Testosterone Levels in Transgender Women Undergoing Gender-Affirming Hormone Therapy
Emily W Miro, Katherine Rizzone, Kory Ford, Tiffany F Ho, Erika Sullivan, Bayarmaa Mark, Masaru Teramoto, Dan Cushman

TL;DR
This study examines how testosterone levels change in transgender women undergoing hormone therapy and compares these levels to sports eligibility guidelines.
Contribution
The study provides empirical data on testosterone suppression in transgender women following standard hormone therapy regimens.
Findings
After 12 months on GAHT, the median testosterone level was 0.52 nmol/L, and the mean was 3.39 nmol/L.
After 24 months on GAHT, the median testosterone level was 0.43 nmol/L, and the mean was 3.90 nmol/L.
Abstract
The participation of transgender women in women’s sports is a topic rife with controversy and lacks a unified set of guidelines. Testosterone thresholds vary widely between organizations, ranging from less than 2.5 nmol/L to less than 10 nmol/L during a pre-competition period of 12 to 24 months. Little is known about how quickly and to what degree testosterone is suppressed below the thresholds required for participation in women’s sports after the initiation of gender-affirming hormone therapy (GAHT). This study examined trends in testosterone levels among transgender women undergoing the current standard of care GAHT and compared these values to existing guidelines for participation in women’s sports. After 12 months on GAHT, the median testosterone level was 0.52 nmol/L (95% CI: 0.47-0.73), and the mean was 3.39 nmol/L (95% CI: 2.63-4.15) (N=261). After 24 months, the median…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
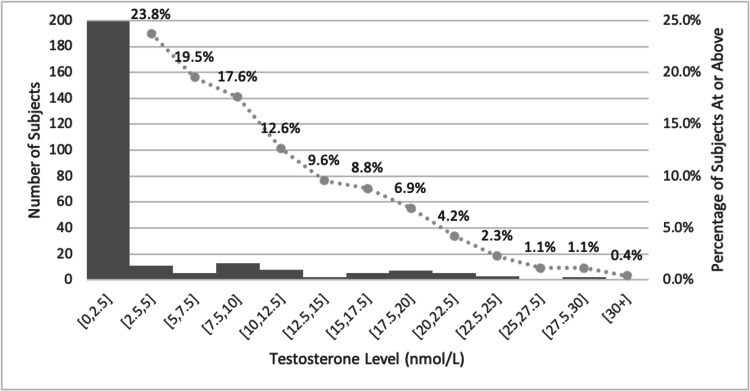 Figure 1
Figure 1| ICD-9 diagnostic code | ICD-10 diagnostic code |
| 302.50: trans-sexualism with unspecified sexual history (aka “trans-sexualism not otherwise specified”) | F64.0: transsexualism |
| 302.51: trans-sexualism with asexual history | F64.1: dual role transvestism |
| 302.52: trans-sexualism with homosexual history | F64.2: gender identity disorder of childhood |
| 302.53: trans-sexualism with heterosexual history | F64.8: other gender identity disorders |
| 302.60: gender identity disorder in children | F64.9: gender identity disorder, unspecified |
| 302.85: gender identity disorder in adolescents or adults | Z87.890: personal history of sex reassignment |
| Timing | Medication and recommendations |
| Initial dose | Estradiol: |
| Oral estradiol: 2 mg by mouth daily | |
| Injectable estradiol valerate (20mg/mL): 1-2 mg weekly | |
| Transdermal estradiol: 0.1 mg twice weekly | |
| Spironolactone: 25-50 mg daily | |
| After one month | Estradiol: |
| Oral estradiol: increase estradiol to 2 mg by mouth twice daily | |
| Injectable estradiol valerate: increase by 1 mg increments | |
| Transdermal estradiol: increase by 0.1 mg increments | |
| Spironolactone: increase by 50 mg increments to 200 mg by mouth daily | |
| Three months after starting hormones | Check labs. If labs are not within the desired range (estradiol 100-200 pg/mL and testosterone <50 ng/dL): |
| Increase oral estradiol to 5 or 6 mg total daily dosing (typically 2-3 mg AM/3 mg PM) | |
| Increase spironolactone to the maximum dose of 400 mg daily | |
| Every three months | Check labs. If labs are not in the desired range: |
| Increase oral estradiol typically to a max of 6mg total daily dose | |
| Increase spironolactone to the maximum dose of 400 mg daily |
| Timing | Laboratory tests |
| Baseline | Basic metabolic panel or CMP if using spironolactone |
| First year (or when making dose adjustment) | Estradiol |
| Total testosterone | |
| CMP | |
| Semi-annually or annually for years >1 | Estradiol |
| Total testosterone | |
| CMP |
| Organization | Country/region | Testosterone threshold for participation | Interval for required testing |
