A Man With Exertional Dyspnea
Jumpei Yamashita, Daisuke Mizu, Hidenori Higashi, Masataka Miyamoto

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
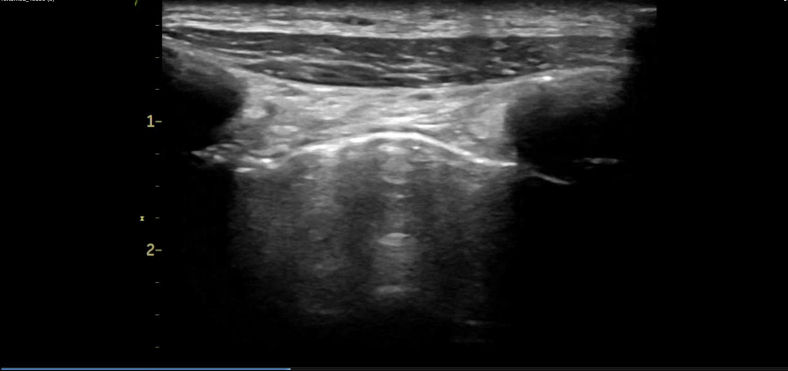 Figure 1
Figure 1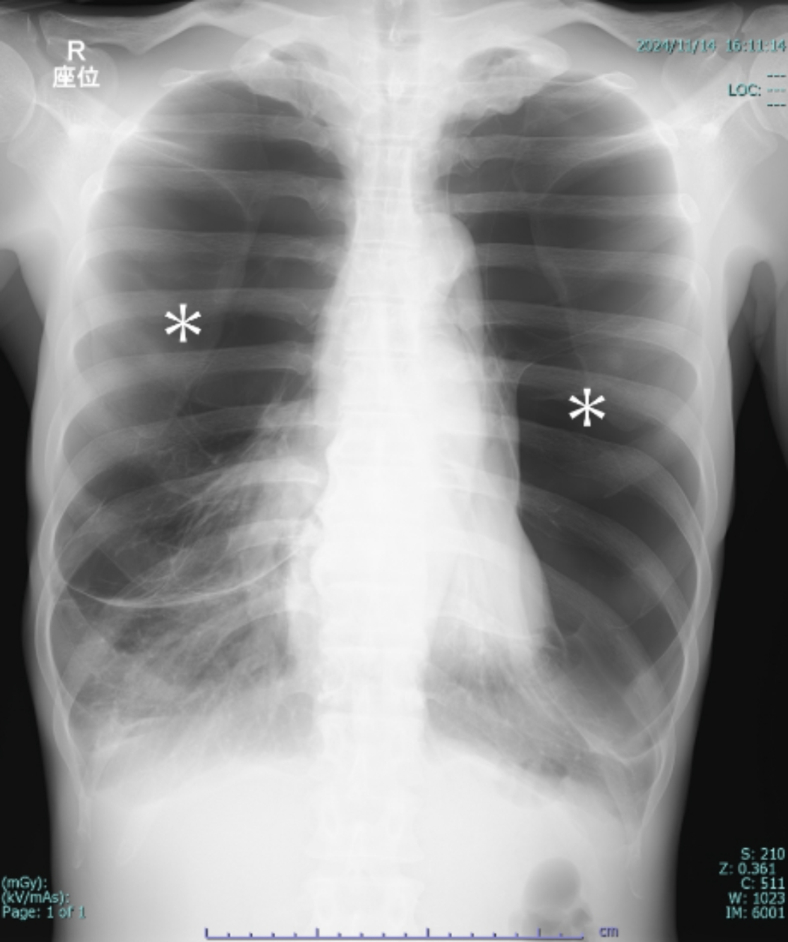 Figure 2
Figure 2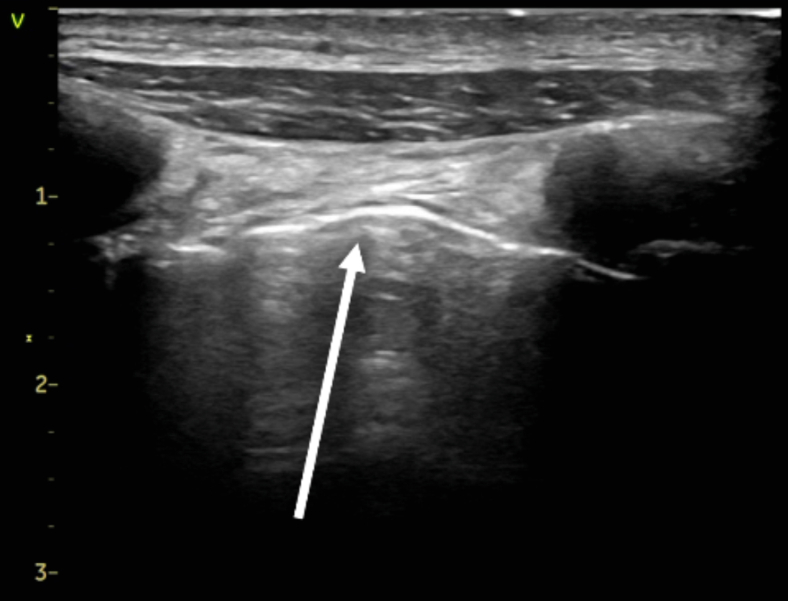 Figure 3
Figure 3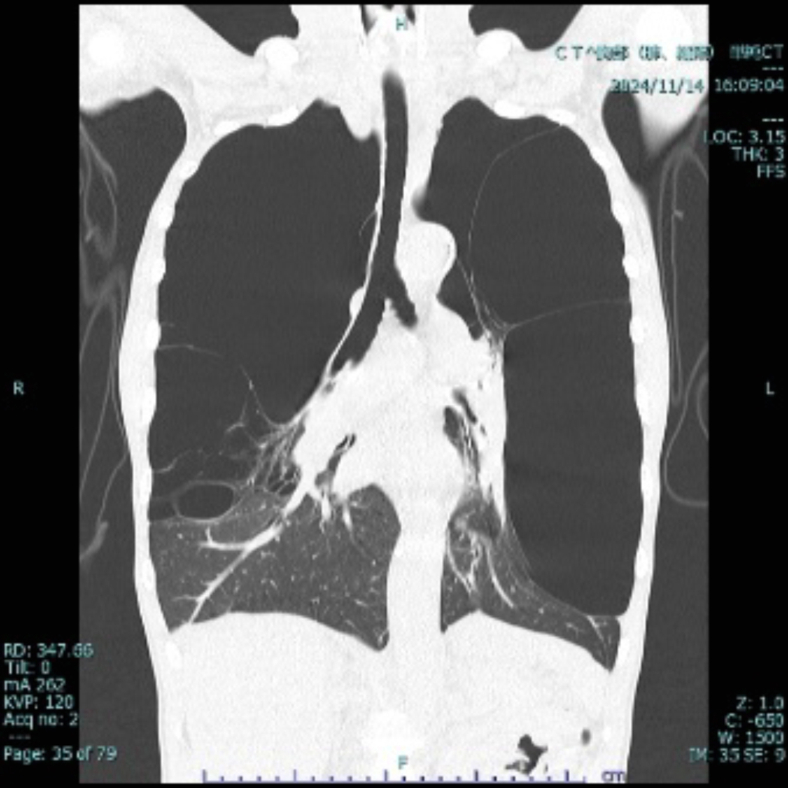 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Pericarditis and Cardiac Tamponade
Patient Presentation
1
A 48-year-old man with a history of smoking (30 cigarettes per day for 30 years) presented to our emergency department with exertional dyspnea. Bilateral respiratory sounds were weakened, the respiratory rate was 22, and the oxygen saturation level was 90% on ambient air. Chest radiography revealed increased lung translucency bilaterally (Fig 1). Although we initially suspected bilateral pneumothorax, lung ultrasonography revealed a lung sliding sign (Fig 2; Video), ruling out pneumothorax. Computed tomography revealed giant bullae with compressed lung parenchyma (Fig 3).Figure 1. Chest radiography showing increased lung translucency and absent vascular markings in the upper and middle lung fields bilaterally (asterisks).Figure 2. Lung ultrasonography showing sliding signs (arrow).VideoLung sliding signs showing vanishing lung syndrome.Figure 3. The area of hyperlucency that appeared to be a pneumothorax on chest radiography is found to be a giant bulla on computed tomography.
Diagnosis: Vanishing Lung Syndrome With Idiopathic Giant Bullous Emphysema
2
