Unilateral Tensor Fascia Suralis: A Rare Type Ia Variant and Its Clinical Implications
Sayan Biswas, Karan Kumar, Praisy Joy, Manisha R Gaikwad

TL;DR
A rare muscle variant in the thigh and leg is described, which could be mistaken for a tumor or cause nerve issues.
Contribution
A new Type Ia variant of tensor fascia suralis with dual muscle bellies and distinct innervation is reported.
Findings
The variant has two fleshy muscle bellies separated by an intermediate tendon.
Both muscle bellies are innervated by the tibial nerve via different pathways.
This anomaly may mimic soft tissue tumors or cause nerve compression.
Abstract
Tensor fascia suralis is a rare supernumerary muscle in the posterior thigh and leg, with a male preponderance as reported in the literature. We present a unique Type Ia variant discovered during cadaver dissection of the left lower limb, originating from the long head of the biceps femoris and terminating at the medial head of the gastrocnemius. Unlike previously reported cases, this variant exhibited two distinct fleshy muscle bellies at origin and insertion, separated by an intermediate tendon. Both bellies received innervation from the tibial nerve, with the upper belly supplied directly via the sciatic nerve and the lower belly via a branch penetrating the gastrocnemius. This anomaly has significant clinical implications, potentially mimicking soft tissue tumors on imaging or contributing to nerve compression syndromes. Awareness of such variants is crucial for accurate diagnosis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
