Prevalence, Antimicrobial Susceptibility Pattern and Associated Factors of Staphylococcus Aureus Among Camel's Raw Milk in Babile District, Oromia, Ethiopia
Ahmednur Abdi, Siraj Hussen, Mohammed Ahmed

TL;DR
This study found that 14% of raw camel milk in Ethiopia was contaminated with Staphylococcus aureus, a bacteria that can cause illness and is often resistant to antibiotics.
Contribution
The study identifies risk factors and high antibiotic resistance in Staphylococcus aureus from raw camel milk in Ethiopia.
Findings
14% of raw camel milk samples were contaminated with Staphylococcus aureus.
High resistance to tetracycline, penicillin G, and amoxicillin was observed in the bacteria.
Factors like poor hygiene and container type increased contamination risk.
Abstract
Staphylococcus aureus (S. aureus) is a versatile pathogen that causes diseases. Raw milk is an ideal, rich medium that helps and supports the growth of microorganisms and is highly susceptible to S. aureus immediately after milking. As camel milk was usually consumed in its raw state in pastoralist areas, the contamination and intoxication of raw milk due to pathogenic S. aureus were a public health problem. The study aimed to determine the prevalence, antibiotic resistance pattern, and associated factors of S. aureus in raw camel milk in Babile District, Oromia Region, Eastern Ethiopia. A community‐based cross‐sectional study was conducted in the Babille district among 350 raw camel milk. Participants were selected using a multi‐stage sampling technique. Data was collected using a pretested structured questionnaire, and 25 mL of raw camel milk was collected in sterile screw‐capped…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
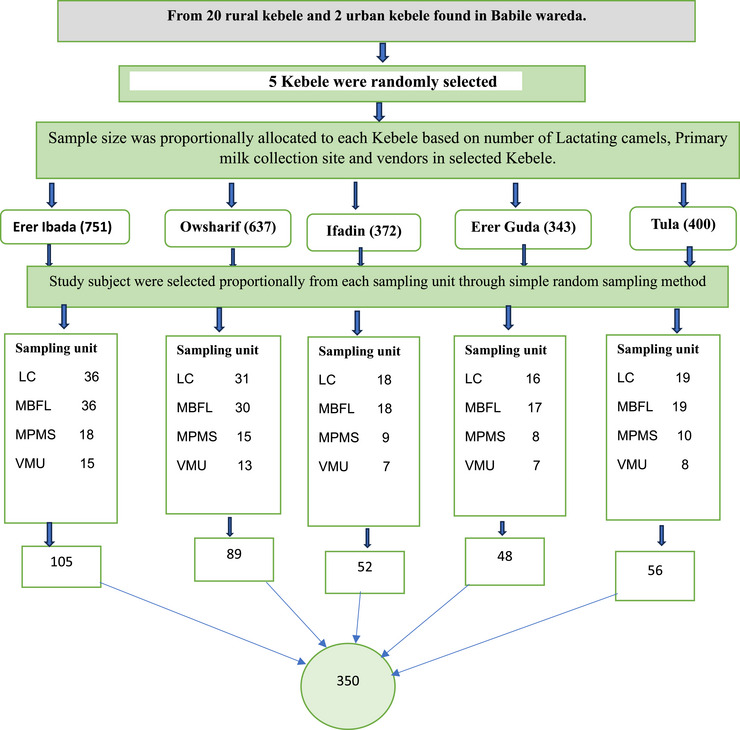 FIGURE 1
FIGURE 1| Variables | Category | Number | Percent (%) |
|---|---|---|---|
| Age | 18–20 | 17 | 4.9% |
| 21–30 | 81 | 23.1% | |
| 31–40 | 163 | 46.6% | |
| 41–50 | 89 | 25.4% | |
| Sex | Male | 110 | 31.4% |
| Female | 240 | 68.6% | |
| Residence | Urban | 27 | 7.7% |
| Rural | 323 | 92.3% | |
| Level of education | No formal education | 272 | 77.7% |
| Primary | 49 | 14% | |
| Secondary | 26 | 7.4% | |
| College and above | 3 | 0.9% |
| Variables | Category | Number | Percent% |
|---|---|---|---|
| Body condition scour of lactating camels | Good | 116 | 48.3% |
| Modern | 79 | 32.9% | |
| Poor | 45 | 18.8% | |
| Number of dairy camels (herd size) | Small (< 5) | 148 | 61.7% |
| Medium (5–10) | 72 | 30% | |
| Large (> 10) | 20 | 8.3% | |
|
Number of birth lactating camels gave (Parity). | Few (1–2 calves) | 101 | 42.1% |
| Moderate (3–4 calves) | 86 | 35.8% | |
| Many (> 4 calves) | 53 | 22.1% | |
| Stage of lactation in month | Early (1–2) | 85 | 35.4% |
| Medium (3–9) | 79 | 32.9% | |
| Late (10–18) | 76 | 31.7% | |
| Age of lactating camels | Young (≥ 5–7) | 91 | 37% |
| Adult (> 8 ‐≥ 11) | 105 | 43.8% | |
| Old (> 11) | 44 | 18.3% | |
| Drainage condition | Good | 159 | 66.3% |
| Poor | 81 | 33.7% | |
| Type of utensils used | Plastic containers | 170 | 70.8% |
| Stainless steel containers | 11 | 4.6% | |
| Traditional container | 59 | 24.6% | |
| Cleaning of utensils before milking | Yes | 231 | 96.3% |
| No | 9 | 3.7% | |
| Cleaning condition | Cold water and Scrub with sand | 188 | 78.3% |
| Soap and cold water | 22 | 9.2% | |
| Soap and hot water | 30 | 12.5% | |
| Smoking of milking equipment | Yes | 235 | 97.9% |
| No | 5 | 2.1% | |
| Hand washing before milking | Yes | 202 | 84.2% |
| No | 38 | 15.8% | |
| Ways to wash hands before milking | With cold water | 155 | 75.2% |
| Soap and cold water | 28 | 13.6% | |
| Soap and hot water | 23 | 11.2% | |
| Udder washing before milking | Yes | 14 | 5.8% |
| No | 226 | 94.2 | |
| Udder or teats dried after washing | Yes | 11 | 78.6% |
| No | 3 | 21.4% | |
| Use of separate towels | Yes | 3 | 6.3% |
| No | 11 | 93.7% | |
| Antiseptic use during milking | Yes | 15 | 21.4% |
| No | 225 | 78.6% | |
| Hair of milkers | Covered | 213 | 88.7% |
| Not covered | 27 | 11.3% | |
| Milk filtering | Yes | 27 | 11.2% |
| No | 213 | 88.8% |
| Variables | Category | Number | Percent (%) |
|---|---|---|---|
| Types of containers used to collect milk | Wide necked‐plastic vessels | 20 | 33.3% |
| Narrow necked plastic vessels | 30 | 50% | |
| Traditional container | 10 | 16.7% | |
