Impact of Video-Assisted Teaching on Knowledge and Practice Regarding the Use of Metered Dose Inhalers Among Patients With Obstructive Respiratory Disorders
Gargee U Karadkar, Rashmi P Choudhary

TL;DR
A study found that video-assisted teaching improved patients' knowledge and use of inhalers for respiratory disorders like asthma and COPD.
Contribution
The study demonstrates that video-assisted teaching significantly enhances inhaler knowledge and practice in obstructive respiratory disorder patients.
Findings
Pre-test knowledge and practice scores were poor in both groups, but the intervention group showed significant improvement.
Paired t-tests revealed statistically significant improvements in knowledge and practice scores after the intervention.
Post-test scores in the intervention group were significantly higher than in the control group.
Abstract
Introduction: Obstructive respiratory disorders include asthma and chronic obstructive pulmonary disease (COPD). This study was conducted with an aim to assess the impact of video-assisted teaching on knowledge and practice regarding the use of metered dose inhalers among outpatient department patients with obstructive respiratory disorders and a comparison of these knowledge and practices across the intervention and control groups was done. Methodology: A quasi-experimental two-group pre-test and post-test design was used; 162 participants (81 each in the intervention and control groups) were selected using a simple random sampling technique, all from the Navi Mumbai Municipal Corporation Hospital, Navi Mumbai. A pre-test was taken, and video-assisted teaching was provided related to knowledge and practice regarding the use of metered dose inhalers, and on the eighth day, the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
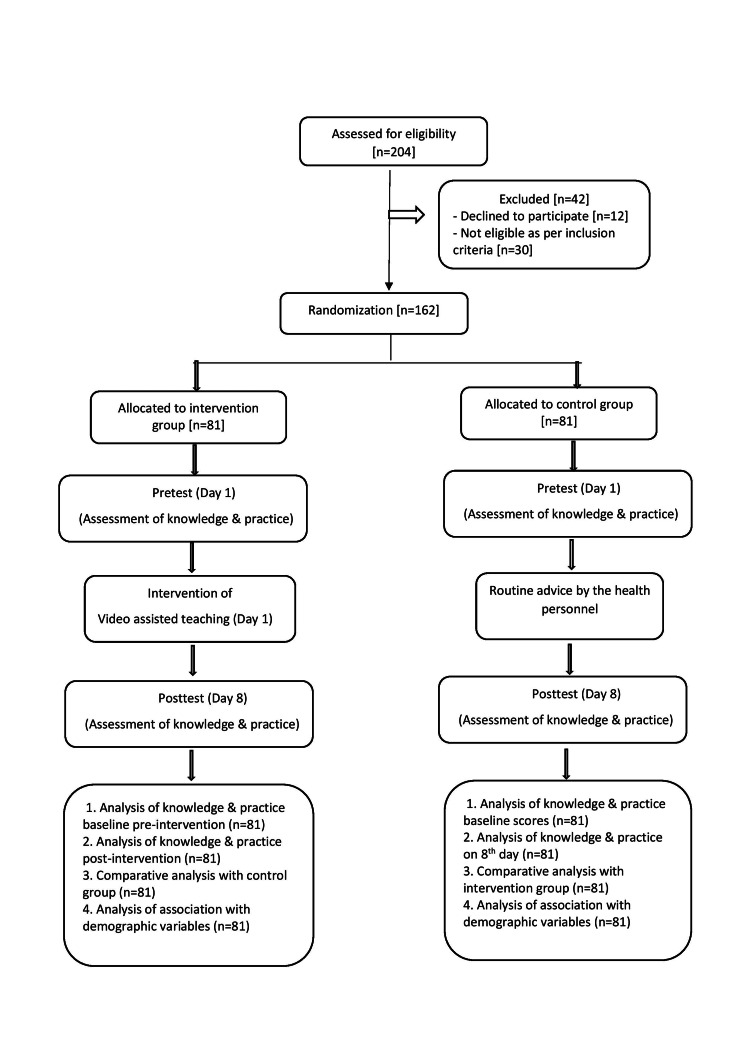 Figure 1
Figure 1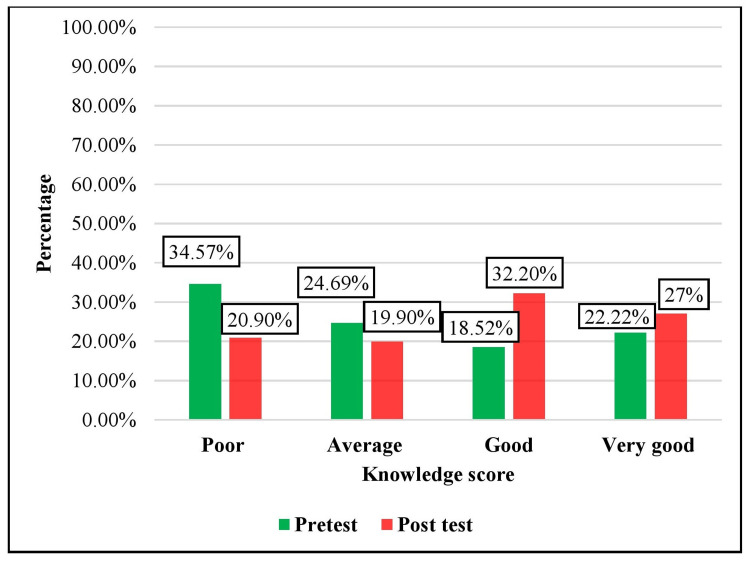 Figure 2
Figure 2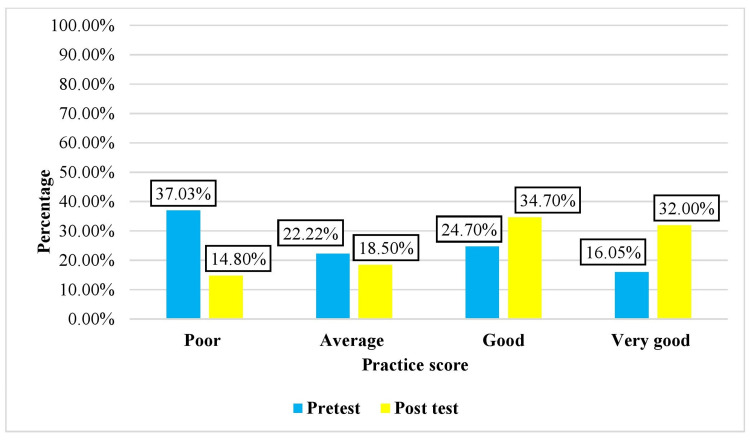 Figure 3
Figure 3| Demographic variable | Category | Intervention group | Control group | ||
| Age | f | % | f | % | |
| <30 years | 42 | 51.9 | 40 | 49.4 | |
| 30.1-40 years | 23 | 28.4 | 23 | 28.4 | |
| >40.1 years | 16 | 19.7 | 18 | 22.2 | |
| Gender | Female | 39 | 48.1 | 41 | 50.6 |
| Male | 42 | 51.9 | 40 | 49.4 | |
| Education | Diploma | 31 | 38.3 | 32 | 39.5 |