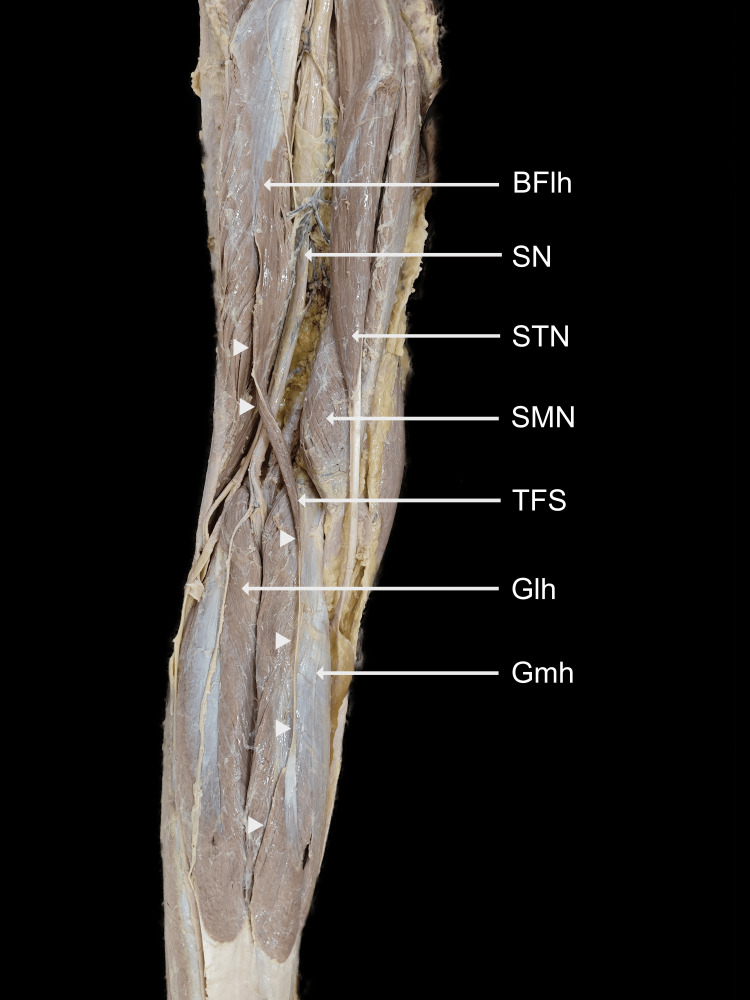 Figure 1
Figure 1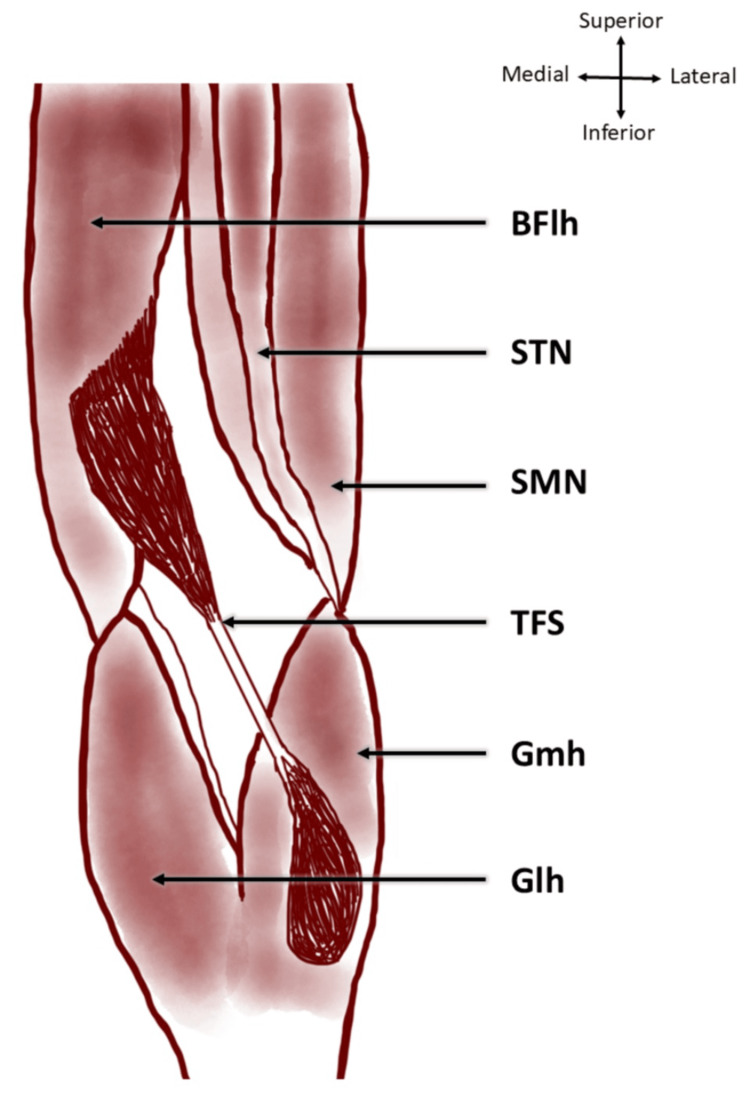 Figure 2
Figure 2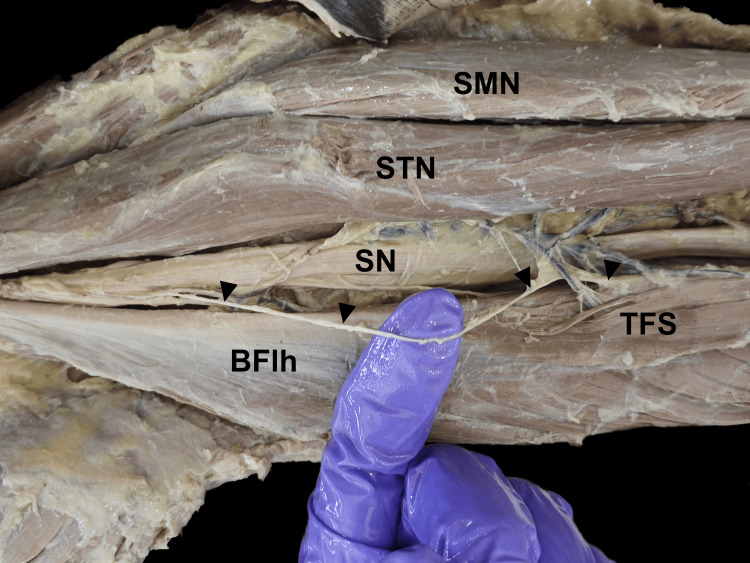 Figure 3
Figure 3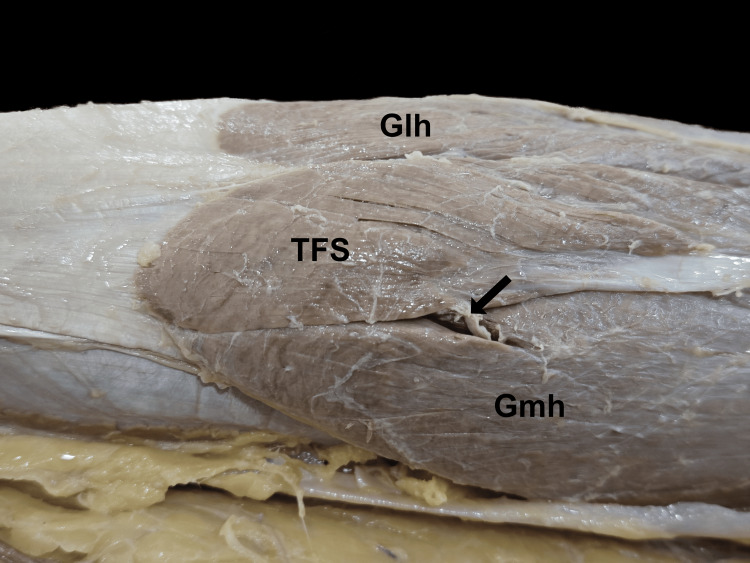 Figure 4
Figure 4| Sl. no. | Year | Author | Side | Sex | Subtype | Nerve | Reference |
| 1 | 1813 | Kelch | - | - | Ia | - | [ |
| 2 | 1870 | Gruber | - | - | Ib | - | [ |
| 3 | 1872 | Turner | Right | - | Ib | - | [ |
| 4 | 1872 | Turner | - | - | Ia | - | [ |
| 5 | 1873 | Gruber | Left | M | Ia | - | [ |
| 6 | 1873 | Gruber | Right | M | Ib | - | [ |
| 7 | 1873 | Gruber | Left | M | Ib | - | [ |
| 8 | 1884 | Turner | - | - | Ia | - | [ |
| 9 | 1879 | Gruber | Left | M | Ic | - | [ |
| 10 | 1879 | Gruber | Left | M | Ia | - | [ |
| 11 | 1881 | Halliburton | Right | F | III | - | [ |
| 12 | 1897 | Gruber | - | - | Ia | - | [ |
| 13 | 1911 | Klaatsch | Right | M | Ic | TN | [ |
| 14 | 1913 | Schaeffer | Left | M | Ia | - | [ |
| 15 | 1924 | Barry and Bothroyd | Left | M | III | TN | [ |
| 16 | 1935 | Kawai | - | - | Ib | - | [ |
| 17 | 1940 | Mogi | Right | M | Ib | TN | [ |
| 18 | 1954 | Nonaka and Ishii | - | - | II | - | [ |
| 19 | 1985 | Miyauchi et al. | Right | M | II | - | [ |
| 20 | 1995 | Chason et al.* | - | - | Ib | - | [ |
| 21 | 1995 | Sinav et al. | Bilateral | F | Ia | TN | [ |
| 22 | 1998 | Somayaji et al. | - | - | II | TN | [ |
| 23 | 2001 | Seema and Balalkrishna | Right | - | III | - | [ |
