropathic pain, hypertension | Agalsidase alfa | Headache in the 19th week of gestation | - |
| 4 | Parent et al. [ | 36 | 34 | p.Cys56Ter (c.168C4A) | Acroparesthesia, tinnitus, hearing loss, hypohidrosis, cold intolerance, abdominal cramping, diarrhea | Agalsidase beta | - | - |
| 5 | Germain et al. [ | 21 | 13 | p.Cys52Arg | Peripheral neuropathic pains, diarrhea, hypohidrosis, edema, proteinuria | Agalsidase beta | - | - |
| 6 | Bouwman et al. [ | 24 | 21 | p.Arg310Ter | Acroparesthesia, proteinuria, multiple white matter abnormalities of brain | Agalsidase beta | - | - |
| 7 | Politei [ | 37 | 31 | p.Leu415Pro | Acroparesthesia, angiokeratomas, syncopal episodes, corneal verticillata, fatigue | Agalsidase beta | - | - |
| 8 | Senocak Tasci and Bicik [ | 26 | 25 | p.Leu275Phe | Corneal opacity, corneal verticillata, limb position sense deficit, proteinuria, stenosis of the common carotid artery | Agalsidase beta | - | - |
| 9 | Senocak Tasci and Bicik [ | 29 | 28 | p.Leu275Phe | Papules like angiokeratomas, photophobia, acroparesthesia, proteinuria, fatigue | Agalsidase beta | - | - |
| 10 | Iwafuchi et al. [ | 22 | 22 | p.Gly375Glu (c.1124G>A) | Proteinuria, macroscopic hematuria | Agalsidase alfa | - | - |
| 11 | Fernández et al. [ | 36 | 35 | p.Cys174Gly | Acroparesthesia, pain crisis, heat intolerance, hearing loss, peripheral nervous system involvement | Agalsidase alfa | - | - |
| 12 | Fernández et al. [ | 38 | 35 | p.Cys174Gly | Acroparesthesia, pain crisis, heat intolerance, decrease in glomerular filtration rate | Agalsidase alfa | - | - |
| 13 | Fernández et al. [ | 24 | 22 | p.Cys174Gly | Severe pain crisis, microalbuminuria | Agalsidase alfa | - | Eclampsia, hypertensive crisis, proteinuria at the 36th week of gestation |
| 14 | Fernández et al. [ | 26 | 22 | p.Cys174Gly | Severe pain crisis, microalbuminuria | Agalsidase alfa | - | - |
| 15 | Fernández et al. [ | 19 | 16 | p.Cys174Gly | Decrease in glomerular filtration rate | Agalsidase alfa | - | - |
| 16 | Fernández et al. [ | 29 | 28 | p.Cys174Gly | Decrease in glomerular filtration rate | Agalsidase alfa | Impaired renal function, kidney disease progression | - |
| 17 | Fernández et al. [ | 22 | 18 | p.Cys174Gly | Decrease in glomerular filtration rate | Agalsidase alfa | Impaired renal function, kidney disease progression | - |
| 18 | Madsen et al. [ | 38 | 2 | p.Gly85Asn | Ischemic stroke, hypertension, albuminuria, decrease in glomerular filtration rate, transient ischemic attack | Agalsidase beta, acetylic acid, labetalol | Blood pressure and albuminuria increased, renal function decreased in the 3rd trimester | Preeclampsia |
| 19 | Politt and Gaik [ | 30 | 19 | NA | Diarrhea, sweating, acroparesthesia, hypertrophied septum | Agalsidase alfa | - | - |
| 20 | Paydas and Akcabay [ | 28-29 | 28 | p.Asp313Tyr | Recurrent episodic abdominal pain | Agalsidase alfa | - | - |
| 21 | Paydas and Akcabay [ | 30-31 | 28 | p.Asp313Tyr | Recurrent episodic abdominal pain | Agalsidase alfa | - | - |
| 22 | Kido et al., 2025 | 37 | 10 | c.178_179del | Limb pain, ischemic stroke, painful subcutaneous nodule | Agalsidase alfa, prednisolone | Pain in the legs | HDP (GH), placenta previa |
| Pregnancy complications | FD with ERT (n = 22) |
Literature values in patients with FD without ERT [ | Odds ratio (95% confidence interval) | p-value |
| Hypertensive disorders of pregnancy | 3 (13.6%) | 12 (10.8%) | 1.18 (0.20-5.00) | 0.73 |
| Preeclampsia | 2 (9.1%) | 5 (4.9%) | 1.93 (0.17-12.84) | 0.61 |
| Proteinuria | 2 (9.1%) | 38 (37.2%) | 0.17 (0.02-0.76) | 0.01 |
