Renal vascular patterns assessment before robot-assisted partial nephrectomy: a video-based correlation with hilum dissection
O. S. Barnoiu, H. R. Yazdani, A. V. Andersen

TL;DR
This study uses surgical videos to assess how kidney blood vessel patterns affect the time needed to control the renal hilum during robot-assisted partial nephrectomy.
Contribution
The study introduces a video-based method to evaluate factors influencing renal hilum control during RAPN, focusing on vascular anatomy.
Findings
Previous renal surgery and complex vascular anatomy increase time to hilum control.
Renal hilum control time accounts for about 15% of the total operation time.
Surgeon and surgical approach had no significant impact on hilum control time.
Abstract
Surgical video review (SVR) is an emerging tool for assessing patient outcomes, especially in complex surgeries such as robot-assisted partial nephrectomy (RAPN). Adhesive probability and morphological scores are used to evaluate fat management and warm ischemia, respectively; however, the factors influencing renal hilum control (RHC) during RAPN have not yet been assessed. The aim of this study is to use SVR to identify the renal vascular patterns and factors that influence RHC. We evaluated 60 surgical video recordings of patients undergoing RAPN in 2023–2024, and measured the time to hilum control (THC) and total operation time (TOT) using a stopwatch. Patient and surgical factors were recorded and SPSS software was used to identify the correlation of these factors and vascular patterns with THC. We observed a median THC of 22.7 min representing 15.1% of TOT. A significant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
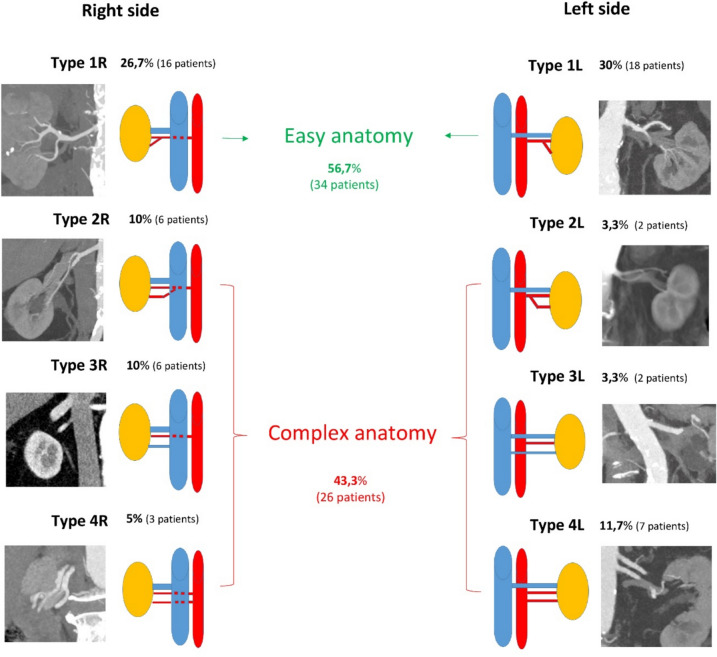 Figure 1
Figure 1- —Sørlandet Sykehus HF
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal and Vascular Pathologies · Renal cell carcinoma treatment · Pediatric Urology and Nephrology Studies
Introduction
Minimally invasive partial nephrectomy (PN), whenever feasible, is the standard of care for patients diagnosed with T1a and T1b kidney cancer [1]. However, this approach is technically challenging and requires a detailed understanding of renal and tumour surgical anatomy to optimise oncological, functional and perioperative outcomes [2].
Contrast-enhanced computer tomography (CT) of the abdomen is the reference standard for primary imaging of renal tumours and the vascular system. Study the renal arterial anatomy via CT scan has been previously used for arterial tree representation [3]. In approximately 75% of cases, a single renal artery and vein are present, but a high percentage (15–20%) of patients also show anatomic variations such as duplication or early branching [2]. Disposition of the renal hilar structures and their numbers are significantly more variable than the classical pattern given in standard textbooks of anatomy, and a precise knowledge of both normal and variant anatomies of renal hilum is essential in the era of robotic surgery [4].
Robotic surgery platforms enable high-quality video recordings, providing greater magnification and closer views of anatomical details. Surgical video review (SVR) is an emerging tool for assessing patient outcomes [5], especially in complex surgeries such as robot-assisted PN (RAPN). Three key surgical phases are critical during RAPN: renal hilum control (RHC), fat management and warm ischemia time (WIT). Adhesive probability and morphological scores are respectively used to evaluate fat management [6] and warm ischemia [7], along with SVR; however, the factors influencing RHC during RAPN have not yet been assessed.
