Analysis of 4 Cases of Left Bundle Branch Block With Ventricular Preexcitation
M. M. Li Yi, B. M. Li Xingjie

TL;DR
This paper describes four cases where ventricular preexcitation coexists with left bundle branch block, highlighting differences based on accessory pathway location.
Contribution
The study provides new clinical insights into electrocardiographic patterns of WPW with LBBB based on real patient cases.
Findings
Right-sided accessory pathways were observed in one case, while left-sided pathways were found in three cases.
Electrocardiographic features varied depending on the location of the accessory pathway.
Intermittent WPW was confirmed in all four cases.
Abstract
This paper reports 4 cases of ventricular preexcitation (WPW) accompanied by left bundle branch block (LBBB). WPW appeared intermittently in all cases: Case 1 involved a right‐sided accessory pathway, while Cases 2–4 involved left‐sided accessory pathways. The electrocardiographic characteristics of both right‐sided and left‐sided accessory pathways coexisting with LBBB are discussed.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
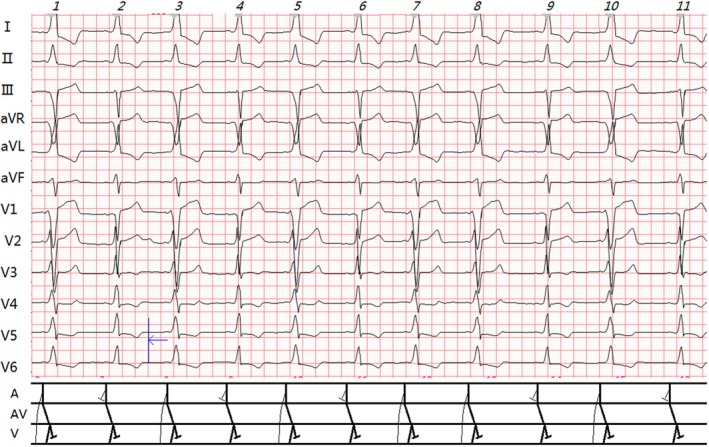 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2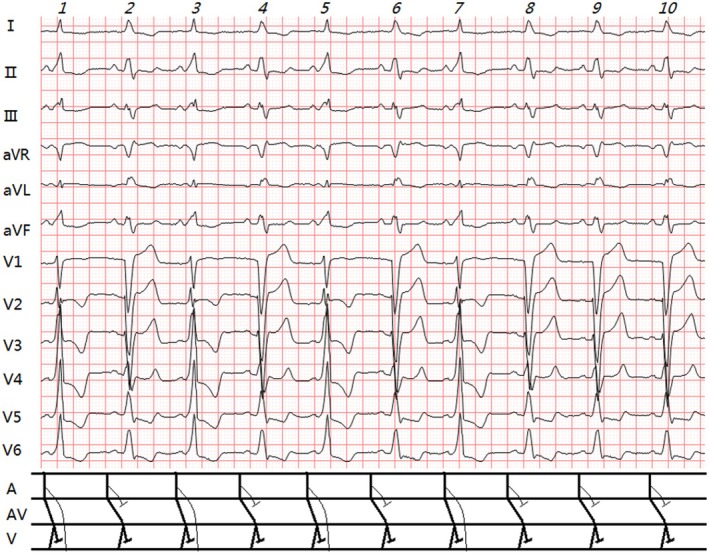 FIGURE 3
FIGURE 3 FIGURE 4
FIGURE 4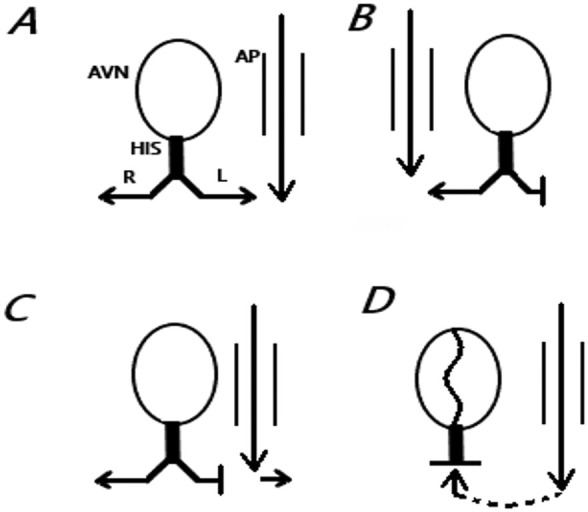 FIGURE 5
FIGURE 5| Case no. | Gender | Age | Clinical diagnosis | Accessory pathway localization (based on Δ wave direction) | WPW presentation | LBBB presentation | Characteristics of WPW + LBBB | QRS features in OAVRT | Other findings |
|---|---|---|---|---|---|---|---|---|---|
| Case 1 | Male | 22 | Hypertrophic Obstructive Cardiomyopathy | Right lateral wall | Intermittent | Persistent | Neither masks the other | ||
| Case 2 | Female | 50 | ① Type 2 Diabetes; ② Hypertension; ③ Coronary Artery Disease | Left posterior septum | Intermittent (Figure | Intermittent (Figure | WPW masks LBBB | LBBB‐typ | |
| Case 3 | Male | 84 | Coronary Artery Disease | Left anterior wall | Intermittent | Persistent | WPW masks LBBB | ||
| Case 4 | Male | 73 | ① Type 2 Diabetic Nephropathy; ② Hypertension; ③ Coronary Artery Disease | Left anterior wall | ① Intermittent; ② Complete (Figure | Persistent | ① Complete WPW obscures LBBB (Figure | Intermittent First‐Degree AVB (Figure |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Cardiac pacing and defibrillation studies · Cardiac electrophysiology and arrhythmias
Chiale P.A. et al. (Chiale and Elizari 2012) noted that WPW with LBBB is rare. We hereby report 4 cases encountered in our practice.
Discussion
1