| Graduation | 8 | 9.9 | 8 | 9.9 | |
| High school | 4 | 4.9 | 1 | 1.2 | |
| Intermediate | 10 | 12.3 | 29 | 35.8 | |
| Middle school | 2 | 2.5 | 2 | 2.5 | |
| Professional degree | 26 | 32.1 | 9 | 11.1 | |
| Occupation | Clerks | 1 | 1.2 | 11 | 13.6 |
| Craft and related work | 0 | 0 | 1 | 1.2 | |
| Professionals | 32 | 39.5 | 16 | 19.8 | |
| Technical work | 31 | 38.3 | 34 | 42 | |
| Unemployed | 17 | 21 | 19 | 23.4 | |
| Type of family | Joint | 24 | 29.6 | 20 | 24.7 |
| Nuclear | 52 | 64.2 | 53 | 65.4 | |
| Separated family | 5 | 6.2 | 8 | 9.9 | |
| Information on the use of inhalers | Yes | 39 | 48.1 | 33 | 40.7 |
| No | 42 | 51.9 | 48 | 59.3 | |
| Variable | Category | Intervention group | Control group | ||
| F | % | F | % | ||
| Diagnosis | Asthma | 44 | 54.3 | 44 | 54.3 |
| COPD | 37 | 45.7 | 37 | 45.7 | |
| Duration of illness | 1.1 to 2 years | 18 | 22.2 | 16 | 19.8 |
| 2.1 to 3 years | 28 | 34.6 | 26 | 32.1 | |
| 3.1 to 4 years | 15 | 18.5 | 24 | 29.6 | |
| 4.1 to 5 years | 20 | 24.6 | 15 | 18.5 | |
| Use of a metered dose inhaler | With a spacer | 10 | 12.3 | 2 | 2.5 |
| Without a spacer | 71 | 87.7 | 79 | 97.5 | |
| Duration of use of a metered dose inhaler | 1.1 to 2 years | 42 | 51.9 | 16 | 19.8 |
| 2.1 to 3 years | 13 | 16.0 | 18 | 9.9 | |
| 3.1 to 4 years | 15 | 18.5 | 20 | 13.6 | |
| 4.1 to 5 years | 11 | 13.6 | 27 | 6.2 | |
| Frequency of use of a metered dose inhaler | Once a day | 23 | 28.4 | 33 | 40.8 |
| Twice a day | 24 | 29.6 | 26 | 32.1 | |
| Thrice a day | 13 | 16.1 | 10 | 12.3 | |
| More than three times | 21 | 25.9 | 12 | 14.8 | |
| Knowledge level | Score category | Group | |||
| Intervention | Control | ||||
| Frequency | Percentage | Frequency | Percentage | ||
| Poor | 1-6 (0-25%) | 28 | 34.57 | 26 | 32.1 |
| Average | 7-12 (26-50%) | 20 | 24.69 | 18 | 22.22 |
| Good | 13-18 (51-75%) | 15 | 18.52 | 20 | 24.70 |
| Very good | 19-24 (76-100%) | 18 | 22.22 | 17 | 20.98 |
| Total | 81 | 100 | 81 | 100 | |
| Practice level | Score category | Group | |||
| Intervention | Control | ||||
| Frequency | Percentage | Frequency | Percentage | ||
| Poor | 0-4 (0-25%) | 30 | 37.03 | 36 | 44.44 |
| Average | 5-10 (26-50%) | 18 | 22.22 | 16 | 19.75 |
| Good | 11-15 (51-75%) | 20 | 24.70 | 17 | 21 |
| Very good | 16-21 (76-100%) | 13 | 16.05 | 12 | 14.81 |
| Total | 81 | 100 | 81 | 100 | |
