The treatment effect of rehabilitation gymnastics on postoperative rehabilitation in elderly patients with lumbar spinal stenosis
Yushan Guo, Xianghui Wang, Yingtao Shi

TL;DR
This study shows that combining rehabilitation gymnastics with compression therapy helps elderly patients recover faster after lumbar spinal stenosis surgery, but the benefits fade by 3 months.
Contribution
The study demonstrates the short-term benefits of integrating rehabilitation gymnastics with compression therapy for postoperative recovery in elderly patients.
Findings
The intervention group had significantly reduced DVT incidence and lower pain scores at 2 weeks and 1 month post-surgery.
Patients in the intervention group showed higher functional scores and satisfaction rates early after surgery.
The benefits of the intervention were not sustained by the third month post-surgery.
Abstract
This study sought to evaluate the impact of integrating rehabilitation gymnastics with compression therapy on postoperative recovery outcomes in elderly patients undergoing surgery for lumbar spinal stenosis. Patients aged ≥65 years hospitalized for lumbar spinal stenosis between July 2016 and July 2018 were included. Eighty-four patients receiving postoperative rehabilitation gymnastics and compression therapy were assigned to the intervention group, while 84 matched controls received standard care alone. Both groups underwent routine postoperative management. Clinical outcomes were assessed at 2 weeks, 1 month, and 3 months post-surgery using measures including lower-extremity deep venous thrombosis (DVT) incidence, visual analog scale (VAS) pain scores, Oswestry Disability Index (ODI), Japanese Orthopaedic Association (JOA) scores, and patient satisfaction rates. The intervention…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
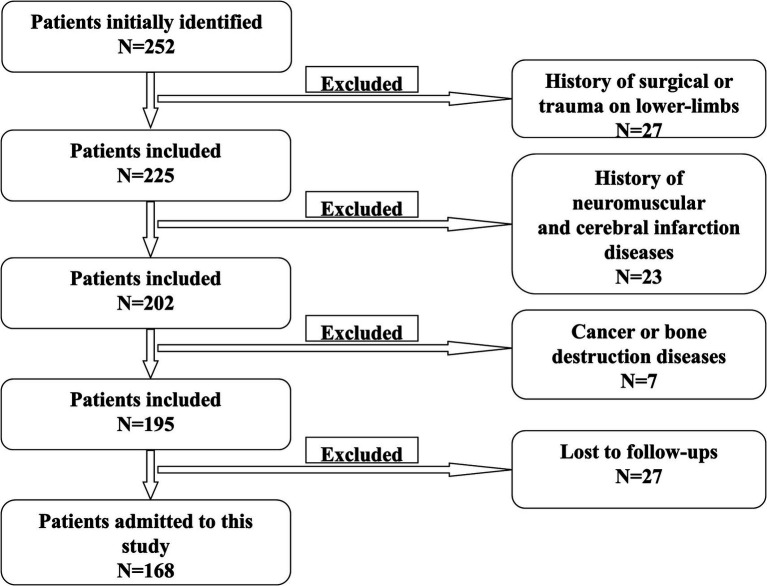 Figure 1
Figure 1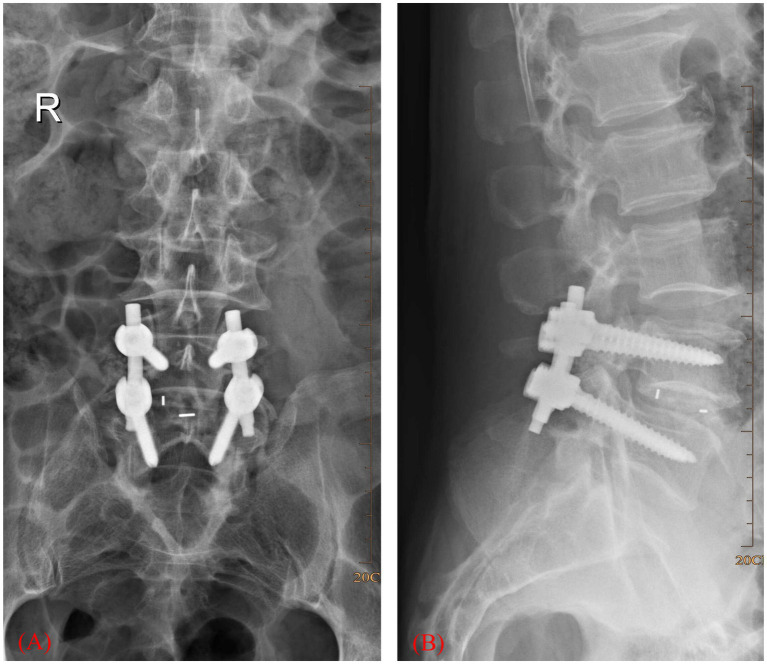 Figure 2
Figure 2| After surgery | Intervention ( | Control ( | Chi-square test | |
|---|---|---|---|---|
| Non-DVT/ DVT | Non-DVT/ DVT | χ2 |
| |
| 2 weeks | 79 cases/5 cases | 71 cases/13 cases | 3.98 |
|
| 1 month | 81 cases/3 cases | 74 cases/10 cases | 4.09 |
|
| 3 months | 83 cases/1 cases | 78 cases/6 cases | 2.39 | 0.122 |