| Chilling/cooling machine | Yes | 0 | 0 |
| No | 60 | 100% | |
| Length of time milk stayed before transportation | < 2 h | 13 | 21.7% |
| 2 –6 h | 25 | 41.6% | |
| 6 –12 h | 22 | 36.7% | |
| Transportation of milk to the market | Using car | 23 | 38.3% |
| Using donkey | 28 | 46.7% | |
| Motorcycle | 9 | 15% | |
| Main source of water used for cleaning | Tap water | 280 | 80% |
| River | 70 | 20% | |
| Habit of milk consumption | Raw milk | 274 | 78.3% |
| Boiled milk | 76 | 21.7% | |
| Knowing any GIT disturbance | Yes | 134 | 38.3% |
| No | 216 | 61.7% |
| Variables | Category | Number | Percent (%) |
|---|---|---|---|
| Type of milk selling | Raw milk | 19 | 38% |
| Boiled milk | 23 | 46% | |
| Both raw and boiled milk | 8 | 16% | |
|
Type of containers used for selling milk | Wide‐necked aluminium vessels | 19 | 38% |
| Wide‐necked plastic vessels | 11 | 22% | |
| Narrow necked plastic containers | 13 | 26% | |
| Used plastic water bottles | 7 | 14% | |
|
Routine cleaning of the milk containers. | Cleaning before putting in milk | 19 | 38% |
| Cleaning after delivery of milk | 6 | 12% | |
| Before putting in milk and after delivery of milk | 25 | 50% | |
| Milk storage | In plastic containers | 31 | 62% |
| In traditional containers | 3 | 6% | |
| In stainless steel containers | 16 | 32% | |
| Cooling of milk | Yes | 19 | 38% |
| No | 31 | 62% |
| Prevalence of | Bivariate analysis | Multivariable analysis | |||||
|---|---|---|---|---|---|---|---|
| Variables | Category | Growth n (%) | No Growth n (%) | COR (95% CI) |
| AOR (95% CI) |
|
| Educational status |
No formal Education No formal education | 44 (16.2) | 228 (83.8) | 2.61 (0.598, 11.355) |
| 1.33 (0.026, 4.315) | 0.400 |
| Primary | 3 (6.1) | 46 (93.9) |
1.88 (0.138, 5.606) | 0.893 | 1.19 (0.050, 12.574) | 0.869 | |
| Secondary and college | 2 (6.89) | 27 (93.103) | 1 | 1 | |||
| Body condition scour | Good | 9 (7.8) | 107 (92.2) | 1 | 1 | ||
| Medium | 7 (8.9) | 72 (91.1) | 1.16 (0.412, 3.244) | 0.783 | 0.65 (0.194, 2.138) | 0.473 | |
| Poor | 12 (26.7) | 33 (73.3) | 4.32 (1.675, 11.160) |
| 1.72 (0.527, 5.615) | 0.369 | |
| Number of dairy camels (herd size) | Small (< 5) | 15 (10.1) | 133(89.9) | 1 | 1 | ||
| Medium (5–10) | 9 (12.5) | 63 (87.5) | 1.27 (0.526, 3.051) | 0.598 | 1.02 (0.342, 3.061) | 0.966 | |
| Large (>10) | 4 (20) | 16 (80) | 2.21 (0.655, 7.499) |
| 1.77 (0.137, 4.363) | 0.772 | |
| Number of birth lactating camels give (parity) | Few (1–2) | 7 (6.9) | 94 (93.1) | 1 | 1 | ||
| Moderate (3–4) | 8 (9.3) | 78 (90.7) | 1.38 (0.478, 3.967) | 0.533 | 1.11 (0.360, 3.433) | 0.854 | |
| Many (> 4) | 13 (24.5) | 40 (75.15 | 4.36 (1.621, 11.752) |
| 3.52 (1.207, 10.277) |
| |
| Age of lactating camels | Young (≥ 5 ≥ 7) | 5 (5.5) | 86 (94.5) | 1 | 1 | ||
| Adult (≥ 8 ‐≥ 11) | 11 (10.5) | 94 (89.5) | 2.01 (0.672, 6.028) |
| 3.97 (0.896, 17.622) | 0.069 | |
| Old (> 11) | 12 (27.3) | 32 (72.7) | 6.45 (2.106, 19.757) |
| 3.19 (0.760, 13.419) | 0.113 | |
| Drainage condition of milking place | Good | 9 (5.7) | 150(94.3) | 1 | 1 | ||
| Poor | 19(23.5) | 62 (76.5) | 5.11 (2.191, 11.908) |
| 4.63 (1.853, 11.557) |
| |
| How to clean milking utensils | Cold water and Scrub with sand | 25 (13.3) | 163 (86.7) | 4.45 (0.580, 34.119) |
| 4.43 (0.314, 62.457) | 0.136 |
| Soap and cold water | 2 (9.1) | 20 (90.9) | 2.90 (0.246, 34.187) | 0.398 | 5.31 (0.527, 47.784) | 0.136 | |
| Soap and hot water | 1 (3.3) | 29 (96.7) | 1 | 1 | |||
| Washing hand before milking | Yes | 15 (7.4) | 187(92.6) | 1 | 1 | ||
| No | 13 (34.2) | 25 (65.8) | 6.48 (2.765, 15.197) |
| 3.94 (1.599, 9.716) |
| |
| Hair of milker. | Covered | 19 (8.9) | 194 (91.1) | 1 | 1 | ||
| Not covered | 9 (33.3) | 18 (66.7) | 5.11 (2.017, 12.921) |
| 1.87 (0.511, 6.879) | 0.344 | |
| Type of milk selling | Boiled milk | 2 (8.7) | 21 (91.3) | 1 | 1 | ||
| Raw milk | 6 (31.6) | 13 (68.4) | 4.85 (0.848, 27.704) |
| 7.21 (0.956, 54.389) | 0.055 | |
| Both Raw and boiled milk | 2 (25) | 6 (75) | 3.50 (0.404, 30.342) | 0.256 | 4. 95 (0.399, 61.438) | 0.213 | |
| Type of containers used for selling milk. | Wide‐necked aluminium vessels | 2 (9.5) | 19 (90.5) | 1 | 1 | ||
| Wide‐necked plastic vessels | 1 (12.5) | 7 (87.5) | 1.36 (0.106, 17.417) | 0.815 | 1.70 (0.056, 8.8222) | 0.783 | |