| Intervention group | N | Statistic | Pre-test score | Post-test score | Df | t -value | p -value | Significance |
| Knowledge | 81 | Mean | 10.81 | 13.88 | 80 | -14.65 | 0.001 | Significant |
| Standard deviation | 8.28 | 4.36 | ||||||
| Practice | 81 | Mean | 11.48 | 15.67 | 80 | -17.97 | 0.001 | Significant |
| Standard deviation | 8.86 | 4.71 |
| Group | N | Mean | Standard deviation (SD) | t-value | df | p-value | Significance |
| Intervention | 81 | 13.88 | 4.36 | -19.43 | 80 | 0.001 | Significant |
| Control | 81 | 14.72 | 8.72 |
| Group | N | Mean | Standard deviation (SD) | t-value | df | p-value | Significance |
| Intervention | 81 | 15.67 | 4.36 | -18.7 | 80 | 0.001 | Significant |
| Control | 81 | 7.91 | 5.6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInhalation and Respiratory Drug Delivery · Asthma and respiratory diseases · Respiratory Support and Mechanisms
Introduction
Obstructive respiratory disorders include conditions that are characterized by airway obstruction, such as bronchitis, bronchiectasis, asthma, and chronic obstructive pulmonary disease (COPD). Among these, asthma and COPD are the most common diseases that are prevalent globally. In the 21st century, COPD is a disease that has become one of the major health issues in developing countries [1,2]. Common environmental factors like air pollution due to increasing urbanization, long-term smoking, exposure to chemicals, or second-hand smoke predispose patients to suffer from COPD. Asthma is a chronic inflammatory disorder of the lungs in which there is inflammation and narrowing of the airways. The patient may present with seasonal or regular asthma exacerbations [3]. Inhaled medications are used to treat respiratory disorders such as asthma, COPD, and obstructive lung disorders. With the advent of technology and modern medicine, conventional tablets and syrups have been used in conjunction with inhalers for relaxation of the airways to ease breathing. These have been proven to be very effective and safe ways to relieve dyspnea. Inhalers have been found to be patient-friendly, making it easy for them to use and very handy to carry wherever required and available at an affordable cost. Even if the doctors prescribe medicines, the patient needs to follow the instructions for increasing the effectiveness of treatment [4].