| World Aquatics [ | International | 2.5 nmol/L | In androgen-sensitive athletes, male puberty must be suppressed beginning at Tanner stage 2 or by age 12, whichever is later, AND have continuously maintained testosterone below 2.5 nmol/L. |
| World Rowing [ | International | 2.5 nmol/L | At least 24 months prior to the athlete’s first competition. |
| Union Cycliste Internationale (UCI) Cycling [ | International | 2.5 nmol/L | In androgen-sensitive athletes, male puberty must be suppressed beginning at Tanner stage 2 or by age 12, whichever is later, AND have continuously maintained testosterone below 2.5 nmol/L. |
| International Tennis Federation (ITF) [ | International | 5 nmol/L | At least 12 months prior to the athlete’s first competition. |
| USA Wrestling [ | United States | 10 nmol/L | At least 12 months prior to the athlete’s first competition. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLGBTQ Health, Identity, and Policy · Sexuality, Behavior, and Technology · Sexual Differentiation and Disorders
Introduction
The participation of transgender women in women’s sports is a topic rife with controversy [1,2]. The International Olympic Committee (IOC) published guidelines in 2015 stating that testosterone values among transgender women must be <10 nmol/L for at least 12 months prior to an athlete’s first competition [3]. In 2021, the IOC’s stance changed to deferring to each sport’s national governing body to set guidelines for participating in their sport [4]. Without a unifying set of guidelines, organizations have established their policies for participation [5]. Many have utilized objective measures, such as serum testosterone values, to guide eligibility criteria for transgender women in women’s sports. Testosterone levels vary widely between individuals, ranging from less than 2.5 nmol/L to less than 10 nmol/L, during a pre-competition period of 12-24 months [6-10].
Little is known regarding how quickly testosterone is suppressed below the threshold required for participation in women’s sport after initiation of gender-affirming hormone therapy (GAHT). Additionally, data is lacking that shows the degree to which specific regimens of GAHT achieve the defined testosterone thresholds in sport. This study aimed to elucidate trends in testosterone levels among transgender women on GAHT.
Materials and methods
Participants and procedures
Our retrospective cohort study examined clinical data from transgender women 18 and older who were seen at one academic medical system between January 2013 and April 2023. The Institutional Review Board of the University of Utah approved the study (approval number: 00161271, approval date: December 20, 2022). Waiver of consent and authorization was approved for this study. For this study, transgender women were defined as those who had at least one clinical encounter that billed specific International Classification of Diseases (ICD)-9 or ICD-10 diagnosis codes associated with gender dysphoria/transgender status (Table 1) [11,12] and documented prescriptions of estradiol and spironolactone for GAHT. Participation in sport was not an inclusion criterion of this study, as this information was not available to the authors. Protocols for initiating and titrating GAHT medications, as well as laboratory monitoring, at this institution (Tables 2-3) mirror the current standards of care recommended by the Endocrine Society and the World Professional Association for Transgender Health [13,14]. An index date was defined for each patient as the date at which the first prescription for GAHT was provided. Further details of the dataset creation were previously published by Ho et al. [15]. Serum testosterone values, previously drawn as part of routine GAHT monitoring, were analyzed.