| Narrow necked plastic containers | 1 (14.3) | 6 (85.7) | 1.58 (0.121, 20.686) | 0.726 | 1.64 (0.051, 7.965) | 0.726 | |
| Used plastic water bottles | 6 (42.9) | 8 (57.1) | 7.13 (1.177, 23.144) |
| 8.40 (1.258, 26.068) |
| |
| Routine cleaning of milk containers. | Cleaning before putting in milk | 6 (31.6) | 13 (68.4) | 3.69 (0.790, 17.249) |
| 4.40 (0.581, 33.335) | 0.151p |
| Cleaning after delivery of milk | 1 (25) | 3 (75) | 2.67 (0.206, 24.555) | 0.453 | 2.04 (0.88, 37.422) | 0.658 | |
| Before putting in milk and after delivery of milk | 3 (11.1) | 24 (88.9) | 1 | 1 | |||
| Cooling of milk | Yes | 2 (10.5) | 17 (89.5) | 1 | 1 | ||
| No | 8 (25.8) | 23 (74.2) | 2.96 (0.556, 15.729) |
| 1.7 (0.84, 11.119) | 0.980 | |
| Type of containers used to collect milk | Wide necked‐plastic vessels | 2 (10) | 18 (90) | 1 | 1 | ||
| Narrow necked plastic vessels | 7 (23.3) | 23 (76.7) | 2.74 (0.506, 14.818) |
| 1.24 (0.017, 3.407) | 0.292 | |
| Traditional container | 2 (20) | 8 (80) | 2.25 (0.267, 18.925) | 0.455 | 1.61 (0.059, 6.185) | 0.672 | |
| Main source of water | Tap water | 31 (11.1) | 249 (88.9) | 1 | 1 | ||
| River | 18 (25.7) | 52 (74.3) | 2.79 (1.447, 5.343) |
| 1.95 (0.705, 5.363) | 0.199 | |
| Habit of milk consumption | Boiled milk | 5 (6.6) | 71 (93.4) | 1 | 1 | ||
| Raw milk | 44 (16.1) | 230 (83.9) | 2.72 (1.038, 7.112) |
| 1.38 (0.190‐1.633) | 0.195 | |
| Knowing any GIT disturbance | Yes | 11 (8.2) | 123 (91.8) | 1 | 1 | ||
| No | 38 (17.6) | 178 (82.4) | 2.39 (1.174, 4.852) |
| 2.12 (0.563, 7.992) | 0.267 | |
|
Anti‐microbial disk | Susceptibility patterns of | |||||
|---|---|---|---|---|---|---|
| S | I | R | ||||
| No | % | No | % | No | % | |
| Gentamicin | 33 | 67.3 | 2 | 4.1 | 14 | 28.6 |
| Erythromycin | 46 | 93.9 | 0 | 0 | 3 | 6.1 |
| Ciprofloxacin | 42 | 85.7 | 2 | 4.1 | 5 | 10.2 |
| Penicillin G | 9 | 18.4 | 0 | 0 | 40 | 81.6 |
| Amoxicillin | 13 | 26.5 | 2 | 4.1 | 34 | 69.4 |
| Tetracycline | 7 | 14.3 | 2 | 4.1 | 40 | 81.6 |
| Cefoxitin | 47 | 95.9 | 0 | 0 | 2 | 4.1 |
| Oxacillin | 47 | 95.9 | 0 | 0 | 2 | 4.1 |
| Chloramphenicol | 38 | 77.6 | 4 | 8.2 | 7 | 14.3 |
| Trimethoprim‐sulfamethoxazole | 14 | 28.6 | 7 | 14.3 | 28 | 57.1 |
| Resistant to drug combination | Antimicrobial phenotypes | Number of isolates | |
|---|---|---|---|
| Number | Percent (%) | ||
| One antibiotic | AML | 2 | 4.08 |
| TET | 3 | 6.122 | |
| Two antibiotics | PEN, TET | 5 | 10.20 |
| TET, AML | 2 | 4.08 | |
| PEN, AML | 1 | 2.04 | |
| PEN, STX | 2 | 2.08 | |
| Three antibiotics | PEN, AML, STX | 1 | 2.04 |
| TET, AMP, STX | 1 | 2.04 | |
| PEN, TET, AML | 4 | 8.16 | |
| Four antibiotics | PEN, TET, AML, STX | 6 | 12.24 |
| PEN, GEN, TET, STX | 2 | 4.08 | |
| PEN, TET, CHL, STX | 1 | 2.04 | |
| Five antibiotics | PEN, GEN, TET, AML, STX | 7 | 14.28 |
| CHL, PEN, TET, AML, STX | 2 | 4.08 | |
| CIP, PEN, GEN, TET, AML | 1 | 2.04 | |
| CHL, CIP, PEN, TET, AML | 1 | 2.04 | |
| Six antibiotics | CHL, PEN, GEN, TET, AML, STX | 2 | 4.08 |
| ERY, CIP, PEN, GEN, AML, STX | 1 | 2.04 | |
| ERY, CIP, PEN, TET, AML, STX | 1 | 2.04 | |
| Eight antibiotics | CHL, CIP, PEN, TET, AML, CFO, OX, STX | 1 | 2.08 |
| ERY, PEN, GEN, TET, AML, CFO, OX, STX | 1 | 2.08 | |
| None | Resistance to none (susceptible to all antibiotics) | 2 | 4.08 |
| Total | 49 | 100 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnimal Diversity and Health Studies · Probiotics and Fermented Foods · Yersinia bacterium, plague, ectoparasites research
Introduction
1
Food‐borne diseases are a serious public health threat, which leads to significant losses in productivity and high medical costs (Garcia et al. 2020). Raw milk and raw milk products concerning staphylococcal poisoning were of great concern around the world (Sema et al. 2019). According to the World Health Organization (WHO), bacteria were incriminated in two‐thirds of dairy food borne outbreaks, registered globally (Enquebaher 2016). Staphylococcal food poisoning (SFP) was estimated to cause 420,000 deaths every year and generate health costs and economic losses in the range of 110 billion dollars worldwide (Danai et al. 2020). Camel milk is a vital source of food, nutrition security, and household income, as well as a significant cultural value for pastoral populations in Eastern African countries including Somalia, Sudan, Ethiopia and Kenya (Guliye et al. 2007).