| After surgery | Intervention ( | Control ( | Student’s | |
|---|---|---|---|---|
| Mean± SD | Mean± SD |
|
| |
| 2 weeks | 3.32 ± 1.61 | 5.10 ± 1.21 | 8.11 |
|
| 1 month | 2.01 ± 0.95 | 3.40 ± 1.13 | 8.64 |
|
| 3 months | 1.45 ± 0.70 | 1.57 ± 0.76 | 1.05 | 0.295 |
| After surgery | Intervention ( | Control ( | Student’s | |
|---|---|---|---|---|
| Mean± SD | Mean± SD |
|
| |
| 2 weeks | 50.26 ± 3.79 | 55.98 ± 7.32 | 6.35 |
|
| 1 month | 30.32 ± 3.46 | 35.64 ± 7.12 | 6.16 |
|
| 3 months | 21.47 ± 3.20 | 21.94 ± 2.74 | 1.00 | 0.314 |
| After surgery | Intervention ( | Control ( | Student’s | |
|---|---|---|---|---|
| Mean± SD | Mean± SD |
|
| |
| 2 weeks | 14.21 ± 2.97 | 10.19 ± 4.00 | −7.40 |
|
| 1 month | 19.65 ± 3.09 | 16.81 ± 2.94 | −6.12 |
|
| 3 months | 25.57 ± 1.73 | 25.17 ± 1.87 | −1.45 | 0.148 |
| After surgery | Intervention ( | Control ( | Chi-square test | |
|---|---|---|---|---|
| Very satisfied/satisfied/dissatisfied | Very satisfied/satisfied/dissatisfied | χ2 |
| |
| 2 weeks | 36 cases/38 cases/10 cases | 28 cases/30 cases/26 cases | 9.052 |
|
| 1 month | 47 cases/33 cases/4 cases | 41 cases/28 cases/15 cases | 7.187 |
|
| 3 months | 52 cases/30 cases/2 cases | 49 cases/29 cases/6 cases | 2.106 | 0.349 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Musculoskeletal pain and rehabilitation · Shoulder Injury and Treatment
Introduction
Lumbar spinal stenosis (LSS), an important cause of chronic lower back pain, significantly impairs mobility and diminishes quality of life in affected individuals (1). Surgical intervention, particularly posterior lumbar fusion, is frequently employed to address spinal stenosis, with evidence supporting its superior efficacy over conservative treatments (2–8). While surgical precision remains a primary focus, postoperative complications, including lower-limb deep venous thrombosis (DVT), pose persistent challenges, particularly in elderly patients. Advanced age and prolonged postoperative bed rest, necessitated by degenerative conditions, heighten vulnerability to complications such as DVT, muscle atrophy, and nerve adhesions. Despite this elevated risk, research on optimizing recovery strategies for elderly LSS patients remains limited.