Statistical analyses
Mean and median testosterone values at 12 and 24 months after initial prescription for GAHT and proportions of testosterone values over 5 nmol/L and 2.5 nmol/L were calculated. These time points and serum values were chosen because they are commonly used to guide eligibility criteria for participation in sport [6-10]. A 95% confidence interval was also computed for the means, medians (calculated using bootstrapping with 1,000 replications) [16-18], and proportions (calculated based on Wilson confidence intervals) [19] above.
Results
A total of 261 patients met study criteria at 12 months. The mean age among this group was 28 years. After 12 months on GAHT, patients demonstrated a median testosterone of 0.52 nmol/L (95% CI: 0.47-0.73) and a mean testosterone of 3.39 nmol/L (95% CI: 2.63-4.15) (Figure 1). After 24 months, 112 patients met study criteria. The mean age of this group was 30 years. The median testosterone level among this group was 0.43 (95% CI: 0.35-0.66), and the mean was 3.90 nmol/L (95% CI: 2.51-5.29). As shown in Figure 1, at 12 months, 19.5% (95% CI: 15.2-24.8) of patients had testosterone values higher than the 5 nmol/L threshold, and 23.8% (95% CI: 19.0-29.3) had values above the 2.5 nmol/L threshold. At 24 months, 22.3% (95% CI: 15.6-30.9) and 25.0% (95% CI: 17.9-33.8) were above the respective thresholds.
Histogram of testosterone levels (nmol/L) for all subjects at 12 monthsThe x-axis lists the ranges of each testosterone level for each bin. The left y-axis refers to the bar graph and indicates the number of subjects in each bin. The right y-axis refers to the line graph, representing the percentage of subjects with a testosterone level at or higher than that bin. For example, 23.8% of subjects have a testosterone level of 2.5 nmol/L or higher.
Discussion
Many organizations have testosterone-based policies informing the participation of transgender women in women’s sports. Policies vary in testosterone threshold and length of documented testosterone suppression prior to participation. Testosterone levels of less than 10, 5, or 2.5 nmol/L are required by many organizations for varying periods prior to participation (Table 4) [6-10]. However, there is a paucity of data supporting the use of these specific thresholds. Moreover, recent publications suggest that testosterone suppression post-puberty does not negate the male performance advantage; persistent biomechanical advantages are seen in transgender women, namely muscle mass and explosive strength [1,20,21].
Many studies exist that review testosterone values among cisgender women. One meta-analysis aggregating nine studies demonstrated a 95% confidence interval for testosterone of 0-1.7 nmol/L [22]. The same meta-analysis showed that among women with polycystic ovary syndrome, a common condition associated with increased circulating testosterone levels, the mean testosterone level was 1.69 nmol/L, with an upper limit of 3.13 nmol/L (95% CI, one-sided) or 4.77 nmol/L (99.99% CI, one-sided) [22].
Current Endocrine Society guidelines define the goal testosterone for transgender women as <1.73 nmol/L [14]. Nonetheless, published data on testosterone levels among transgender women vary. One previous study of 40 participants reported mean testosterone levels of 0.52 nmol/L and 0.59 nmol/L after 12 and 24 months of GAHT, respectively. Another study of 275 participants reported mean levels of 0.40 nmol/L after both 12 months and two to four years on GAHT [23,24]. Notably, participation in sports was not a criterion for eligibility in either study.
Our study found that transgender women had a mean testosterone of 3.39 nmol/L after 12 months of GAHT and 3.90 nmol/L after 24 months on GAHT. These values are significantly higher than the median values of 0.52 nmol/L and 0.43 nmol/L at 12 and 24 months on GAHT, respectively. The positively skewed data in our study shows that while many patients achieve significant suppression of testosterone values on standard doses of GAHT, this regimen may not be adequate for all patients. Additionally, this retrospective data likely describes testosterone levels of transgender women with typical use of GAHT versus perfect use in those mentioned above, highly standardized, prospective studies.