| Premature delivery | 2 (9.1%) | 16 (18.8%)* | 0.43 (0.04-2.11) | 0.35 |
| Eclampsia | 1 (4.5%) | NA | NA | NA |
| Gestational diabetes | 1 (4.5%) | 9 (8.8%) | 0.49 (0.01-3.92) | 0.69 |
| Placenta previa | 1 (4.5%) | NA | NA | NA |
| No. | Authors, year | Delivery mode | Gestational age (weeks) | Sex | Birth weight (g) | Apgar score | FD | Others |
| 1 | Wendt et al. [ | NA | 37 | M | 3,010 | 9/10 | - | NA |
| 2 | Kalkum et al. [ | eCS | 36 | M | 2,790 | 9/10 | - | NA |
| 3 | Kalkum et al. [ | NA | Term | F | NA | NA | + | Hemangioma |
| 4 | Parent et al. [ | ND | 38 | F | 2,885 | 2/10 | - | - |
| 5 | Germain et al. [ | ND | 38 | M | 3,120 | 10/10 | - | NA |
| 6 | Bouwman et al. [ | NA | NA | F | NA | NA | + | NA |
| 7 | Politei [ | ND | 38 | M | 3,300 | 9/10 | + | NA |
| 8 | Senocak Tasci and Bicik [ | NA | 40 | F | 3,100 | NA | - | - |
| 9 | Senocak Tasci and Bicik [ | NA | 40 | F | 3,400 | NA | NA | - |
| 10 | Iwafuchi et al. [ | NA | 40 | F | 2,734 | 8/9 | + | NA |
| 11 | Fernández et al. [ | ND | 37 | F | 3,800 | 9/10 | - | Recurrent urinary tract infection |
| 12 | Fernández et al. [ | ND | 39 | M | 3,190 | 8/10 | - | NA |
| 13 | Fernández et al. [ | eCS | 36 | F | 2,370 | 6/10 | + | NA |
| 14 | Fernández et al. [ | CS | 37 | M | 2,890 | 8/10 | - | NA |
| 15 | Fernández et al. [ | ND | 39 | M | 3,085 | 8-9/10 | - | NA |
| 16 | Fernández et al. [ | ND | 39 | F | 2,730 | 8-9/10 | - | NA |
| 17 | Fernández et al. [ | ND | 38 | F | 2,530 | 8-9/10 | - | Asthma |
| 18 | Madsen et al. [ | CS | 38 | M | 2,675 | 10/10 | - | NA |
| 19 | Politt and Gaik [ | CS | 40 | NA | 3,200 | Normal | NA | NA |
| 20 | Paydas and Akcabay [ | ND | 37 | M | NA | 9/10 | - | - |
| 21 | Paydas and Akcabay [ | ND | 37 | M | NA | NA | Not tested | - |
| 22 | Kido et al., 2025 | CS | 37 | M | 2,504 | 8/9 | + | - |
| Symptoms of FD | Before pregnancy (n = 22) | Worsening symptoms during pregnancy with ERT (n = 22) |
| Proteinuria | 10 (45.5%) | 2 (9.1%) |
| Limb pain | 9 (40.9%) | 2 (9.1%) |
| Acroparesthesia | 7 (31.8%) | 0 (0%) |
| Abdominal symptoms | 7 (31.8%) | 0 (0%) |
| Renal dysfunction* | 5 (22.7%) | 3 (13.6%) |
| Ear symptoms | 3 (13.6%) | 0 (0%) |
| Hypertension | 2 (9.1%) | 1 (4.5%) |
| Cerebrovascular disease | 2 (9.1%) | 0 (0%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLysosomal Storage Disorders Research · Trypanosoma species research and implications · Child Nutrition and Feeding Issues
Introduction
Fabry disease (FD) is a progressive metabolic disorder characterized by the pathogenic accumulation of globotriaosylceramide resulting from deficient or reduced α-galactosidase A (α-GAL) activity. The natural history of untreated FD includes progressive renal failure, cardiovascular complications, and cerebrovascular events. The prevalence of FD among newborns is reported to be one in 10,000 patients, with a higher prevalence among male newborns (one in 3,125) than in female newborns (one in 100,000) [1]. While traditionally classified as an X-linked recessive disorder primarily affecting the male population, contemporary understanding [2] recognizes that the heterozygous female population frequently develops significant clinical manifestations. Some studies [2,3] reported that pregnancies complicated by FD are associated with an increased incidence of gestational hypertension and exacerbation of disease-specific symptoms.