Metered dose inhalers (MDIs) are the first-choice device for most people with COPD or asthma with acute exacerbations, but they are not easy to use unless proper education is provided. Studies have shown that an incorrect inhaler technique can lead to inadequate asthma management, resulting in poor asthma control and clinical outcomes. Rates of incorrect inhaler techniques continue to remain high among asthma patients, with minimal improvement in recent times. Since this remains a real challenge in achieving optimal asthma control, investing more time in educating patients on appropriate inhaler use becomes important for healthcare professionals [5].
In practice, patient satisfaction regarding the correct self-use of the MDI device has remained a matter of concern, thus affecting patient outcomes. Nurses are primarily involved in caring for patients and administering the inhaler therapy. Patient education on the correct use of the inhaler technique by nurses would provide confidence to patients on the effective use of inhalers and optimize the relief and control of asthma symptoms. It will further help in reducing complications and subsequent mortality in patients living with asthma or COPD [6].
Thus, this study focused on educating patients by developing and incorporating a video-assisted educational intervention on knowledge and practice regarding the use of MDIs for patients with obstructive respiratory disorders. It aimed to assess the effectiveness of this video-assisted teaching in patients who received the intervention with the help of pre-intervention and post-intervention observations, compare the findings with the control group, and find the association between pre-interventional knowledge and practices with selected sociodemographic variables of the patients.
The hypotheses that were statistically tested were as follows: H01: There is no significant difference between knowledge and practices regarding the use of MDIs in the intervention group of patients with obstructive respiratory disorders before and after video-assisted teaching at a 0.05 level of significance. H02: There is no significant difference between knowledge and practices regarding the use of MDIs between the intervention and control groups of patients with obstructive respiratory disorders at a 0.05 level of significance. H03: There is no significant association between pre-interventional knowledge and practices regarding the use of MDIs among patients with obstructive respiratory disorders and sociodemographic variables at the 0.05 level of significance.
Materials and methods
Study design
A quantitative research approach and quasi-experimental pre-test post-test design were employed to evaluate the impact of the video-assisted teaching intervention on knowledge and practice regarding the use of MDIs among patients with obstructive respiratory disorders. Participants were assigned to an intervention group and a control group.
Study participants and procedures
The patients were eligible if they were aged 18 years or older, diagnosed with obstructive respiratory disorders i.e., COPD and asthma and attending chest and pulmonary outpatient department from the selected hospital, received treatment on outpatient basis from Navi Mumbai Municipal Corporation Hospital in Navi Mumbai, using an MDI with or without spacer and who understood Hindi, English, or Marathi language. Patients were excluded if they were on other forms of medication or using MDIs for more than five years or if they did not provide written informed consent.