Collectively, these data show wide variability in testosterone levels among transgender women on the current standard of care regimens of GAHT. This may be related to variability in patient compliance with treatment regimens, patient population, or laboratory testing.
Limitations
Our study has several limitations. The authors acknowledge that many individuals taking estradiol-based GAHT do not identify as transgender women. For this study, transgender women were defined as those who met the combined criteria of an ICD-9 or ICD-10 diagnosis associated with gender dysphoria/transgender status and prescriptions for GAHT. Although these patients had documented prescriptions for estradiol and spironolactone, it is possible that these medications were not taken as prescribed. Nonadherence to GAHT may affect testosterone values obtained at the 12- and 24-month time points. This may highlight the typical use versus the ideal use of hormones in prior studies. Patients were not excluded if they had received previous gender-affirming surgeries. Our final cohort of 112 patients at 24 months was significantly smaller than the initial cohort of 261 patients at 12 months, as many were likely lost to follow-up or had transitioned their care to another institution. Finally, participation in sport was not an inclusion criterion of this study, as this data was unavailable to the authors.
Conclusions
While many organizations have included testosterone thresholds in their guidelines for participation of transgender women in women’s sports, limited studies exist describing typical trends in testosterone among transgender women on GAHT. In our sample, almost one quarter of patients did not achieve testosterone suppression below the thresholds of 2.5 and 5 nmol/L proposed by many organizations after one and two years on the current standard of care GAHT guidelines. These data may be used to inform the typical history of testosterone levels on the current standard of care GAHT therapy for future athlete-specific studies to reference. Further understanding of both the degree of testosterone suppression on different regimens of GAHT and the duration of GAHT required to meet guidelines for participation in women’s sport is needed to inform guidelines for participation of transgender women in women’s sport.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Transgender women in the female category of sport: perspectives on testosterone suppression and performance advantage Sports Med Hilton EN Lundberg TR 1992145120213328990610.1007/s 40279-020-01389-3PMC 7846503 · doi ↗ · pubmed ↗
- 2Gender, testosterone, and sport Clin J Sport Med Rizzone KH 77783220223294138010.1097/JSM.0000000000000849 · doi ↗ · pubmed ↗
- 3IOC consensus meeting on sex reassignment and hyperandrogenism November 2015 L., Jose, M., Patino, M., Ritzén, M., Vilain, E., Partner, J. T., Bird, B. &, Riley, L., & Thill, C 4 2025 Harper Harper J.J. Hirschberg Hirschberg AA 20152015 https://stillmed.olympic.org/Documents/Commissions_PD Ffiles/Medical_commission/2015-11_ioc_consensus_meeting_on_sex_reassignment_and_hyperandrogenism-en.pdf
- 4IOC framework on fairness, inclusion and non-discrimination on the basis of gender identity and sex variations 4 2025 2021 https://stillmed.olympics.com/media/Documents/Beyond-the-Games/Human-Rights/IOC-Framework-Fairness-Inclusion-Non-discrimination-2021.pdf 10.1136/bjsports-2022-10638636526281 · doi ↗ · pubmed ↗
- 5Policies by organization 4 2025 Mosier Mosier C.(2024 2024 https://www.transathlete.com/policies-by-organization
- 6Policy on eligibility for the men’s and women’s competition categories 4 2025 FINA.(2023 2023 https://resources.fina.org/fina/document/2023/03/27/dbc 3381 c-91e 9-4ea 4-a 743-84c 8b 06debef/Policy-on-Eligibility-for-the-Men-s-and-Women-s-Competiition-Categrories-Version-on-2023.03.24.pdf
- 7ITF transgender policy 4 2025 International Tennis Federation.(2023 August 10 2023 https://www.itftennis.com/media/2163/itf-transgender-policy.pdf
- 8Transgender athlete participation policy 4 2025 2025 https://s 3.amazonaws.com/usac-craft-uploads-production/documents/USA-Cycling-Policy-VII-Transgender-Athlete-Participation.pdf