The advent of enzyme replacement therapy (ERT) and chaperone therapy has dramatically improved the prognosis of FD [4]. However, due to the condition's rarity, consensus guidelines for management during pregnancy and the perinatal period remain lacking. This report presents our experience with the maternal and perinatal management of a pregnant woman with FD who maintained α-GAL therapy throughout pregnancy, supplemented by a comprehensive review of the relevant literature.
Case presentation
A 37-year-old nulligravida with paternally inherited FD presented for prenatal care. Her family history was significant for her father's death from heart failure at age 36 (Figure 1).
Family tree of the patient in the present case
The patient's clinical course began with corneal opacity in childhood, and reduced α-GAL activity was initially detected at age 10. Genetic testing at age 18 identified a pathogenic variant in the GLA gene (NM_000169.3:c.718_719del, p.Lys240Glu). The patient's disease progression included the onset of limb pain at age 27, leading to the initiation of ERT with α-GAL (0.2 mg/kg every 2-3 weeks) at age 30 following a pattern of remitting and relapsing symptoms. Prednisolone 3 mg/day was administered for elevated inflammatory response. The patient manifested painful subcutaneous nodules at 31 years of age. Histopathological examination of the biopsied tissue revealed non-specific findings without diagnostic features. After marriage at age 33, she pursued genetic counseling in preparation for family planning. At the age of 35, she experienced a cerebral infarction (both old and fresh lacunar infarctions), with concurrent elevation of plasma Lyso-Gb3 to 3.74 ng/mL (reference: <2 ng/mL). Following successful in vitro fertilization while maintaining ERT, the patient was referred to our institution at 14 weeks' gestation for specialized perinatal care. Initial evaluation revealed stable manifestations of FD, including chronic cerebral infarction sequelae, painful subcutaneous nodules, and urinary mulberry bodies. Cardiac function was preserved (ejection fraction 71%) with no evidence of wall motion abnormalities, diastolic dysfunction, or left ventricular hypertrophy. Renal function remained normal with no proteinuria. ERT was continued during pregnancy under multidisciplinary management, with a dose of 10.5 mg administered for patients weighing less than 55 kg. The dose was changed to 14 mg after 29 weeks' gestation when the patient's weight exceeded 55 kg. At 27 weeks' gestation, the patient manifested peripheral limb pain unresponsive to acetaminophen therapy (1,000-2,000 mg daily). Given the persistent symptoms, corticosteroid intervention was initiated with prednisolone at 10 mg daily, subsequently titrated to 7.5 mg daily according to symptom intensity. Mild gestational hypertension developed at 36 weeks' gestation but remained non-severe, with no evidence of proteinuria or end-organ damage. An elective cesarean delivery was performed at 37 weeks and one day due to partial placenta previa. Intraoperative hemorrhage from the placental separation site required intrauterine balloon tamponade for hemostasis. The procedure duration was 64 minutes, with an estimated blood loss of 1,251 g (including amniotic fluid). A male infant was delivered weighing 2,504 g (appropriate for gestational age), with Apgar scores of 8 and 9 at one and five minutes, respectively. Neonatal examination revealed no apparent congenital anomalies. Postoperative recovery was uneventful with blood pressure well-controlled on nifedipine 40 mg/day, enabling discharge on postoperative day 6. The patient's limb pain improved postpartum, allowing gradual prednisolone tapering (Figure 2).