| 24 | 2002 | Montet et al.* | Right | M | Ib | - | [ |
| 25 | 2004 | Okamoto et al. | Right | F | Ic | CPN | [ |
| 26 | 2006 | Tubbs et al. | Right | M | Ib | TN | [ |
| 27 | 2006 | Kumar | Right | M | II | TN | [ |
| 28 | 2009 | Kim et al. | Right | F | Ia | CPN | [ |
| 29 | 2009 | Luca et al. | Right | M | Ia | TN | [ |
| 30 | 2011 | Padmalatha et al. | Left | M | Ib | - | [ |
| 31 | 2014 | Feimster et al. | Bilateral | M | Ia | TN | [ |
| 32 | 2014 | Sowmya et al. | Right | M | Ia | TN | [ |
| 33 | 2015 | Gandhi et al. | Bilateral | M | Ia | TN | [ |
| 34 | 2015 | Kim et al.* | Right | M | Ib | - | [ |
| 35 | 2016 | Rajendiran and Murugesan | Left | M | Ia | TN | [ |
| 36 | 2017 | Dickson and Koulouris* | Left | M | Ia | - | [ |
| 37 | 2017 | Oommen et al. | Left | M | II | - | [ |
| 38 | 2017 | Arakawa et al. | Right | M | Ia | TN | [ |
| 39 | 2017 | Bale and Herrin | Bilateral | M | Ia | - | [ |
| 40 | 2017 | Tsifountoudis et al.* | Right | M | Ib | - | [ |
| 41 | 2018 | Elliott | Right | M | Ib | - | [ |
| 42 | 2019 | George et al. | Left | M | III | CPN | [ |
| 43 | 2020 | Boudier-Revéret et al.* | Bilateral | M | Ib | - | [ |
| 44 | 2021 | Olewnik et al. | Right | M | III | - | [ |
| 45 | 2021 | Olateju | Left | M | Ia | TN | [ |
| 46 | 2023 | Bale et al. | Left | M | Ia | - | [ |
| 47 | 2024 | Swancutt et al. | Bilateral | F | Ia | - | [ |
| 48 | 2024 | Snow et al. | Left | - | Ia | - | [ |
| 49 | 2025 | Lee et al.* | Right | M | Id | - | [ |
| 50 | 2025 | Present case report | Left | M | Ia | TN | - |