Current clinical guidelines advocate postoperative lower-limb rehabilitation exercises to mitigate complications. However, adherence to such regimens is often low among elderly patients due to discomfort and pain following surgery. To address this barrier, our study integrates compression therapy—a modality designed to enhance muscular contraction and relaxation, thereby improving circulation with structured rehabilitation gymnastics.
This investigation evaluates whether combining lower-limb rehabilitation gymnastics with compression therapy yields superior postoperative outcomes compared to conventional care in elderly LSS patients, focusing on functional recovery, complication prevention, and patient compliance.
Materials and methods
Ethics statement
This study was approved by the Ethics committee of North China Medical and Health Group Xingtai General Hospital. This is a retrospective case–control study in which we collected data and analyzed them anonymously without any potential harm to the patients. Thus, informed consent was waived by the ethics committee, given the retrospective design.
Patients and inclusion criteria
Medical records of elderly patients (aged ≥65 years) who underwent surgery because of lumbar spinal stenosis between July 2016 and July 2018 were collected. Figure 1 is a scheme showing the process of enrolling the patients in our study. Finally, 168 patients were recruited in our study, 84 in the intervention group and another 84 in the control group. There were 103 males and 65 females. The age was 68 ± 3 years on average. Figure 2 shows a postoperative X-ray image of the spine after the lumbar fusion surgery. The inclusion criteria for the patients in our study are listed as follows. 1. Patients underwent lumbar spinal fusion surgery; 2. no history of trauma or operation on the lower limbs; 3. no neuromuscular or cerebral infarction disease history; 4. no cancer or bone destruction diseases; 5. muscle strength of preoperative lower limbs was grade IV or grade V; 6. no preoperative lower-limb DVT; 7. no infection after surgery; 8. no nerve injury was observed. Patients that did not apply to these criteria were excluded from this study.
Scheme of patient selection.
X-ray image showing lumbar interbody fusion surgery. (A) Coronary plane. (B) Sagittal plane.
Group allocation and demographics
The cohort was divided into two age-matched groups (n = 84 each): an intervention group (54 males, 32 females) and a control group (47 males, 39 females). Both groups received standardized perioperative care, including routine nursing protocols, pharmacological management, and postoperative administration of low-molecular-weight heparin.
Intervention protocols
The intervention group underwent a 3-month regimen combining lower-limb rehabilitation exercises with compression therapy, while the control group received standard care alone. The rehabilitation exercise protocol was performed as follows (9).
- Initial Relaxation: Patients assumed a supine position for muscle relaxation.
- Lower-Limb Massage: A 5-min centripetal massage was administered to both limbs.
- Ankle Pump Exercise: Repeated flexion-extension of the ankles (5 s per movement, 50 repetitions/set, 3 daily sets).
- Knee-Pressing Exercise: Legs were fully extended while pressing knees downward (10-s holds, 20 repetitions/set, 3 daily sets).
- Straight Leg Raises: Active or passive elevation of lower limbs (30 repetitions/leg, 5 daily sets).
- Hip/Knee Flexion: Patients bent knees and hips to 30° flexion in a relaxed state (20 repetitions/set, 3 daily sets).
The POWER Q-1000 pneumatic device delivered sequential compression via air-filled leggings covering the lower limbs and thigh base. Parameters included: (1) limb compression: 40 mmHg pressure, 10 mmHg incremental steps, 8-s inflation intervals; (2) foot compression: 130 mmHg pressure, 10 mmHg steps, 5-s inflation intervals. Sessions lasted 30 min twice daily.
Follow-up and outcome measures
Postoperative assessments were conducted at 2 weeks, 1 month, and 3 months. Outcomes included: (1) patient satisfaction: stratified as “very satisfied,” “satisfied,” or “dissatisfied”; (2) clinical metrics: incidence of lower-limb DVT, Visual Analog Scale (VAS) pain scores, Oswestry Disability Index (ODI), and Japanese Orthopaedic Association (JOA) functional scores.