Milk, being an essential source of food in the human diet, is an important carrier of both helpful and harmful microbes. Several pathogens, including Brucella spp., Campylobacter spp., Shiga toxin‐producing Escherichia coli, Listeria monocytogenes, Mycobacterium spp., Salmonella spp., and bacterial toxins, have been causally associated with milk‐borne illnesses (Dhanashekar et al. 2012). Among these bacteria, Staphylococcus aureus (S. aureus) is most commonly responsible for SFP outbreaks, and the ingestion of less than 1.0 µg enterotoxin causes SFP (Abdurabbah et al. 2018). Furthermore, zoonotic bacteria have developed significant antibiotic resistance. Antibiotics are utilised extensively in food animal production in underdeveloped nations to improve animal health and growth, even if their use in camels is not that much studied (Woldearegay et al. 2015, Gemeda et al. 2020). This approach may give some economic benefits to producers and consumers in general. Nonetheless, a major risk in this practice is related to continually exposing these animals to modest dosages of antibiotics that contribute considerably to antimicrobial resistance (Van et al. 2020).
S. aureus is a ubiquitous pathogen that causes invasive and life‐threatening infections, ranging in severity from slight skin infections to more severe diseases such as pneumonia, endocarditis, and septicaemia (Yakubu et al. 2020, Teshome et al. 2016). S. aureus is a Gram‐positive, catalase‐positive, facultative anaerobic, and usually oxidase‐negative bacterium which belongs to the family of Micrococcaceae and the genus Staphylococcus (Aqib et al. 2018). The natural ecological niches of S. aureus are the nasal cavity and the skin of warm‐blooded animals. The mucous membranes, skin, udders, and teats of milking animals are the most important reservoirs of this contaminant (Teshome et al. 2016).
Methicillin‐resistant S. aureus (MRSA) and biofilm‐producing S. aureus are emerging common strains of S. aureus being isolated from dairy products (Aqib et al. 2019). It produces a variety of toxins and invasive enzymes such as haemolysins, staphylococcal enterotoxins (SE), toxic shock syndrome toxin‐1 (TSST‐1), leukocidin, plasma coagulase and deoxyribonuclease (Jingsha et al. 2019). There are several types of staphylococcal enterotoxins (SE), and SE is responsible for dairy food poisoning, and to date, more than 21 different SEs and SE‐like super‐antigens have been identified (Betelihem and Shimels 2017). Among various factors associated with this pathogen are unhygienic milking procedures, poor handling practices of milk, improper preventive techniques, lack of germicidal teat dipping, and improper storage and transport of milk (Ayoub et al. 2020). In addition, dairy animals suffer from S. aureus‐induced mastitis is also the other source of milk contamination (Remaz et al. 2017). Furthermore, in camels, anatomically, the anus is positioned above the udders, making faecal contamination during milking a common occurrence, even in the most hygienic operations (Dairy safe, 2019).
S. aureus has been associated with many diseases of humans and animals, and the pathogenicity of this bacterium is mostly due to a combination of genetic factors mediating invasiveness, virulence, ability to produce different enzymes, antibiotic resistance, ability to evade the immune system of the host, and possessing mechanisms that damage the host's tissue and facilitate colonisation (Emmanuella et al. 2019, Arumugam et al. 2017, Edalati et al. 2019). Raw milk is an ideal rich medium that supports the growth of microorganisms and is an important source of staphylococcal food poisoning that causes gastroenteritis (Jingsha et al. 2019). Milk is highly susceptible to S. aureus immediately after milking when it is almost at body temperature (Tawfik et al. 2019).
There are many ways by which the pathogen can enter into dairy food destined for human consumption, especially in the raw state (Ana et al. 2020). Most commonly, microbial contamination of milk can occur from three main sources: from within the udder, from the exterior of the udder, and from the surface of milk handling and storage equipment (Ewa et al. 2016). Approximately 20–30% of human populations are consistent carriers of this bacterium, while 60% are the transient carriers of S. aureus. Therefore, insufficient pasteurisation during preparation, processing, and distribution by the carriers of S. aureus is the common factor for the outbreaks of staphylococcal dairy food poisoning (Fakhri et al. 2019).
In developing countries like Ethiopia, there is high consumption of raw milk with poor hygienic practices (Carruth et al. 2017). Also, misuse of antibiotics was common, which may result in the development of multi‐drug resistant (MDR) S. aureus isolates, and S. aureus milk intoxication was one of the leading public health problems in this regard (Yenealem 2020). In Ethiopia, the data regarding the prevalence of S. aureus in raw camel milk was scarce. Some authors have reported the prevalence of S. aureus in a limited area of the country, with varied prevalences ranging from 4.2% (n = 174) at Jigjiga town (Husein et al. 2013) to 88% (n = 35) at Dubti town in the Afar region (Wasie et al. 2015), which needs national surveillance to get the general epidemiology of S. aureus in raw camel milk. Generally, there are few studies on the prevalence, associated factors, and antimicrobial susceptibility of S. aureus in raw camel milk in Ethiopia, and more extensive investigations may provide more information. Continuous monitoring of the prevalence and profile of antimicrobial susceptibility could help to control infections more effectively while reducing the emergence of antibiotic‐resistant microbes.
Therefore, this study was aimed at determining the prevalence, antimicrobial susceptibility pattern, and associated factors of S. aureus in raw camel milk in the Babille district Oromia region of Eastern Ethiopia.
Methods and Materials
2
Study Setting, Design and Period
2.1
The study was conducted at Babile District, which is located in the East Hararghe zone, Oromia region, Eastern Ethiopia, from May 2021 to July 2021. Babile District (BD) is one of the districts in the East Hararghe zone located in the eastern corner of Oromia Regional State, bordered by Fedis, Gursum, Harari and Somali National Regional State. The district has a total area of 3169.06 km^2^ and an estimated total population of 94,650 people, of whom 56,198 are male and 48,452 are female (CSA 2014). Babille district has 20 rural kebeles and two urban administrations. Babile district has a huge potential in dairy production and livestock husbandry, which was dominated by 56,355 cattle, 122,160 sheep, 23,020 goats and 10,317 camels (Amentie et al. 2016, District 2018). According to evidence obtained from the Babille district, average milk production per year was about 3,470,776 litres, and about 75% was used for the market as income generation in the district (BDLDHA 2018). A community‐based cross‐sectional study was conducted among raw camel milk in the Babille district. The unavailability of raw milk during sample collection was excluded from the study.