LBBB and WPW are distinct arrhythmias characterized by wide QRS complexes. When coexisting, their ECG interpretation becomes challenging. Pick (Pick and Fisch 1958) reported a 0.24% coexistence rate of bundle branch block (BBB) and WPW in 100,000 ECGs. Since right BBB (RBBB) is twice as common as LBBB (Surawicz and Knilans 2008), the estimated prevalence of LBBB + WPW is – 0.08% (Pick and Fisch 1958).
Pick (Pick and Fisch 1958) proposed:
- WPW can coexist with RBBB or LBBB.
- If the accessory pathway and BBB are contralateral, both features are discernible.
- Ipsilateral pathways pre‐excite the blocked ventricle, masking BBB.
- Bilateral pathways may obscure BBB.
The four patients in this study did not undergo intracardiac electrophysiological studies, and the localization of the atrioventricular accessory pathways could only be determined based on the direction of the Δ waves (Surawicz and Knilans 2008) in the surface electrocardiogram (see Table 1).
Case 1 (right‐sided pathway + LBBB): Due to contralateral pathways, both features remained visible (Figures 1 and 5B). PJ intervals were 0.30s.
Case 1's standard ECG (calibration: 1 mV = 2.5 mm). Slanted numbers above the figure denote QRS complex sequence. In the ladder diagram, thin arcs represent accessory pathway conduction, and thick lines indicate normal pathway conduction (same for subsequent figures). Additional details are provided in the text. Clinical summary of Case 1 (Table 1). ECG Analysis (Figure 1): Sinus rhythm (64 bpm). Two types of QRS complexes: 1. Isolated LBBB (R2, 4, 6, 9, 11): PR 0.14 s; no delta wave; broad R waves in leads I, aVL, V5, V6; QS pattern in V1; QRS duration 0.16 s; PJ interval 0.30s. 2. WPW + LBBB (R1, 3, 5, 7, 8, 10): PR 0.08 s; Δ wave present; QRS duration 0.22 s; PJ 0.30s; rS pattern in V1–V3 (r/S < 1, rV1 blunted); R/S transition at V4; R/S > 1 in I, aVL. Diagnosis: ① Sinus rhythm; ② LBBB; ③ Intermittent WPW (right‐sided pathway).
Case 2–4 involves a patient with a left‐sided accessory pathway and LBBB. Since the accessory pathway and the BBB are on the same side, part of the left ventricular myocardium that was originally activated with a delay due to the LBBB is pre‐activated by the impulse conducted through the accessory pathway. Therefore, the waveform of the LBBB is often masked by the WPW, and the P‐J interval is shortened. When the combination of LBBB and WPW appears continuously, because the waveforms of both are atypical, it is extremely easy to lead to missed diagnosis or misdiagnosis (see Figures 2, 3, 4 and Figure 5C). Only when one of them appears intermittently can the other show a typical manifestation. Therefore, it is necessary to make full use of the electrocardiographic information of pure LBBB or WPW revealed by intermittent WPW, intermittent LBBB, OAVRT, or junctional activation for analysis and identification.