The data were collected after prior permission from the Ethical Committee of Bharati Vidyapeeth (Deemed to be University) College of Nursing, Pune (BV(DU)/CON/EC/64/ 2021-22) and hospital authorities, followed by informed consent being taken from the patients. A total sample of 162 patients diagnosed with obstructive respiratory disorders was included using a probability sampling method, with a simple random sampling technique for ensuring unbiased representation of the population. The sample size was determined by power analysis to ensure adequate statistical power for the study. The calculated sample size was 162 patients, with 81 participants in the intervention group and 81 participants in the control group. Probability simple random sampling was used for the selection of the participants. The 81 participants who fulfilled the inclusion criteria were randomly assigned to the intervention group and 81 patients to the control group separately. The data were collected on participant demographics, medical information of the participants, and data on knowledge regarding the use of MDIs with a questionnaire comprising 21 multiple-choice questions (see Appendix A). The checklists (Appendix B) were used to observe the practice of the use of MDIs by the participants; two checklists were used for observing the use of MDIs with a spacer (20 steps) and without a spacer (21 steps). The tools for data collection and video were validated by experts. The tools were tested for reliability using kr-20 and Cronbach’s alpha reliability coefficients. The tools were found to be reliable, with a reliability value of 0.75 for the knowledge questionnaire and 0.86 for the checklist.
Intervention
Participants who were eligible as per the inclusion criteria were randomly assigned to the intervention group that received video-assisted teaching intervention on knowledge and practice regarding the use of MDIs and the control group that received routine information from the health personnel, as depicted in Figure 1. The video included a demonstration of an MDI with a spacer and without a spacer with the help of audio-visual aids, such as charts and a PowerPoint presentation. A live commentary of the steps was explained in the video, divided into three parts, i.e., pre-procedure, during procedure, and post-procedure. The videos were made in three languages, viz., English, Hindi, and Marathi. The intervention was provided by a trained nurse researcher; a pre-test was conducted using the knowledge questionnaire and practice checklist. The participants were provided with video-assisted teaching on the same day. A post-test was conducted on the eighth day of the intervention.
Schematic presentation of the research design
Statistical analysis
Data analysis was computed using descriptive and inferential statistics. Participant demographics and medical characteristics were described using frequency and percentage. The comparative statistical analysis was done using a paired t-test, a two-sample t-test, and a chi-square test. In the tests of significance, a p-value less than 0.05 was used. IBM SPSS Statistics for Windows, version 23.0 (released 2015, IBM Corp., Armonk, NY) was used in the analysis.
Results
A total of 162 participants were included in the intervention group (n = 81) and control group (n = 81). The results are described in sections on frequency and percentage distribution of demographic data, followed by the knowledge and practice levels of the participants in the intervention group and control group. The analysis also includes pre-test and post-test scores assessed before and after the intervention in the intervention group, as well as a comparative analysis depicting the knowledge and practice for both the intervention and control groups.
Table 1 depicts the demographic variables; out of the total participants, the majority were below 30 years of age in both groups. As per gender, the majority were females in the intervention group, i.e., 39 (48.1%), and the control group, i.e., 41 (50.6%). Regarding education, in both groups, the maximum participants had diploma-level education (31 (38.3%) and 32 (39.5%), respectively). The majority in the intervention group were professionals, i.e., 32 (39.5%), and 34 (42%) from the control group were engaged in technical work. The majority belonged to nuclear families from both groups. Thirty-nine (48.1%) participants from the intervention group and 33 (40.7%) participants from the control group had information regarding the use of MDIs. Social media was the most popular source of information as compared to doctors, nurses, or friends.
The medical characteristics of the participants, as shown in Table 2, show that in both groups, 44 (54.3%) participants were diagnosed with asthma and 37 (45.7%) with COPD; the majority were diagnosed with asthma for a duration of more than two to three years. From both groups, the maximum participants did not use MDIs with spacers, and the majority of them were using inhalers for a period of more than one to two years. Regarding the frequency of the use of inhalers, in the intervention group, the majority, i.e., 24 (29.6%), were using inhalers twice a day, whereas 33 (40.8%) in the control group were using inhalers once a day.
The pre-test knowledge regarding the use of an MDI among patients with obstructive respiratory disorders before video-assisted teaching, as presented in Table 3, shows that in both the intervention and control groups, the majority of participants had poor knowledge, i.e., 28 (34.57%) and 26 (32.1%), respectively.
The pre-test practice regarding the use of MDIs among patients with obstructive respiratory disorders before video-assisted teaching, as depicted in Table 4, in both the intervention and control groups, show that majority had poor practice scores, i.e., 30 (37.03%) and 36 (44.44%), respectively. Participants from both groups had scored low for the category of very good practices, i.e., 13 (16.05%) and 12 (14.81%) in the intervention and control groups, respectively.