Management of Fabry disease and blood pressure (BP) during pregnancyHDP: hypertensive disorders of pregnancy; POD: postoperative day
Newborn screening for FD via expanded mass spectrometry on day 4 indicated the need for further evaluation. Subsequent testing confirmed FD diagnosis with reduced leukocyte α-GAL activity (0.1 nmol/hr/mL). Genetic testing was also performed on the infant, and the same pathogenic variants as the mother were detected, leading to a definitive diagnosis of FD.
Discussion
This report describes the successful management of pregnancy in a woman with FD and prior cerebrovascular complications, demonstrating favorable maternal and fetal outcomes with continued ERT. Despite developing mild gestational hypertension and requiring cesarean delivery for placenta previa, the patient maintained stable disease status without stroke recurrence or cardiac dysfunction through term gestation. Current therapeutic options for FD include ERT and chaperone therapy. ERT, established approximately two decades ago, functions by supplementing agalsidase to facilitate globotriaosylceramide clearance from affected cells [5]. To contextualize our experience, we manually conducted a literature review using the search formula “fabry AND pregnancy AND enzyme replacement therapy” in the PubMed database (June 1997 to April 2024) without language or geographic restrictions. After excluding French-language publications and reviews, we identified 22 cases of FD-complicated pregnancies managed with continued ERT (including our case) (Table 1) [6-17]. A seminal study by Holmes and Laney analyzing 41 women with FD (102 pregnancies) reported ERT use in only four cases (9.8%) [3]. Comparative analysis of pregnancies with continued ERT (Group A) versus those without (Group B) revealed several notable findings (Table 2).
Group A complications included hypertensive disorders of pregnancy (13.6%), preeclampsia (9.1%), proteinuria (9.1%), preterm delivery (9.1%), eclampsia (4.5%), gestational diabetes (4.5%), and placenta previa (4.5%). Group B demonstrated comparable rates of gestational hypertension (10.8%) and preeclampsia (4.9%) but higher rates of proteinuria (37.2%) [3]. Statistical analysis was performed using R software version 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria). Due to the small sample size, Fisher's exact test was employed to compare complication rates between groups, with odds ratios and 95% confidence intervals calculated to quantify the associations. A p-value < 0.05 was considered statistically significant. Additional neonatal complications in Group A included hemangioma (4.5%), recurrent urinary tract infections (4.5%), and asthma (4.5%). Importantly, no low-birth-weight infants or congenital anomalies were reported among the 20 term deliveries (Table 3).
The pathogenesis of hypertensive disorders in FD-complicated pregnancies likely involves disrupted angiogenic balance and placental dysfunction [18]. Recent histopathological studies have demonstrated extensive GL-3 accumulation across multiple placental cell types, including intermediate trophoblasts, endothelial cells, and smooth muscle cells of maternal vessels within the decidua [19]. While the transplacental distribution of supplemental enzymes remains incompletely characterized, our review suggests an increased occurrence of complications in late pregnancy despite ERT. Disease manifestations in women with FD are diverse, with acroparesthesia representing the most common initial symptom [20]. Prepregnancy symptoms in Group A included proteinuria (45.5%), limb pain (40.9%), acroparesthesia (31.8%), gastrointestinal symptoms (31.8%), renal dysfunction (22.7%), hypertension (9.1%), and cerebrovascular disease (9.1%) (Table 4).