Sample Size and Sampling Technique
2.2
The sample size (n = 350) was calculated using a single population proportion formula with the following assumptions: confidence level of 95%, margin of error of 5%, prevalence of S. aureus in raw camel's milk in Jigjiga 11.45% (Serda et al. 2018), design effect 2 and 10% non‐respondent rate.
Multi‐stage sampling techniques were used to select kebeles, dairy householders, primary milk collectors, vendors, and milk utensils. From 20 rural kebele and 2 urban administrative, of which 5 kebele were selected using the lottery method. Accordingly, 350 respondents and subsequent 350 camels’ raw milk samples owned by these respondents were aseptically collected from the udder, milking bucket at farm level, milk container from primary milk collectors, and vendor's milk container using simple random sampling. After proportional allocation was made to take an appropriate sample from woredas, we took 105 from Erer ibada, 89 from Owsharif, 52 from Ifadin, 48 from Erer guda and 56 from Tula kabale according to the following diagram (Figure 1).
Diagram showing sampling technique from Babille district, Oromia Region Eastern Ethiopia, 2021. LC, lactating camel; MPMS, milking bucket at farm level; MPMS, Milk utensil at primary milk collection site; VMU, vendors milk utensil.
Data Collection Methods
2.3
Data collectors were trained and informed to collect data by using the structured questionnaire. After informed, voluntary, written, and signed consent was obtained, socio‐demographic characteristics and information related to milk handling practices such as awareness of milk contamination, transportation condition, storage condition, drainage condition of milking environment, body condition scour of lactating camels, washing of milking equipment and milk storage, hand washing before milking, type of the milking equipment, type of water used, filtration of milk after milking, stage of lactation, parity of the camel, age of lactating camel and heard size was collected by trained medical laboratory profession through face‐to‐face interview using structured questionnaires. While administering questionnaires, direct observation of the cleanliness of body condition scour and drainage condition of the milking place was also noted.
Sample Collection Procedure and Laboratory Analysis
2.4
Twenty‐five (Ewa et al. 2016) mL of fresh milk samples were collected into sterile screw‐capped bottles by trained laboratory technologists. Samples from the udder were collected directly from the udder of randomly selected lactating camels on the farm. The surface of the teat end was cleaned by wiping it with clean cotton dipped in 70% alcohol before sampling, and the first jets of milk were discharged to reduce the contamination of the teat canal (Venugopal et al. 2019).
The bottles were labelled with permanent markers before sampling. All samples were placed in separate sterile plastic bags to prevent spillage and cross‐contamination, and sample‐containing bottles were transported in an icebox to the Microbiology laboratory, College of Health and Medical Sciences, Haramaya University within 2 h of collection. Upon arrival, the samples were cultured immediately or stored in a refrigerator at 4°C for a maximum of 24 h until inoculated onto a standard bacteriological media (Yenealem 2020).
The bacteriological medium was prepared according to the manufacturer's recommendations, and milk samples were subjected to bacterial culture and identification according to the procedures described by Quinn (Quinn et al. 2004). The presence of Staphylococcus was confirmed based on colony morphology, Gram's staining, catalase tests and DNase tests. Briefly, a loop full of milk samples was inoculated onto blood agar base enriched with 5% sheep blood (S2) and incubated aerobically at 37^∘^C for 24–48 hrs. Suspected colonies were sub‐cultured onto mannitol salt agar (S1) and incubated aerobically at 37°C for 24–48 hrs. The colonies of staphylococci that produced a yellow pigment on mannitol salt agar media were subjected to DNase tests. Finally, Staphylococcus aureus was identified as DNase positive (Quinn et al. 2004). After identification, all isolates of S. aureus were preserved at ‐20°C in 30% glycerol.
Antimicrobial Susceptibility Tests
2.5
Antibiotic susceptibility testing was done using the Kirby‐Bauer disc diffusion method on Mueller‐Hinton agar, according to the criteria set by the Clinical and Laboratory Standards Institute (CLSI 27^th^ edition) (Clinical and Laboratory Standards Institute (CLSI) 2017). The following antimicrobial discs were used: amoxicillin (25 µg), penicillin G (10 units), cefoxitin (30 µg), gentamicin (10 µg), ciprofloxacin (5 µg), trimethoprim‐sulfamethoxazole (25 µg), erythromycin (15 µg), chloramphenicol (30 µg), oxacillin (1 µg) and tetracycline (30 µg) (Teshome et al. 2016). These antibiotics were selected because of their local availability, and antibiotics of veterinary and human health relevance were also considered.
Fresh overnight cultures were prepared and used for antibiotic sensitivity tests. About 3–5 morphologically identical colonies of S. aureus from pure cultures were collected with an inoculating loop and transferred into a tube containing 5 mL of nutrient broth, and the suspension became adjusted to the density of 0.5 McFarland standards, which yielded a uniform suspension. After incubating the plates at 37°C for 18–24 h aerobically, diameters of the zone of bacterial growth inhibition around the discs were measured to the nearest millimetre, and the susceptibility or resistance to the agent in each disc was determined (S3). S. aureus susceptibility was classified as sensitive, intermediate, or resistant according to the standardised table of CLSI (2017) (Clinical and Laboratory Standards Institute (CLSI) 2017).
Data Management and Quality Control
2.6
The questionnaire was prepared in English, translated to Afan Oromo, and then translated back to English to check for consistency. Proper training was given to data collectors. Before starting the actual study, the questionnaire was pre‐tested in non‐selected kebele (Gamachu and Darera Arba kebele), and feedback was presented to the data collectors, and the questionnaire was amended accordingly. The principal investigator monitored the data collection process to ensure the completeness and reliability of the collected information throughout the data collection process.
For laboratory analysis, pre‐analytical, analytical, and post‐analytical stages of quality assurance were applied, and standard operating procedures (SOPs) of the microbiology laboratory were strictly followed. New batches of stain and reagent were checked for the correct staining reaction using a smear containing known Gram‐positive and Gram‐negative S. aureus as a control. Preparation and performance evaluation of culture media were improved by strictly following standard operating procedures and the manufacturer's instructions. All culture plates and antibiotic discs were stored at the recommended refrigeration temperature (2–8°C). Sterility of culture media was assessed by incubating 3–5% of a batch of prepared culture media at 35–37° for 24 h and checking for any growth. The reference strain of S. aureus ATCC 25923 was used for quality control of the antimicrobial susceptibility test. Quality control of culture media was checked by inoculating quarter plates of the medium with a control organism and incubating aerobically at 35–37°C for 24 h. The results of each control species and isolated S. aureus were recorded.