Statistical analyses
All statistical analyses were performed using SPSS 18.0 (IBM SPSS Inc., United States). Continuous variables were assessed for normality using the Shapiro–Wilk test (p > 0.10). Normally distributed data are presented as mean ± standard deviation (SD); non-normally distributed data are expressed as median (interquartile range, IQR). Parametric comparisons between groups were conducted using Student’s t-test for data meeting assumptions of normality and homogeneity of variance (Levene’s test). Non-parametric analyses employed the Mann–Whitney U test. Categorical variables—including deep venous thrombosis (DVT) incidence and patient satisfaction rates—were evaluated using Pearson’s chi-square test. A two-tailed p-value < 0.05 defined statistical significance.
Results
Lower limb DVT
As indicated in Table 1, two weeks after surgery, the incidence of lower limb DVT in the intervention group was lower than in the control group (χ^2^ = 3.982, p = 0.046). Similarly, at one-month post-surgery, the intervention group had a lower incidence of DVT compared to the control group (χ^2^ = 4.085, p = 0.043). However, by the third month, no significant difference in lower limb DVT was observed between the two groups (χ^2^ = 2.39, p = 0.122).
VAS score
Table 2 shows that the VAS scores were significantly lower in the intervention group than in the control group at both the second week and first month after surgery (t = 8.11, p < 0.001; t = 8.64, p < 0.001, respectively). However, no significant difference in VAS scores was found between the groups at the third month post-surgery (t = 1.05, p > 0.295).
ODI
As presented in Table 3, the ODI scores were lower in the intervention group than in the control group during the second week and first month after surgery (t = 6.35, p < 0.001; t = 6.16, p < 0.001, respectively). Nevertheless, by the third month, there was no significant difference in ODI scores between the intervention and control groups (t = 1.00, p = 0.314).
JOA score
As shown in Table 4, two weeks and 1 month after surgery, the JOA score was higher in the intervention group compared to the control group (t = −7.40, p < 0.001; t = −6.12, p < 0.001, respectively). However, by the third month post-surgery, no significant difference in JOA scores was observed between the intervention and control groups (t = −1.454, p = 0.148).
Satisfaction survey
According to Table 5, the satisfaction rate was higher in the intervention group compared to the control group at both the two-week and one-month marks after surgery (χ^2^ = 9.052, p = 0.011; χ^2^ = 7.187, p = 0.027, respectively). However, by the third month, no significant difference in satisfaction rates was observed between the two groups (χ^2^ = 2.106, p = 0.349).
Discussion
Lumbar spinal stenosis (LSS) in elderly patients is primarily attributed to degenerative pathologies such as lumbar disc herniation, ligamentum flavum hypertrophy, vertebral osteophytes, and spondylolisthesis (1). These conditions frequently result in debilitating symptoms, including chronic lower back pain and functional limitations, which markedly impair mobility and quality of life (2). Surgical decompression, often involving the removal of osteophytes, hypertrophic ligaments, and degenerative tissues, remains a standard intervention to alleviate neural compression (3–5).
In this study, we evaluated the efficacy of combining rehabilitation gymnastics with compression therapy to enhance postoperative recovery in elderly LSS patients. Compared to controls receiving standard care, the intervention group demonstrated superior short-term outcomes, including reduced lower-limb DVT incidence, VAS pain scores, improved ODI and JOA scores, and higher patient satisfaction at 2 weeks and 1 month postoperatively (all p < 0.05). However, these differences were no longer statistically significant by the third month. While both groups achieved comparable long-term recovery, the intervention group exhibited accelerated functional restoration during the critical early postoperative phase (e.g., reduced hospital stays, cost-effectiveness) despite transient effects.
The rising global prevalence of spinal surgery, particularly among aging populations, underscores the need for optimized rehabilitation strategies (10–13). LSS is now the leading indication for spinal surgery in elderly patients (3), with common techniques including decompressive laminectomy and fusion (14). Despite procedural advancements, functional recovery remains inconsistent, with studies reporting wide variability in success rates: patient satisfaction ranges from 15 to 81% (15–17), and functional improvement spans 58–69% (13, 18, 19). Postoperative complications, such as trunk muscle dysfunction, further complicate recovery (20), highlighting the importance of structured rehabilitation.