The knowledge scores of the pre-test and post-test after the intervention as presented in Figure 1 shows that in the intervention group, in the pre-test, 28 (34.57%) participants had poor knowledge, 20 (24.69%) participants had average knowledge, 15 (18.52%) participants had good knowledge, and 18 (22.22%) had very good knowledge. In the post-test, 17 (20.90%) participants had poor knowledge, 16 (19.90%) participants had average knowledge, 26 (32.20%) participants had good knowledge, and 22 (27%) participants had very good knowledge. The majority of participants had good knowledge after the intervention.
Distribution of pre-test and post-test knowledge scores before and after video-assisted teaching in the intervention group N = 81 (intervention group), 81 (control group)
The practice scores of the pre-test and post-test before and after the intervention are presented in Figure 2. In the intervention group, pre-test scores showed that 30 (37.03%) participants had poor scores, 18 (22.22%) participants had average scores, 20 (24.7%) participants had good scores, and 13 (16.05%) participants had very good scores. In the post-test, maximum, i.e., 28 (34.7%), scored good, 26 (32%) scored very good, whereas 15 (18.5%) scored average and 12 (14.8%) scored poor on the scale for practices.
Distribution of the pre-test and post-test practice scores before and after video-assisted teaching in the intervention group N = 81 (intervention group), 81 (control group)
The effectiveness of video-assisted teaching on knowledge and practices regarding the use of MDIs in the intervention group of patients with obstructive respiratory disorders is depicted in Table 5. The mean of the pre-test knowledge score was 10.81, the SD was 8.28, the t-value was -14.65, and the p-value was 0.001. The mean of the pre-test practice score was 11.48, the SD was 4.36, the t-value was -17.97, and the p-value was 0.001. Thus, there was a significant difference between knowledge and practices regarding the use of MDIs in the intervention group of patients with obstructive respiratory disorders before and after the intervention at the 0.05 level of significance as calculated by the paired t-test. The p-values for both knowledge and practice were less than 0.05. Hence, the null hypothesis that no significant difference between the pretest and post-test scores for knowledge and practice regarding the use of MDIs exists was rejected.
Table 6 depicts a comparison between the knowledge of the intervention and control groups that was calculated with an unpaired t-test. The post-test mean of the intervention group was 13.88, and the SD was 4.36; the post-test mean of the control group was 14.72 and the SD was 8.72. The t-value was -19.43 and the p-value was 0.001. The null hypothesis that there was no significant difference between knowledge regarding the use of MDIs among the intervention and control groups of patients with obstructive respiratory disorders at the 0.05 level of significance was rejected, as the p-value < 0.05.
Table 7 represents a comparison of practices regarding the use of inhalers between the intervention and control groups was calculated with an unpaired t-test. The post-test mean of the intervention group was 15.67 and the SD was 4.36, and the post-test mean of the control group was 7.91 and the SD was 5.6. The t-value was -18.7 and p-value was 0.001, which was significant at the 0.05 level of significance. Thus, there was a statistically significant difference in both groups (p < 0.05). The null hypothesis that there was no significant difference between practice regarding the use of MDIs among the intervention and control groups of patients with obstructive respiratory disorders at the 0.05 level of significance was rejected.
There was a significant difference between the intervention and control groups of patients with obstructive respiratory disorders for knowledge and practices regarding the use of MDIs at the 0.05 level of significance; thus, the null hypothesis was not accepted.
The association between pre-interventional knowledge and practices regarding the use of MDIs among patients with obstructive respiratory disorders with selected sociodemographic variables was calculated using a chi-square test. The association between pre-interventional knowledge of patients and their demographic variables of age (years), gender, occupation, education, type of family, information regarding the use of MDIs earlier, source of information, diagnosis, duration of illness, use your inhaler, its duration of use, and frequency of use; no significant association was found as p > 0.05. Similarly, no significant association was found between the pre-interventional practices of patients and their demographic variables (p > 0.05) except for the variable of duration of illness. Thus, the null hypothesis was accepted for knowledge and for practices except for the variable of duration of illness (p = 0.036).