| Parameters | Number of cases | Reference |
| Study types | Gross dissection: 43 |
[ |
| Radiological: 7 |
[ | |
| Side | Right: 20 |
[ |
| Left: 15 |
[ | |
| Bilateral: 6 |
[ | |
| Unknown: 9 |
[ | |
| Sex | Male: 33 |
[ |
| Female: 5 |
[ | |
| Unknown: 12 |
[ | |
| Innervation | Tibial nerve: 15 |
[ |
| Common peroneal nerve: 3 |
[ | |
| Unknown: 32 |
[ | |
| Subtypes | Ia: 22 |
[ |
| Ib: 14 |
[ | |
| Ic: 3 |
[ | |
| Id: 1 |
[ | |
| II: 5 |
[ | |
| III: 5 |
[ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyofascial pain diagnosis and treatment
Introduction
The tensor fascia suralis (TFS) is a rare supernumerary muscle located in the lower posterior thigh and leg. It usually originates from one of the hamstrings and inserts into the gastrocnemius, calcaneal tendon, or the crural fascia, and hence is also called ischioaponeuroticus [1]. With a prevalence rate of 1.27%, the presence of this muscle is often incidental, discovered during dissections or imaging studies, more commonly in men. It is mostly supplied by the tibial nerve, which may be compressed. TFS acts as a weak flexor of the knee joint when present. Anatomical variations of this kind may have implications in surgical procedures and clinical imaging [2].
Case presentation
During the routine dissection of an Indian male cadaver, we identified aberrant muscular fibers in the left lower limb, extending between the long head of the biceps femoris and the insertion of the gastrocnemius tendon (Figures 1, 2).