Data Processing and Analysis
2.7
Data was checked for completeness, cleaned, coded, and entered using EPI Data version 3.1 and exported to the statistical package for social scence (SPSS) version 25 for analysis. All variables were initially tested for association with S. aureus in raw camel milk by using the binary logistic regression. Then the variables, which showed p < 0.25 by binary logistic regression, were selected for multivariate analysis to check for possible associated factors of S. aureus by controlling potential confounding factors. An odds ratio with a 95% confidence interval (CI) was used to measure the strength of the association. In all cases, a P‐value <0.05 was considered to be statistically significant.
Results
3
Sociodemographic Characteristic of Respondents in Babile District
3.1
In this study, 350 respondents were enrolled with a 100% response rate. Of these, 120 were camel householders, 120 were milking personnel, 60 were primary milk collectors and 50 were vendors. The mean age of the respondents was 35.14 with (±SD) 7.99 years. Of the total respondents, 68.6% were females, 92.7% were rural residents and 77.7% of respondents had no formal education (Table 1).
Prevalence of S. aureus in Raw Camel Milk of Babile District
3.2
The overall prevalence of S. aureus isolated from raw camel milk in the study area was 14% (95% CI; 10–18). Out of the total sample size, 26.6% (13/49), 30.6% (15/49), 22.4% (11/49) and 20.4% (10/49) were isolated samples from the udder, milking container, primary milk collection centre, and vendor's milk container, respectively. The prevalence within the sources of sampling points varied from 10.8 % to 20 %: 10.8 %, 12.6%, 18.3% and 20 % were isolated from udder, milking container, primary milk collection centre and vendor's milk container, respectively. There was variation in the prevalence of S. aureus between kebeles.
Among the five‐selected kebeles, the higher prevalence of S. aureus was isolated from the Erer Gudda kebele at 20.8% (10/48), followed by Ifadin at 15.4% (8/52), while the lowest was isolated from the Owsharif kebele at 11.2% (10/89).
Factors Associated With Prevalence of S.aureus in Raw Camel Milk
3.3
Factors Related to Milk Handling Practice by Milking Personnel and Lactating Camels
3.3.1
In this study, 61.7% (148/240) of householders had kept a small number of dairy camels (herd size), and 42.1% were lactating camels that gave few births. A large proportion of milking personnel (70.8%) used plastic containers for milking; most of the milking personnel (94.2%) did not wash the udder before milking, and 93.7% did not use antiseptic during milking (Table 2).
Factors Related to Milk Collectors at the Primary Collection Centre, Main Source of Water and Awareness of Risks Associated With Raw Milk Consumption
3.4
The present study result showed that from 60 primary milk collection centres, 50% of primary milk collectors used narrow necked‐plastic vessels to collect milk at the primary milk collection centre, and a large proportion of primary milk collectors (41.6%) kept milk at the collection centre for 2–6 h before it was transported to the market. Of 350 respondents, 80% (280/350) used tap water as a main source of water. Moreover, 78.3% (274/350) and 38.3% (134/350) of respondents consumed raw milk and knew of GIT disturbances associated with drinking raw camel milk, respectively (Table 3).
Factors Related to Vendors' Milk Handling Practice
3.5
In this study, 38% (19/50) and 46% (23/50) of vendors sold raw milk and boiled milk respectively. Among 50 vendors, 38% (19/50) and 14% (7/50) used wide‐necked aluminium vessels and used plastic water bottles to sell the milk, respectively. In addition, 50% (25/50) of vendors cleaned their milk containers both before and after the delivery of milk, and 62% (31/50) stored the milk in plastic containers without a cold chain (Table 4).
Bivariate and Multivariable Analysis of Factors Associated With Prevalence of S. aureus in Camel's Raw Milk
3.6
In bivariate analysis, educational status, body condition scour, number of dairy camels, parity, age of lactating camel, drainage condition of the milking place, how to clean milking utensils, hand washing before milking, hair of milkers, type of milk selling, type of containers used for selling milk, cleaning of milk containers, cooling of milk, types of containers used to deliver milk to the collection centres, the main source of water, the habit of milk consumption, and knowing any GIT disturbance symptoms associated with consumption of raw milk were factors associated with the prevalence of S. aureus in a camel's raw milk in binary logistic regression.
However, in multi‐variable analysis, parity [AOR = 3.52, 95% CI: (1.207, 10.277)], drainage condition of milking place [AOR = 4.63, 95% CI: (1.853–11.557)], hand washing before milking [AOR = 3.94, 95% CI: (1.599, 9.716)] and type of containers used for selling milk [AOR = 8.40, 95% CI: (1.258, 26.068)] were significant predictors of the S. aureus in raw camel milk (Table 5).
Antibiotic Susceptibility Patterns of S. aureus
3.7
As illustrated in Table 6, antimicrobial susceptibility of S. aureus showed high susceptibility to cefoxitin (95.9%), oxacillin (95.9%), and erythromycin (93.9%), whereas a high level of resistance was recorded against tetracycline (81.6%), penicillin G (81.6%), and amoxicillin (69.4%) (Table 6).
The overall prevalence of MDR patterns (resistance to at least one antimicrobial drug in three or more antimicrobial categories) of S. aureus isolated from raw camel milk was 48.97 % (n = 24/49). Among 49 S. aureus isolated from camel's raw milk, five (10.2%) isolates were resistant to only one antibiotic, eleven (22.44%) isolates were resistant to five antibiotics, and two (4.08%) isolates were resistant to eight antibiotics. However, two (4.08%) isolates were susceptible to all subjected antibiotics (Table 7).
Discussion
4
Camel milk is a major food source in arid and sub‐arid environments, fulfilling a variety of qualitative and quantitative dietary requirements. Pastoralists in Ethiopia's eastern lowlands rely heavily on camels due to their outstanding ability to thrive in arid and semi‐arid settings with limited forage and water resources (Bekele and Molla 2001).