Discussion
Utilization of videos for teaching improves comprehension, cognitive ability, and skills [7]. When used in patient education, they are effective tools for their understanding about the health conditions, and compliance to the treatment is improved as it includes visual and audio explanations. This study incorporated a video to educate patients with obstructive respiratory disorders about MDIs. The intervention group demonstrated a significant improvement in knowledge and practice about its use, as evidenced by improved knowledge and practice scores post-intervention. A comparison of the mean scores of both the intervention and control groups showed a significant difference between the two groups, with the unpaired t-test values and p < 0.05 rejecting the null hypotheses. The findings were relatable to studies that have focused on similar strategies to have improved patient outcomes.
To overcome the problem of incorrect use of inhalers, Al-Kharouf et al. (2023) did a prospective and randomized controlled trial involving 103 asthmatic patients: 51 in the intervention group and 52 in the control group. The patients received intervention of a video-based teach-to-goal strategy, whereas the control group received a verbal education. There was an improvement in the use of inhaler technique in the intervention group (93.4%) in comparison to the control group (49.5%) (p < 0.05). The quality of life was significantly improved at a follow-up assessment [8].
A comparative study by S. F. Tafti et al. (2019) on individual and traditional bedside MDI use and group teaching with video demonstration involved 32 patients who received traditional teaching and 60 patients who received video teaching. In the traditional group, the mean age was 53 years and 20 were males. In the group that received demonstration of videos, the mean age was 62 years and 54 were males. The two groups did not significantly differ in the correct explanation of MDI use by phone interviews (p > 0.05). However, the two groups did statistically differ in age group and Saint George Respiratory Questionnaire scores at the beginning of the study (p < 0.004) [9].
Interestingly, video-based education has proved effective in patients with other health conditions too. A study by E. R. Miller et al. (2021) conducted a quality improvement program at a primary care clinic in Saudi Arabia that enrolled 269 adults with elevated levels of blood pressure who were not prescribed anti-hypertensive medications and utilized short, animated videos, as well as web-linked diet lifestyle intervention. Of the participants, 77% were males and 33% were females, and the average age was 41.6 years. A high level of engagement was demonstrated after the intervention. Those who return demonstrated a considerable reduction in systolic BP levels, i.e., -10.5 mm Hg from the baseline readings of 138.0 (7.2) mm Hg, which was a significant change (p < 0.001) [10].
In an article by N. Balasubramanian et al. (2018) on evaluating the implementation of a VATM, i.e., video-assisted teaching module regarding home care of schizophrenic patients, the authors provided intricate steps and process details of the preparation of the teaching material. Such a module demonstrated a reduction in burden of the caregivers with improved patient care, effective coping, and adjustment with developing good skills in patient care at home [11].
The review of the literature mentions the use of novel techniques other than the written or verbal methods of patient education improves patient adherence to the therapies and has better health outcomes [12]. Mastering the appropriate inhaler technique is directly correlated to better control of the clinical symptoms and reduced exacerbations of the disease. The results of the study go in line with the findings of the studies done on patients with obstructive respiratory disorders and on those with other chronic conditions like hypertension or psychiatric conditions. The explanation about the use of the inhaler in patient-friendly language made it more comprehensible for the patients understanding. The one-to-one interaction with the patients also helped in better engagement of the patients, which was evident from the practice score that was assessed with a checklist that checked for the steps followed sequentially as per the appropriate and effective use of the inhaler device and had a better learning outcome. Future opportunities could be researching therapy adherence aspects by utilizing qualitative methodologies and conducting randomized clinical trials with the use of modern patient teaching technologies.
The researchers do identify certain limitations of the study. The study included only one follow-up observation of the demonstration of MDIs in patients with obstructive respiratory disorders. Thus, repeated teaching, self-motivation levels of patients, and patient self-care education were not included. The patients visiting outpatient department were only included in the study and were from the geographical location of Navi Mumbai. Thus, the findings may not be generalized.