The clinical utility of postoperative rehabilitation, however, remains debated. Prior research indicates that home-based physiotherapy programs, including strength and flexibility exercises, fail to improve long-term functional outcomes (21). Similarly, rehabilitation protocols and educational interventions show limited impact on postoperative management in extended follow-ups (22). A randomized controlled trial with 1-year follow-up found no significant benefit from active rehabilitation in spinal fusion patients (23). These discrepancies may stem from non-standardized protocols and poor patient adherence, often due to postoperative pain. In contrast, our integrated approach—combining guided rehabilitation gymnastics to mitigate muscle atrophy with compression therapy to enhance circulation, addressed these barriers, yielding measurable early benefits over conventional care. Our findings show that rehabilitation gymnastics combined with compression treatment is effective for facilitating recovery after lumbar spinal surgery. Thus, we would suggest that this method of postoperative rehabilitation should be widely promoted in the clinic.
There are some limitations in this study. Firstly, it is difficult to avoid selection bias when selecting cases because of the retrospective study. Secondly, recall bias is difficult to avoid when obtaining medical record information. At last, considering the small sample size of only 168 patients from a single-center and the homogeneous demographics (e.g., age 68 ± 3 years), this may affect the generalizability of the findings and limit the applicability of this study to diverse populations. Thus, future multi-center studies with larger sample sizes are warranted to validate our findings.
In conclusion, our findings suggest that rehabilitation gymnastics paired with compression therapy accelerates early postoperative recovery in elderly LSS patients undergoing posterior lumbar fusion. This non-invasive strategy offers a pragmatic solution to enhance short-term outcomes, though its effects attenuate over time. Given the challenges of postoperative adherence and variable surgical success rates, this combined regimen represents a valuable adjunct to standard care. Future studies should explore protocol refinements to sustain long-term efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Atlas SJ Keller RB Wu YA Deyo RA Singer DE. Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the Maine lumbar spine study. Spine. (2005) 30:927–35. doi: 10.1097/01.brs.0000158954.68522.2a 15834338 · doi ↗ · pubmed ↗
- 2Aalto TJ Leinonen V Herno A Alen M Kröger H Turunen V. Postoperative rehabilitation does not improve functional outcome in lumbar spinal stenosis: a prospective study with 2-year postoperative follow-up. Eur Spine J. (2011) 20:1331–40. doi: 10.1007/s 00586-011-1781-y, PMID: 21523459 PMC 3175851 · doi ↗ · pubmed ↗
- 3Huo Y Ding W Rudd S Yang D Ma L Zhao R. Incidence and risk factors of lumbar plexus injury in patients undergoing oblique lumbar interbody fusion surgery. Eur Spine J. (2023) 32:336–44. doi: 10.1007/s 00586-022-07439-w, PMID: 36370208 · doi ↗ · pubmed ↗
- 4Chou R Baisden J Carragee EJ Resnick DK Shaffer WO Loeser JD. Surgery for low back pain: a review of the evidence for an American pain society clinical practice guideline. Spine. (1976) 2009:1094–109. doi: 10.1097/BRS.0b 013e 3181 a 105fc 19363455 · doi ↗ · pubmed ↗
- 5Li Z Gao X Ding W Li R Yang S. Asymmetric distribution of Modic changes in patients with lumbar disc herniation. Eur Spine J. (2023) 32:1741–50. doi: 10.1007/s 00586-023-07664-x, PMID: 36977942 · doi ↗ · pubmed ↗
- 6Deyo RA Gray DT Kreuter W Mirza S Martin BI. United States trends in lumbar fusion surgery for degenerative conditions. Spine. (1976) 30:1441–5. doi: 10.1097/01.brs.0000166503.37969.8a 15959375 · doi ↗ · pubmed ↗
- 7Deyo RA Mirza SK Martin BI Kreuter W Goodman DC Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. (2010) 303:1259–65. doi: 10.1001/jama.2010.338, PMID: 20371784 PMC 2885954 · doi ↗ · pubmed ↗
- 8Du Bois M Szpalski M Donceel P. A decade’s experience in lumbar spine surgery in Belgium: sickness fund beneficiaries, 2000-2009. Eur Spine J. (2012) 21:2693–703. doi: 10.1007/s 00586-012-2381-1, PMID: 22661202 PMC 3508248 · doi ↗ · pubmed ↗