Dissected posterior compartments of the left lower limb. The TFS muscle can be seen originating from the long head of the biceps femoris and descending to terminate on the medial head of the gastrocnemiusWhite arrowheads show the course of the TFSTFS, tensor fascia suralis; BFlh, long head of biceps femoris; SN, sciatic nerve; STN, semitendinosus; SMN, semimembranosus; Gmh, medial head of gastrocnemius; Glh, lateral head of gastrocnemius
The TFS muscle originating from the long head of the biceps femoris and terminating on the medial head of gastrocnemiusTFS, tensor fascia suralis; BFlh, long head of biceps femoris; STN, semitendinosus; SMN, semimembranosus; Gmh, medial head of gastrocnemius; Glh, lateral head of gastrocnemiusImage credit: This is an original image created by the author Sayan Biswas
From the biceps femoris, the muscle belly descended inferomedially as a common tendon over semitendinosus, enclosed in a loose sheath. Dissection revealed that this tendon was separate from the semitendinosus. It descended further down the back of the leg, forming a spindle-shaped muscular slip, which was broad and flattened in the anteroposterior aspect. It terminated by merging with the tendon of the medial head of the gastrocnemius muscle. The upper belly originated at a distance of 16 cm from the ischial tuberosity and measured 20 cm in length and 2.3 cm in width. The intermediate tendon was 11 cm long, 1.2 mm wide, and 0.6 mm thick, while the lower belly was observed to be 8.5 cm in length and 2.5 cm in width. The measurements were taken using a calibrated steel tape and a digital vernier calliper. The upper belly received innervation from a branch carrying the tibial component of the sciatic nerve above the popliteal fossa (Figure 3), whereas the lower belly was innervated by a branch of the tibial nerve after it pierced through the medial head of the gastrocnemius (Figure 4). There were no anatomical variations in the contralateral limb.
The upper belly of the TFS receiving innervation from a branch of the sciatic nerve (black arrowheads)TFS, tensor fascia suralis; SN, sciatic nerve; BFlh, long head of biceps femoris; STN, semitendinosus; SMN, semimembranosus
The lower belly of the TFS inserted into the tendon of the medial head of the gastrocnemius and received nerve supply from a branch of the tibial nerve that pierces through the medial head of the gastrocnemius muscle bellyThe black arrow shows the nerve supplyTFS, tensor fascia suralis; Gmh, medial head of gastrocnemius; Glh, lateral head of gastrocnemius
Discussion
The presence of the TFS is a rare anatomical variant, with a prevalence rate of only 1.27%. Various studies have described muscular anomalies in the posterior compartment of the thigh and leg, attributing them to evolutionary remnants or adaptations for additional muscle function. First appearing in the literature in 1813, a proper classification system for TFS was developed more than two centuries later [2].
Although the insertion can vary, the TFS has been classified by Bale et al. into three types: type I where it originates from one of the hamstring muscles (Ia: long head of biceps femoris, Ib: semitendinosus, Ic: short head of biceps femoris, and Id: semimembranosus), type II where it originates in the form of double head from semitendinosus and biceps femoris, and type III comprising of all other variations. This case represents a variant of type Ia as it originates from the long head of the biceps femoris. These variants originate or insert as aponeurotic or tendinous structures with the muscle belly lying either at the origin or in the middle [2,3]. It consists entirely of muscle belly in cases where muscle fibers are transversely oriented [4]. Other variants include origin from the femur [1,5] or from the semimembranosus muscle [6]. An extensive literature search showed no more than 49 cases of TFS being published to date (Table 1), a summary of which has been provided in Table 2. The most common variant of this muscle was type Ia. It was mostly found in men and was innervated mainly by the tibial nerve.
This case is unique in that it features a sequence of a muscle belly, an intermediate tendon, followed by the reforming of a flattened muscular slip. Although double muscle bellies have been seen in TFS, they both lie at the origin, unlike at either end, as observed in the present case [8]. The only case having two bellies separated by an intermediate tendon was reported by Olateju [17]. However, the proximal belly had a commonly observed tendinous origin, unlike the fleshy origin in our case. Moreover, both bellies in this case were supplied by tibial nerve components, but the upper belly from the sciatic nerve directly and the lower one after the sciatic nerve had divided in the popliteal fossa.