Conclusions
The results of the study showed a notable improvement in both knowledge and practice regarding the use of MDIs in the patients from the intervention group. Thus, the intervention was found to be a useful aid for better understanding the technique of using MDIs. The findings highlight a positive impact of the video-assisted teaching regarding the knowledge and practice of MDIs, as found by the statistically significant differences between the pre-test and post-test scores among the intervention group. Thus, it can be concluded that patient teaching utilizing both audio and visuals has a greater impact as compared to routine health education. However, no significant association was found between the pre-interventional knowledge of patients and their demographic variables of age (years), gender, occupation, education, type of family, information regarding the use of MDIs earlier, source of information, diagnosis, duration of illness, use of inhaler, its duration of use, and frequency of use. No significant association was found between the pre-interventional practices of patients and their demographic variables except for the variable of duration of illness. Thus, the null hypothesis was accepted for knowledge and for practices except for the variable of duration of illness.
Patient education can be enriched for chronic pulmonary patients and asthmatics, particularly in using medications via inhalers for achieving control of the symptoms and better pulmonary compliance. This study examined the impact of video-assisted teaching of the correct technique of the use of an MDI that was developed by a nurse who plays a pivotal role in patient care and educating them for better adherence to the treatment. The findings suggest potential for the cost-effective use of newer technologies, especially when there is easy availability of mobile-based technology to all globally. The study highlights the need for nurses to use newer and more interactive methods to improve the benevolence, adherence to treatment, and better quality of life of patients having chronic obstructive respiratory disorders.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary Eur Respir J AgustíA Celli BR Criner GJ 61202310.1183/13993003.00239-2023 PMC 1006656936858443 · doi ↗ · pubmed ↗
- 2Is manual therapy of the diaphragm effective for people with obstructive lung diseases? A systematic review Respir Med Res Tsimouris D Arvanitidis M Moutzouri M 101002832023 https://www.sciencedirect.com/science/article/pii/S 25900412230001443702789510.1016/j.resmer.2023.101002 · doi ↗ · pubmed ↗
- 3Brunner & Suddharth’s: textbook of medical-surgical nursing Smeltzer C Bare G Hinkle J Chicago Wolters Kluwer 2002 https://books.google.com.ph/books?hl=en&lr=&id=Smtj SD 1x 688C&oi=fnd&pg=PA 1295&dq=Brunner+%26+Suddharth%E 2%80%99s:+Textbook+of+Medical-Surgical+Nursing&ots=clm 8hd 2N 9V&sig=z Jnsj SRZ Ddme YN Kn 6T Njf Dxao MY&redir_esc=y#v=onepage&q=Brunner%20%26%20Suddharth%E 2%80%99s%3A%20Textbook%20of%20Medical-Surgical%20Nursing&f=false
- 4Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability Eur Respir J Giraud V Roche N 2462511920021186600410.1183/09031936.02.00218402 · doi ↗ · pubmed ↗
- 5Problems with inhaler use: a call for improved clinician and patient education Respir Care Fink J Rubin B 1360137450 (10)2005 https://www.liebertpub.com/doi/10.4187/respcare.0550136016185371 · pubmed ↗
- 6Confidence of nurses with inhaler device education and competency of device use in a specialised respiratory inpatient unit Chron Respir Dis Swami V Cho JG Smith T Wheatley J Roberts M 147997312110022411820213373919410.1177/14799731211002241 PMC 7983467 · doi ↗ · pubmed ↗
- 7Video-assisted instruction improves the success rate for tracheal intubation by novices Br J Anaesth Howard-Quijano KJ Huang SL Matevosian R 5685721012008 https://www.bjanaesthesia.org/article/S 0007-0912(17)34174-0/fulltext 1867641810.1093/bja/aen 211 · doi ↗ · pubmed ↗
- 8Video-based teach-to-goal intervention on inhaler technique on adults with asthma and COPD: a randomized controlled trial P Lo S One Al-Kharouf MS Abdeljalil MH Obeidat NM Oweidat KA Awwad O 018202310.1371/journal.pone.0286870 PMC 1025622837294823 · doi ↗ · pubmed ↗