Bilateral Renal Infarcts Due to Blunt Trauma in a Healthy Young Female Patient: A Case Report
Taylor Locklear, Alyssa McMandon, Rachel A Daley, Saptarshi Biswas

TL;DR
A healthy young woman developed rare bilateral kidney damage after a car accident, with no underlying health issues, and recovered with conservative treatment.
Contribution
This case report presents a rare instance of trauma-induced bilateral renal infarcts in a healthy young female.
Findings
The patient had bilateral renal infarcts following blunt trauma with no prior medical conditions.
Imaging confirmed multiple injuries, including fractures and kidney damage, but no underlying vascular or clotting disorders.
The patient recovered with conservative management and no long-term complications were observed.
Abstract
Bilateral renal infarcts due to blunt trauma in the absence of underlying pathology are a rare condition. Trauma-induced renal infarction occurs due to decreased perfusion to the renal system. A 23-year-old woman with no significant past medical history presented to the emergency department with abdominal pain after being struck by a car as a pedestrian. She reported abdominal pain, shoulder pain, and pelvic pain. Imaging revealed multiple traumatic injuries, including a right shoulder dislocation, vertebral and pelvic fractures, and bilateral renal infarcts. Extensive workup, including echocardiography, renal ultrasound, magnetic resonance angiography, and hypercoagulability testing, was unremarkable. The findings were attributed to transient renal hypoperfusion secondary to trauma-related vascular dysfunction. Her symptoms resolved with conservative management, and she was discharged…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1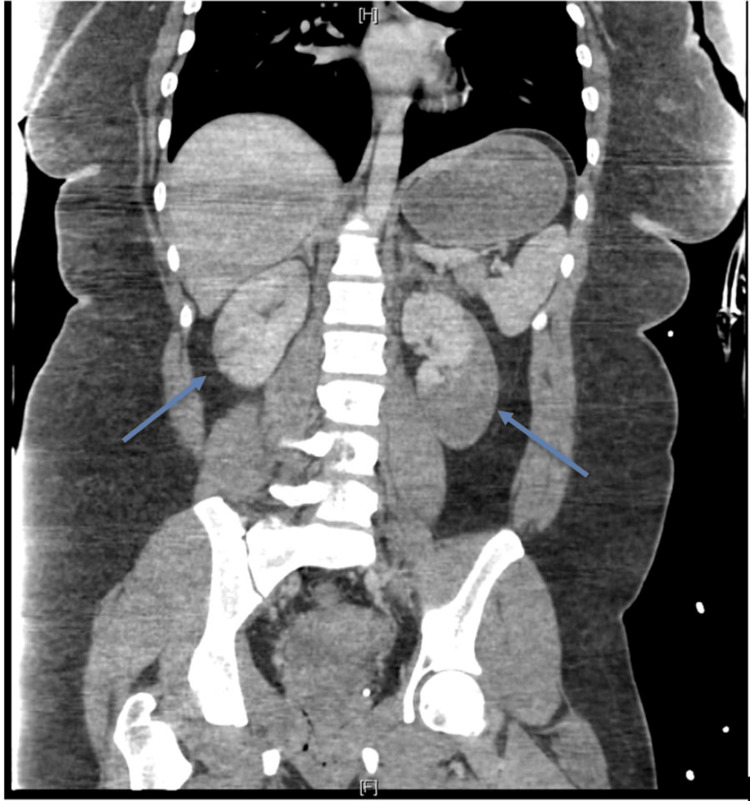 Figure 2
Figure 2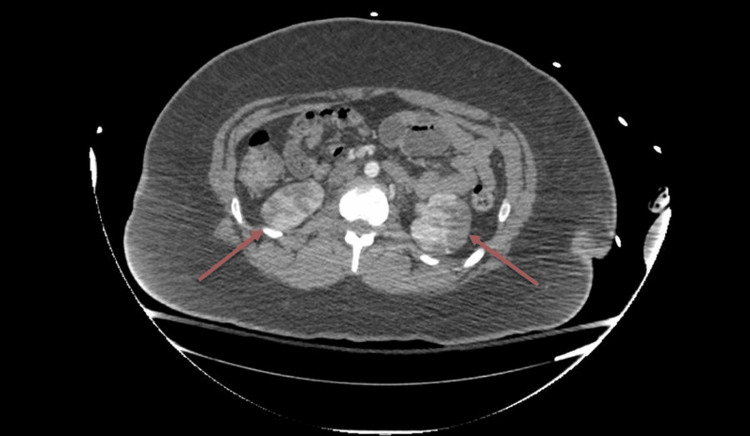 Figure 3
Figure 3| Variable | Value | Normal Range |
| Temperature | 98.1 ˚F | 97-99 ˚F |
| BP | 115/79 mmHg | <120/80 mmHg |
| HR | 116 bpm | 60-100 bpm |
| RR | 17 | 12-20 (breaths per minute) |
| Pulse Oximetry | 98% | 95-100% O2 |
| Variables | Result | Units | Reference |
| Immunology Panel | |||
| ANA | Negative | Negative | |
| c-ANCA | <0.2 | AI | 0.0-0.9 |
| p-ANCA | <0.2 | AI | 0.0-0.9 |
| Complement C3 | 144 | mg/dL | 82-167 |
| Complement C4 | 31 | mg/dL | 12-38 |
| Kidney Function | |||
| On Admission | |||
| Creatinine | 1.2 | mg/dL | 0.7-1.5 |
| BUN | 17 | mg/dL | 7-20 |
| GFR | >=60 | >=60 | |
| On Discharge | |||
| Creatinine | 0.9 | mg/dL | 0.7-1.5 |
| BUN | 15 | mg/dL | 7-20 |
| GFR | >=60 | >=60 | |
| Coagulation | |||
| PT | 12.5 | seconds | 9.8-13.9 |
| INR | 1.05 | 0.9-1.1 | |
| APTT | 26.9 | seconds | 24.9-37.9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Urological Disorders and Treatments · Pediatric Urology and Nephrology Studies
Introduction
Renal infarction is a rare but serious ischemic event that results from the occlusion of the main renal artery or its branches, potentially progressing to acute kidney injury, impaired glomerular filtration rate, end-stage renal disease, or death [1]. This condition can arise from various causes, the most common being cardiogenic [1]. Other causes, in no particular order, include renal artery injuries, hypercoagulable state, or idiopathic [1]. Despite its potentially severe clinical implications, renal infarction remains an uncommon diagnosis, with an estimated incidence of 0.004% among patients presenting to the Emergency Department [2]. The condition may often go unrecognized due to its nonspecific clinical presentation and overlap with more common causes of flank pain or abdominal discomfort. Although a rare condition, CT imaging with contrast, along with a detailed history and physical examination, is the best initial approach to identifying trauma-induced renal injury or a pre-existing renal pathology [3]. This case report presents an incidental discovery of bilateral renal infarcts in a trauma patient without any known predisposing medical conditions, including cardiac arrhythmia or coagulopathy. The absence of these risk factors underscores the importance of considering transient renal ischemic changes in the context of blunt abdominal trauma and highlights the need for further investigation into their pathophysiology and clinical implications.