During development, the ventral muscle mass of the lower limb buds gives rise to the posterior compartment muscles of both thigh and leg under the influence of Shh signaling [19]. Hence, although the embryological basis of TFS is not well established, it is thought to be due to the failure of the disappearance of the embryological fibrous connection that spans the deep fascia of the leg and the biceps femoris tendon [2]. It may also develop as a remnant slip during embryological division of the knee flexor muscle group into individual hamstring muscles [7]. Thus, TFS may be seen with other anomalies in lower limb musculature [15,18]. It is also akin to some muscles found in certain mammals, an example being the abductor cruris caudalis seen in dogs and cats [20].
From a clinical perspective, the presence of this muscle may pose diagnostic challenges. It may be mistaken for soft tissue tumors or abnormal muscle hypertrophy in radiological investigations such as MRI and ultrasound scans, or during clinical examination. Additionally, as the TFS is located near key structures like the sciatic nerve, popliteal vessels, hamstrings, and gastrocnemius, it may lead to compression syndromes and contribute to motor and sensory impairments in the lower leg and foot, necessitating careful evaluation by clinicians [6,9]. Surgeons performing procedures in the posterior compartment of the thigh and leg should be aware of such variations to prevent inadvertent injuries, particularly during hamstring graft harvesting or reconstructive surgeries.
Functionally, the TFS may contribute to biomechanical movements of the lower limb, particularly in assisting flexion at the knee and plantarflexion at the ankle. Biomechanical analysis by Snow et al. observed that the maximal isometric force stood at 8.10 N, thus assisting the surrounding popliteal muscles, which have 9-27 times the force [7]. Athletes presenting with unexplained posterior thigh pain or stiffness may benefit from imaging and physical examination, considering the possibility of an accessory muscle structure. Targeted physiotherapy and myofascial release techniques may help in alleviating symptoms in such cases [14].
Conclusions
TFS having two muscle bellies without any tendinous structure on either end has not been reported before. It is a rare but clinically significant muscle, especially in posterior thigh and knee surgeries. Recognizing its variant morphology is essential for preventing nerve damage and ensuring accurate clinical and radiological diagnosis and surgical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1"Popliteofascial muscle" or rare variant of the tensor fasciae suralis?Folia Morphol (Warsz) OlewnikŁ Gonera B Kurtys K Tubbs RS Polguj M 103710428020213316935110.5603/FM.a 2020.0138 · doi ↗ · pubmed ↗
- 2Tensor fasciae suralis - prevalence study and literature review Morphologie Bale LS Damjanovic MM Damjanovic IG Di Maio NM Herrin SO 10076210820243832501810.1016/j.morpho.2024.100762 · doi ↗ · pubmed ↗
- 3Tensor fasciae suralis J Anat Barry D Bothroyd JS 382383581924 https://pmc.ncbi.nlm.nih.gov/articles/PMC 1249731/17104034 PMC 1249731 · pubmed ↗
- 4An anomalous muscle in the superficial region of the popliteal fossa, with special reference to its innervation and derivation Ann Anat Okamoto K Wakebe T Saiki K Nagashima S 5555591200410.1016/S 0940-9602(04)80106-715646291 · doi ↗ · pubmed ↗
- 5Clinical importance of tensor fasciae suralis arising from linea aspera along with short head of biceps femoris: a rare anomaly Anat Cell Biol George BM Nayak SB Marpalli S 90925220193098445910.5115/acb.2019.52.1.90PMC 6449577 · doi ↗ · pubmed ↗
- 6Symptomatic tensor fasciae suralis muscle as accessory muscle at popliteal fossa in young soldier: a case report BMC Musculoskelet Disord Lee YS Lee YH Park JS Ahn GY Hwang SH Lee CK 1252620253991575310.1186/s 12891-025-08351-2PMC 11803954 · doi ↗ · pubmed ↗
- 7Gross and functional analyses of the tensor fasciae suralis muscle with magnetic resonance imaging Transl Res Anat Snow EL Fox BC Eide HA Vilburn MJ 100325372024
- 8An anomalous muscle in the region of the popliteal fossa: a case report J Anat Soc India Kumar G 6568552006 https://cir.nii.ac.jp/crid/1571135650856960256