(A–C) (Case 2): Clinical summary of Case 2 (Table 1). ECG analysis: (A) Sinus rhythm (83 bpm); typical WPW without LBBB (Figure 5A): PR 0.11 s, delta wave, Rs/R pattern in V1‐V6; QRS duration 0.14 s; PJ 0.26 s. (B) Sinus rhythm (63 bpm). Two QRS types: 1. Isolated LBBB (R1, 2, 5–7): PR 0.16 s; no Δ wave; broad R waves in I, aVL, V5, V6; rS in V1; QRS 0.16 s; PJ 0.32 s. 2. WPW + LBBB (R3, 4, 8): PR 0.11 s; Δ wave present; V1 shifts from Rs (A) to rS due to LBBB; R pattern in V2‐V6; QRS 0.14 s; PJ 0.26 s. (C) OAVRT (166 bpm); QRS morphology similar to LBBB in (B); RP− interval 0.16 s, P −R 0.20s. Diagnosis: ① Sinus rhythm; ② Intermittent LBBB; ③ Intermittent WPW (left‐sided pathway); ④ OAVRT.
(Case 3): Clinical summary of Case 3 (Table 1). ECG analysis: Sinus rhythm (71 bpm). Two QRS types: 1. Isolated LBBB (R2, 4, 6, 8–10): PR 0.16 s; QRS 0.16 s; QS in V1; broad R waves in I, aVL, V5, V6; PJ 0.32 s. 2. WPW + LBBB (R1, 3, 5, 7):PR 0.12 s; Δ wave present; QRS 0.17 s; PJ 0.29 s; rS in V1, Rs/R in V2‐V6. Diagnosis: ① Sinus rhythm; ② LBBB; ③ Intermittent WPW (left‐sided pathway).
(A–B) (Case 4): Clinical summary of Case 4 (Table 1). ECG Analysis: (A):Sinus rhythm (79 bpm). Two QRS types: 1. Isolated LBBB (R2, 4, 6, 8): PR 0.24 s; QRS 0.16 s; PJ 0.40s. 2. Complete WPW (R1, 3, 5, 7): PR 0.12 s;Δ wave present; QRS 0.18 s; PJ 0.30s; R/Rs pattern in V1‐V6. (B) WPW + LBBB (R9–13): PR 0.12 s; Δ wave present; QRS 0.18 s; PJ 0.30s; hybrid QRS morphology (notable in I, III, V1, V2); rS in V1, Rs/R in V2‐V6. Diagnosis: ① Sinus rhythm; ② Intermittent first‐degree AVB; ③ LBBB; ④ Intermittent WPW (left‐sided pathway).
Scenarios of LBBB with WPW. (A) WPW without bundle branch block; (B) Right‐sided pathway with LBBB: Neither masks the other; (C) Left‐sided pathway with LBBB: Accessory pathway pre‐excites the delayed LBBB region, masking LBBB; (D) Left‐sided pathway with first‐degree AVB: Complete WPW obscures LBBB due to retrograde block in the normal pathway.
Case 4 (Figure 4A): First‐degree AVB (PR 0.24 s) delayed normal pathway conduction, allowing exclusive accessory pathway activation (Figure 5D). LBBB was entirely masked. Complete WPW and LBBB alternated, mimicking RBBB‐LBBB alternation. Fusion waves emerged only after AVB resolution (Figure 4B).
In Ebstein's anomaly, RBBB often coexists with WPW. Iturralde et al. found that 94% of patients exhibited RBBB post‐ablation (Chiale and Elizari 2012). Whether LBBB and WPW share similar associations remains unclear; our cases likely reflect random coincidence.
Author Contributions
The author takes full responsibility for this article.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chiale, P. A. , and M. V. Elizari . 2012. “The Electrocardiographic Diagnosis of Intraventricular Blocks Coexisting With Ventricular Preexcitation.” Journal of Electrocardiology 45, no. 5: 515–524.22560599 10.1016/j.jelectrocard.2012.04.002 · doi ↗ · pubmed ↗
- 2Pick, A. , and C. Fisch . 1958. “Ventricular Pre‐Excitation (WPW) in the Presence of Bundle Branch Block.” American Heart Journal 55, no. 4: 504–512.13533228 10.1016/0002-8703(58)90027-9 · doi ↗ · pubmed ↗
- 3Surawicz, B. , and T. K. Knilans . 2008. Chou's Electrocardiography in Clinical Practice. 6th ed, 485–497. Saunders.