Case presentation
A 23-year-old woman with no significant past medical history presented to the emergency department as a Level 2 trauma activation after being struck by a car as a pedestrian. She experienced a brief loss of consciousness but was hemodynamically stable upon arrival, with mild tachycardia (Table 1) and a Glasgow Coma Scale (GCS) of 15. Primary survey revealed a patent airway, adequate breathing, and hemodynamic stability. Notable findings included a right shoulder dislocation and abrasions to the right shoulder. An Extended Focused Assessment with Sonography in Trauma (eFAST) exam was negative for free fluid. She endorsed abdominal pain, right shoulder pain, and left hip pain but denied dysuria, hematuria, fever, chills, nausea, vomiting, joint pain, or leg swelling.
The right shoulder dislocation was successfully reduced, and orthopedic evaluation was obtained with imaging revealing multiple traumatic injuries, including a nondisplaced left posterior iliac bone fracture, a left S1 transverse process fracture, and small avulsion fractures on the left calcaneus and navicular.
Obstetric and gynecologic (OBGYN) history included pre-eclampsia and a prior C-section at 37 weeks. She also had a history of gonorrhea and chlamydia. A transabdominal ultrasound identified an intrauterine pregnancy with a gestational sac (Figure 1) estimated at five weeks and six days with no gestational pole and possible small subchorionic hemorrhages (< 25%). She was diagnosed with a threatened abortion with a high likelihood of nonviability and scheduled a follow-up with her OBGYN upon discharge.
Ultrasound image of intrauterine pregnancyUltrasound showing an intrauterine pregnancy with the gestational sac indicated by yellow markers
Further imaging with contrast-enhanced computed tomography (CT) showed bilateral renal infarcts (Figures 2, 3) with a high suspicion for focal intimal injury in the main left renal artery, while the right renal artery appeared normal. These findings raised concern for a potential vascular injury from blunt trauma. Given the acute presentation and concern for serious underlying pathology, the patient was admitted for close monitoring and underwent an extensive diagnostic work-up to rule out vasculitis and cardioembolic etiologies. Initial laboratory tests, including complete blood count, basic metabolic panel, erythrocyte sedimentation rate, and urinalysis, were unremarkable. Additional testing, including echocardiogram, renal ultrasound, magnetic resonance angiogram of the abdomen, vasculitis panel, and hypercoagulable work-up, did not reveal any underlying pathology. There was no reported family history of renal disease or thrombophilia (Table 2).
Contrast-enhanced coronal-view CT scan showing bilateral renal infarctsThe blue arrows point to the infarcted right and left kidneys
Contrast-enhanced axial-view CT scan also demonstrating bilateral renal infarctsThe red arrows point to the right and left infarcted kidneys on the axial-view CT scan
Given the absence of systemic causes, her renal hypoperfusion was considered secondary to transient hypoperfusion from blunt trauma. Throughout her hospitalization, she was managed conservatively with pain control, orthopedic monitoring, and urologic surveillance. Fluoroscopy exposure was limited due to pregnancy. She remained hemodynamically stable and was discharged with outpatient follow-up appointments scheduled with obstetrics and orthopedics.