Vanishing lung syndrome (VLS) is characterized by giant bullae occupying more than one-third of the thoracic cavity, compressing surrounding lung tissue.1 It typically originates in the upper lobes.1 Radical treatment involves surgical resection,2^,^3 and the patient underwent bullectomy under veno-venous extracorporeal membrane oxygenation support at a later date. VLS presents with diminished breath sounds and increased lung translucency on radiography, mimicking pneumothorax. In patients with VLS, placing a chest tube may cause secondary pneumothorax.1^,^4 In the present case, lung ultrasonography revealed a sliding sign, which led us to rule out pneumothorax and prevent unnecessary drainage. This case highlights the use of lung ultrasonography as an immediate diagnostic tool for differentiating VLS from pneumothorax.
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
Conflict of Interest
All authors have affirmed they have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferreira Junior E.G.Costa P.A.Silveira L.M.F.G.Almeida L.E.M.Salvioni N.C.P.Loureiro B.M.Giant bullous emphysema mistaken for traumatic pneumothorax Int J Surg Case Rep 562019505410.1016/j.ijscr.2019.02.00530826593 PMC 6402233 · doi ↗ · pubmed ↗
- 2Yousaf M.N.Chan N.N.Janvier A.Vanishing lung syndrome: an idiopathic bullous emphysema mimicking pneumothorax Cureus 1282020 e 959610.7759/cureus.9596 PMC 747852032923201 · doi ↗ · pubmed ↗
- 3Wang J.Liu W.Vanishing lung syndrome Can Respir J 21120142810.1155/2014/58369724511569 PMC 3938235 · doi ↗ · pubmed ↗
- 4Ye Y.Zhan Y.Giant pulmonary bullae mistaken for pneumothorax Am J Emerg Med 832024162.e 1162.e 310.1016/j.ajem.2024.07.00839004543 · doi ↗ · pubmed ↗