Our patient experienced worsening limb pain despite continued therapy, necessitating steroid administration. Pain management during pregnancy remains challenging due to limited therapeutic options, and the efficacy of steroid therapy was modest in our case.
Genetic counseling played a crucial role in this case, particularly given the X-linked inheritance pattern of FD. The identified GLA variant (NM_000169.3:c.718_719del, p.Lys240Glu) informed preconception counseling, which addressed inheritance patterns, recurrence risks, and therapeutic options during pregnancy. While preimplantation genetic testing remains unavailable in Japan, comprehensive genetic counseling facilitated informed decision-making regarding pregnancy continuation with ERT. Subsequent neonatal testing confirmed FD diagnosis, prompting ongoing genetic counseling. This case series has inherent limitations, including small sample size, potential selection bias, and incomplete data capture typical of observational studies. While current evidence suggests the safety of ERT during pregnancy, prospective studies with comprehensive outcome assessment are needed.
Conclusions
This case demonstrates successful maternal and fetal outcomes in an FD-complicated pregnancy managed with continuous ERT. While our findings support the safety of maintained ERT during pregnancy, larger prospective studies are needed to establish definitive evidence-based guidelines. Currently, management decisions should involve careful shared decision-making between healthcare providers and patients, with individualized risk-benefit assessment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Impact of GLA variant classification on the estimated prevalence of Fabry disease: a systematic review and meta-analysis of screening studies Circ Genom Precis Med Monda E Diana G Graziani F 016202310.1161/CIRCGEN.123.00425238047356 · doi ↗ · pubmed ↗
- 2Prevalence of symptoms in female Fabry disease patients: a case-control survey J Inherit Metab Dis Bouwman MG Rombach SM Schenk E Sweeb A Wijburg FA Hollak CE Linthorst GE 8918983520122243107310.1007/s 10545-011-9447-9PMC 3432199 · doi ↗ · pubmed ↗
- 3A retrospective survey studying the impact of Fabry disease on pregnancy JIMD Rep Holmes A Laney D 57632120152570126710.1007/8904_2014_384PMC 4470955 · doi ↗ · pubmed ↗
- 4Developments in the treatment of Fabry disease J Inherit Metab Dis van der Veen SJ Hollak CE van Kuilenburg AB Langeveld M 9089214320203208333110.1002/jimd.12228 PMC 7540041 · doi ↗ · pubmed ↗
- 5Enzyme replacement therapy in Fabry disease: a randomized controlled trial JAMA Schiffmann R Kopp JB Austin HA 3rd 2743274928520011138693010.1001/jama.285.21.2743 · doi ↗ · pubmed ↗
- 6Successful pregnancy outcome in a patient with Fabry disease receiving enzyme replacement therapy with agalsidase alfa J Inherit Metab Dis Wendt S Whybra C Kampmann C Teichmann E Beck M 7877882820051615191010.1007/s 10545-005-0018-9 · doi ↗ · pubmed ↗
- 7Enzyme replacement therapy with agalsidase alfa in pregnant women with Fabry disease Eur J Obstet Gynecol Reprod Biol Kalkum G Macchiella D Reinke J Kölbl H Beck M 929314420091923353510.1016/j.ejogrb.2009.01.007 · doi ↗ · pubmed ↗
- 8Fabry disease complicating pregnancy J Matern Fetal Neonatal Med Parent E Wax JR Smith W Blaszyk H Pinette MG Cartin A Blackstone J 125312562320102012139610.3109/14767050903580391 · doi ↗ · pubmed ↗