Discussion
Bilateral renal infarcts without an apparent etiology in a trauma patient represent a consequence of blunt abdominal trauma. While renal infarction may present with abdominal or flank pain, nausea, and vomiting, these symptoms are nonspecific and present in many other conditions [4]. Laboratory findings often include elevated lactate dehydrogenase levels, which serve as a marker of tissue ischemia, though our patient’s laboratory work-up was unremarkable.
Renal infarction can be caused by blockage of arterial or venous drainage; arterial blockage is more common than venous abnormalities [5]. Trauma-related renal infarction is a distinct entity and is a result of direct vascular injury, vasospasm, or transient hemodynamic instability that may contribute to renal hypoperfusion [6]. The most common cause of traumatic renal injury is decreased perfusion from hypotension caused by hemorrhage [7]. Blunt force trauma can cause endothelial damage, leading to vessel damage and infarction [8]. Additionally, vasospasm can occur after blunt trauma, similar to how it occurs in endovascular procedures. Vasospasm is a protective mechanism following vascular insult, which causes narrowing of the arteries, reducing renal perfusion [8,9].
Contrast-enhanced CT is the imaging modality of choice for diagnosing renal infarction, as early detection is important due to the short lifespan of the affected renal parenchyma [10]. The most common finding for renal infarct on CT imaging is a hypoattenuated area with an associated mass effect, followed by the “cortical rim sign”, which suggests preserved perfusion to the renal cortex via collateral vessels [5]. In this case, the bilateral nature of the infarcts and absence of a clear embolic or pathologic cause raises the suspicion of transient renal hypoperfusion due to trauma-related vascular dysfunction.
Trauma is the presumed etiology in this case; alternative causes of bilateral renal infarction must also be considered. Other etiologies include thromboembolic events, hypercoagulable states, or renal artery pathology [1,11]. The extensive work-up, including echocardiogram, vasculitis panel, and hypercoagulability testing, was unremarkable, making these alternative diagnoses less likely. Most trauma-induced renal infarcts resolve without long-term sequelae; some potential complications are chronic kidney disease, renal atrophy, or hypertension due to ischemic injury to the renal tissue [12,13]. Treatment of renal hypoperfusion can vary based on the presentation of the patient. Overall, the goal is to maintain adequate renal perfusion while avoiding fluid overload [14].
Conclusions
Bilateral renal infarction identified on an abdominal contrast-enhanced CT scan without any underlying comorbid condition is an exceptionally rare finding, particularly in a healthy female patient following blunt abdominal trauma. This case highlights a benign and likely transient episode of bilateral renal hypoperfusion, detected incidentally through imaging performed during trauma evaluation. While symptoms were nonspecific, imaging modalities such as contrast-enhanced CT were critical in ruling out more concerning pathologies, including thromboembolic events and vascular injuries. The patient’s clinical course remained stable, with spontaneous resolution and no evidence of long-term renal impairment. This case underscores the importance of including renal hypoperfusion in the differential diagnosis following trauma and suggests that, in select cases after an appropriate work-up, conservative management with close monitoring is a safe and effective approach due to the potential for sequelae of more serious conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical characteristics and outcomes of renal infarction Am J Kidney Dis Oh YK Yang CW Kim YL 2432506720162654563510.1053/j.ajkd.2015.09.019 · doi ↗ · pubmed ↗
- 2ED presentations of acute renal infarction Am J Emerg Med Huang CC Lo HC Huang HH 1641692520071727680510.1016/j.ajem.2006.06.010 · doi ↗ · pubmed ↗
- 3Renal traumas in nephrologic patients Imaging in Nephrology Scuderi M Mannino M Schembari E Terranova W Urzia V 125133 Cham Springer 2021
- 4Acute renal infarction: a case series Clin J Am Soc Nephrol Bourgault M Grimbert P Verret C 392398820132320424210.2215/CJN.05570612 PMC 3586969 · doi ↗ · pubmed ↗
- 5CT features of renal infarction Eur J Radiol Suzer O Shirkhoda A Jafri SZ Madrazo BL Bis KG Mastromatteo JF 59644420021235041410.1016/s 0720-048x(01)00476-4 · doi ↗ · pubmed ↗
- 6Advancements in trauma-induced acute kidney injury: diagnostic and therapeutic innovations Life (Basel) Lassola S Cundari F Marini G Corradi F De Rosa S 10051420243920274710.3390/life 14081005 PMC 11355063 · doi ↗ · pubmed ↗
- 7Renal artery injury secondary to blunt abdominal trauma - two case reports Pol J Radiol Ahmed Z Nabir S Ahmed MN Al Hilli S Ravikumar V Momin UZ 572577812016 https://pmc.ncbi.nlm.nih.gov/articles/PMC 5181523/2805807110.12659/PJR.899710 PMC 5181523 · doi ↗ · pubmed ↗
- 8Severe spasm of the renal artery after blunt abdominal trauma simulating end-organ infarction Case Rep Med Ucar A Yahyayev A Agayev A 207152201020102120980810.1155/2010/207152 PMC 3014801 · doi ↗ · pubmed ↗