In the current study, the prevalence of S. aureus was 14% (95% CI: 10%–18%). The prevalence within the sources of sampling points varied from 10.8 %, 12.6%, 18.3% and 20% isolated from the udder, milking container, primary milk collection centre and vendor's milk container, respectively. This finding was in line with a study conducted in Ethiopia, in the Somali region 11.27% (Teshome et al., 2016); in the Jigjiga district, at 11.45% (Serda et al., 2018); in Iraq, in Al‐Qadisyia Province 13.4% (Abdulkadhim, 2012); and in Somalia, among Borana pastoralist 10.8% (Kebede et al., 2019). However, the present finding was higher than the study done in Eastern Libya (2.7%) (Abdurabbah et al. 2018); around Jigjiga town (4.2%) (Husein et al., 2013); and the study conducted in Iran (2.72%) (Rahi et al., 2020). In contrast, the present study was lower than the study done in Saudi Arabia, 20% (Aljahani et al., 2020); in Matrouh, Egypt, 46% (Ayoub et al., 2020); in Punjab, Pakistan, 88.5% (Aqib et al., 2017); in Southern Algeria, 35.61% (Saidi et al., 2021); in Algeria, 21% (Chaalal et al., 2016); in Kafr Elsheikh, Egypt, 22.6% (Tawfik et al., 2019); and in Dubti town, Afar region, 54% (Wasie et al., 2015). This discrepancy might be due to variability in geographical area, climate condition, system of rearing, awareness of hygiene of milking practice, and variations in the study methods and materials employed by the investigators.
In the present study, most of the milking personnel (94.2%) did not wash the udder before milking, and 78.6 % of the milking personnel did not use a separate towel to dry the udder after washing. This result was in agreement with a study done around Jigjiga city of the Somali Region that reported about 92% of respondents did not use udder washing before milking (Husein et al. 2013). However, the finding disagrees with a study conducted in southern Ethiopia (Gebremedhin et al. 2020) which reported 93.3% of milking personnel were washed udder before milking. The discrepancy might be due to the difference in awareness of milking personnel on milking practice in the study area.
Furthermore, 80% of respondents used tap water as their main source of water used for cleaning, and 20% used river/open well water as their main source of water for cleaning, but the difference was not statistically significant. The result was nearly in line with the study done in southern Ethiopia (Gebremedhin et al., 2020) that reported 97.5% and 11.8 % of respondents used tap water and well water, respectively.
The current study revealed that the prevalence of S. aureus increases as parity increases. Raw milk from lactating camels who gave many births was 3.52 times more likely to be contaminated with S. aureus when compared with raw milk from those who gave few and moderate births [AOR = 3.52; 95% CI: (1.104, 13.057); p ≤ 0.021]. The result was in agreement with a study done in Pakistan (Aqib et al., 2017) and a study done in Mukaturi and Sululta town of Oromia Region (Sema et al., 2019). This could be because as the parity increases, there is a high degree of contamination of the udder and milk through the milking process. Besides, a large amount of milk produced and the pressure on the teat canal forces the canals to be opened widely, allowing the entrance of microbes (Sema et al. 2019).
In the present study, the prevalence of S. aureus in raw camel milk was significantly associated with milking personnel who did not wash hands before milking. Raw milk from milking personnel who did not wash their hands before milking was 3.94 times more likely to be contaminated with S. aureus when compared with milk from those washed hands before milking [AOR = 3.94: 95% CI: (1.599, 9.716); p = 0.003]. This result was in line with a study conducted in Kenyan pastoral herds (Kashongwe et al. 2017). However, it disagrees with the study conducted in Nasarawa, Nigeria (Yakubu et al., 2020), which reported hand washing before milking was not statistically significant (p = 0.800). Sanitary milking habits are important to avoid the spreading of bacteria or their proliferation. The predominant source of the infection is the udder of infected camels, transmitted through milker's hands, utensils, towels and the environment (floor) in which the camels are kept (Elemo et al. 2017).
Prevalence of S. aureus in raw camel milk was significantly associated with drainage condition of milking place. Milk from poor drainage conditions of milking place was 4.62 times more likely to be contaminated with S. aureus compared to milk from good drainage condition of milking place [AOR = 4.62, 95% CI: (1.853, 11.557); p = 0.001]. The study was comparable with a previous study from Sululta Town, Oromia Region, Ethiopia (Sema et al. 2019), which reported the drainage condition of the milking area was significantly (x^2^ = 4.448, p = 0.035) associated with the prevalence of S. aureus in raw milk. Milking area should minimize the risk of contamination from any source, including accumulations of dung and slurry, dust, flies, birds or other animals (Clinical and Laboratory Standards Institute (CLSI) 2006).
The current study showed that the type of containers used for selling milk was associated with the prevalence of S. aureus in raw camel milk. Raw milk from vendors who utilise plastic water bottles as containers for selling milk were 8.4 times more likely to be contaminated when compared with raw milk from those who use wide‐necked aluminium container, wide‐ necked plastic containers and narrow‐necked plastic containers [AOR = 8.40, 95% CI: (1.258, 26.068) p = 0.028]. The use of plastic containers is not advisable, as it is sensitive to heat, and their surface was easily scratched by common cleaning systems. As a result, the surface is nearly impossible to clean with the common cleaning systems and provides hiding places for bacteria during sanitisation, which allows the multiplication of bacteria on milk contact surfaces (Pandey and Voskuil 2011).
In this current study, the antimicrobial susceptibility patterns of S. aureus against ten antimicrobial agents showed that all isolates were found to be 95.9% susceptible to cefoxitin and oxacillin, while 69.4% were resistant to amoxicillin. This result was nearly in agreement with a study done in Bangladesh (Jahan et al., 2015) and a study done by Rana et al. (2019) who reported 91.2% of isolated S. aureus were susceptible to oxacillin. In addition, the current study indicated 93.9% (46/49) of isolated S. aureus were susceptible to erythromycin, while 6.1% (3/49) were resistant to erythromycin. These results were comparable with the study done in China (Wei et al. 2018), in Nigeria (Yakubu et al. 2020) and in Kombolcha, Northern Ethiopia (Mesfin 2015). This might be because these antibiotics are not frequently used in the study area in veterinary services and perhaps in human medicine.
However, most of the isolated S. aureus were resistant to penicillin G (81.6%; n = 40 /49) and tetracycline (81.6%; n = 40 /49), which was comparable to the study conducted around Asella town, Arsi zone (Elemo et al. 2017), in Kazerun, Iran (100% resistance for both penicillin and tetracycline) (Rahi et al. 2020), and in Jigjiga city (Melese et al. 2016). Furthermore, the result was in line with the study done in Central Ethiopia (Emeru et al. 2019). The possible reason of the presence of high antibiotic resistance of S.aureus to tetracycline, penicillin G and amoxicillin is the indiscriminate and repeated use of these antibiotics in animal and human health. Furthermore, tetracycline and penicillin are the most commonly used antimicrobials in the treatment of infections in the livestock sector in Ethiopia (Gemeda et al. 2020), and many strains of S. aureus are now resistant to penicillin because they develop an enzyme known as beta‐lactamase or penicillinase (Van et al. 2020).
The present study showed that 85.7% (42/49) of S. aureus isolates were susceptible to ciprofloxacin, while two (4.1%) and five (10.2%) were intermediate and resistant, respectively. The current finding was nearly in agreement with a study conducted in Pakistan (100% susceptible) (Aqib et al. 2017), in part of Kaduna State, Nigeria (100% susceptible) (Okpo et al. 2018), and Algeria (100% susceptible) (Yakubu et al. 2020). In addition, the current study revealed that 77.6% of the isolated S. aureus were susceptible to chloramphenicol, while 14.3% were resistant. The finding was nearly in agreement with a study conducted in Al Jabal Al Akhdar of Eastern Libya (Abdurabbah et al. 2018) and a study in Jigjiga City of Somali Region (Melese et al. 2016). Moreover, the present study illustrated 67.3% of isolated S. aureus were susceptible to gentamicin and 28.6% were resistant. The finding was in nearly agreement with a study conducted in China (Jingsha et al. 2019).
The overall prevalence of the MDR rate of S. aureus isolated in this study was 48.97 % (n = 24/49). The most frequent MDR isolates were those exhibiting resistance to penicillin G, ampicillin, gentamicin, tetracycline and trimethoprim‐sulfamethoxazole at a frequency of 14.28 %. The present finding of the MDR rate of S. aureus isolated in this study was in line with the previous study conducted in Jigjiga City of the Somali Regional State (55.2 %) (Melese et al., 2016) and a study done in Asella town, Arsi zone (52.05%) (Elemo et al. 2017).
The resistance pattern of S. aureus against broad‐spectrum antibiotics illustrates an alarming situation, which needs special attention. The increasing number of MDR might be due to extensive misuse of antibiotic treatment in veterinary and the use of antibiotics for the preservation of milk. Moreover, tetracycline was used as a growth promoter in food animal production (Normanno 2005).
Conclusion and Recommendation
5
The study revealed that the overall prevalence of S. aureus isolated from raw camel milk in the Babile district was high, and the isolated S. aureus showed a 48.97% MDR rate. The isolated S. aureus from raw camel milk was more resistant to tetracycline and penicillin G, whereas cefoxitin, oxacillin and erythromycin were the most effective antimicrobial agents against S. aureus. Milk handling practice and parameters, including drainage condition of the milking place, not hand washing before milking, type of containers used for selling milk and parity of lactating camels, were statistically significant predictors of S. aureus prevalence in raw camel milk. Most of the respondents consumed raw milk without any heat treatment, and the milk was not cooled both after milking and before delivery to the market due to lack of chilling facilities. Thus indicating the possibilities for S. aureus milk contamination and intoxication that was a risk for consumers. The result indicates that the raw camel milk samples were produced and handled under poor hygienic conditions, posing a significant health risk to consumers. Consumption of raw camel milk should get concerns from concerned bodies. Based on this finding, we recommend the immediate development and implementation of effective, practical, and sustainable interventions to improve camel milk hygiene and safety in the study area, as well as to reduce staphylococcal food poisoning in the area.
Author Contributions
All authors made a significant contribution to the work reported, either in the conception, or the design of the study, conducting the actual study, collection of data, analysis and interpretation of data, or drafting the manuscript. All authors were critically revising the manuscript for important intellectual content and reviewed the final version to be published. We all have decided to which journal the article will be submitted. We all agree to be responsible and accountable for any contents of the article.
Conflicts of Interest
The authors declare no conflicts of interest.
Peer Review
The peer review history for this article is available at https://www.webofscience.com/api/gateway/wos/peer‐review/10.1002/vms3.70438.
Supporting information
Supporting Fig. 1: Mannitol salt agar media with growth of S.aureus mannitol fermenter colony. Supporting Fig. 2: A blood agar media with β‐hemolysis colony of S.aureus. Supporting Fig. 3: Antibiotic susceptibility test with different antibiotic.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abdulkadhim, M. 2012. “Prevalence of Methicillin Resistance Staphylococcus aureus in Cattle and She‐camels Milk at Al‐Qadisyia Province.” Al‐Anbar Journal of Veterinary Sciences 5, no. 2: 63–67.
- 2Abdurabbah, E. M. , N. M. Eissa , S. M. Hussieny , and Y. I. Mahmoud . 2018. “Fares NH. Isolation of Coagulase Positive Staphylococci From She‐Camel Milk at Eastern Libya and Their Drug Susceptibility Patterns.” Australian Journal of Basic and Applied Sciences 12, no. 8: 118–123.
- 3Aljahani, A. H. , K. M. Alarjani , Z. K. Hassan , et al. 2020. “Molecular Detection of Methicillin Heat‐resistant Staphylococcus aureus Strains in Pasteurized Camel Milk in Saudi Arabia.” Bioscience Reports 40, no. 4.10.1042/BSR 20193470 PMC 716725432202302 · doi ↗ · pubmed ↗
- 4Amentie, T. , M. Eshetu , Y. Mekasha , and A. Kebede . 2016. “Milk Postharvest Handling Practices Across the Supply Chain in Eastern Ethiopia.” Journal of Advanced Veterinary and Animal Research 3, no. 2: 112–126.
- 5Ana, G. A. , G. V. Tomás , and B.‐V. Jorge , et al. 2020. “ Staphylococcus aureus Exotoxins and Their Detection in the Dairy Industry and Mastitis.” Toxins MDPI 12: 537.10.3390/toxins 12090537 PMC 755167232825515 · doi ↗ · pubmed ↗
- 6Aqib, A. I. , M. Ijaz , A. Z. Durrani , et al. 2017. “Prevalence and Antibiogram of Staphylococcus aureus, a Camel Mastitogen From Pakistan.” Pakistan Journal of Zoology 49, no. 3: 861–867.
- 7Aqib, A. I. , M. Ijaz , S. H. Farooqi , and A. Raza . 2018. Dairy Staphylococcus aureus: Epidemiology, Drug Susceptibilities, Drug Modulation, and Preventive Measures. Staphylococcus aureus: Intech Open.
- 8Aqib, A. I. , M. Ijaz , R. Hussain , et al. 2017. “Identification of Coagulase Gene in Staphylococcus aureus Isolates Recovered From Subclinical Mastitis in Camels.” Pakistan Veterinary Journal 37, no. 2: 160–164.