The aim of this study is to use SVR to identify the factors that influence RHC according to the renal vascular patterns identified via renal CT scan.
Material and methods
The storage of recorded surgical videos for a period of time is mandatory in Norway to ensure quality of healthcare services and provide medicolegal evidence. This requirement allowed us to retrospectively review surgical video recordings of 60 consecutive patients undergoing RAPN at our institution between January 2023 and June 2024. All procedures were performed on T1a tumours using Intuitive Xi robotic systems (Intuitive™, Sunnyvale, CA, USA). As part of the kidney cancer surgical team, one surgeon (O.B.) reviewed the video recordings and measured time to hilum control (THC) and total operation time (TOT) using a digital stopwatch and exact visual cues for starting and ending points. For THC, we defined the starting point as when the monopolar-curved scissors’ cut function is first used to dissect the renal hilum (gonadal vein on the left side, inferior vena cava (IVC) on the right side), right after colon decollation for the transperitoneal approach or the posterior opening of Gerota’s fascia, for the retroperitoneal approach. The ending point for THC was defined as when the Hem-o-lock clip is applied to the vessel loop surrounding the renal artery. In cases of more than one artery or the need to clamp the renal vein, the ending point was defined as when the Hem-o-lock clip is applied to the vessel loop surrounding the last vascular structure of the hilum. The TOT compromised the time from the first to the last use of the robotic instruments.
We assessed the renal vascular patterns using evaluation of the arterial and venous phase of the CT scans, performed preoperatively. Eight different vascular patterns (Fig. 1) were identified according to side, four on the right (Type 1R, 2R, 3R and 4R) and four on the left (Type 1L, 2L, 3L and 4L). Also the number of arteries or veins and proximity of the artery bifurcation to aorta were taken into consideration. We defined the anatomy of the renal hilum as easy if only one artery with a late bifurcation (lateral for the IVC on the right side, and more than 2 cm from the aorta on the left side) and one vein were present (Type 1L and 1R). Early bifurcation of the artery (behind IVC on the right side for Type 2R, and less than 2 cm from the aorta on the left side for type 2L) and more than one vein (Type 3R and 3L) or artery (Type 4R and 4L) was defined as a complex anatomy.Fig. 1. Vascular patterns identified on preoperative CT scan
Patient factors such as age, BMI, previous renal surgery, inflammation (pyelonephritis or pancreatitis), radiation and immunotherapy were collected from patients’ medical records, as well as vascular anatomy and patterns observed in CT scans. Surgical factors such as intraoperative bleeding during RHC, surgeon, and approach were recorded and analysed using descriptive statistics.
We used SPSS software, including independent samples t-test, one-way ANOVA and Bonferroni multiple comparisons to identify the correlation of these factors and vascular patterns with THC. Additionally, we used stepwise multivariable regression models to assess the predictors, and statistical significance was set at p < 0.05.
Results
Population and surgical features are summarised in Table 1. The cohort comprised 72% males and had a median age of 67.5 years and an interquartile range (IQR) of 15. Most of the patients did not have previous kidney surgery, inflammation, radiotherapy or immunotherapy. The operations were distributed between three surgeons in a 1:1.8:1.5 manner and only 18.3% of RAPN were performed via a retroperitoneal approach.Table 1. Population demographics and surgical featuresVariableOverall(n = 60)VariableOverall(n = 60)Age (years)Median [IQR]67.5 (15)Vascular patternsType 1RType 2RType 3RType 4RType 1LType 2LType 3LType 4 L16 (26.7%)6 (10%)6 (10%)3 (5%)18 (30%)2 (3.3%)2 (3.3%)7 (11.7%)GenderMale43 (71.7%)Female17 (28.3%)Previous surgeryYes4 (6.7%)No56 (93.3%)Previous Inflamation**AnatomyYes2(3.3%)Easy34 (56.7%)No58 (96.7%)Complex26 (43.3%)Previous radiotherapy**OperatorYes1 (1.7%)114 (23.3%)No59 (98.3)225 (41.7%)321 (35%)Previous imunotherapy**Surgical approachYes2 (3.3%)Transperitoneal49 (81.7%)No58 (96.7%)Retroperitoneal11 (18.3%)BMIMedian [IQR]28.1 (6)Time to hilum control(minutes)**SideMedian [IQR]22.7 (17)Right31 (51.7%)Left29 (48.3%)Number of arteries**Total operative time150 (83.3%)Median [IQR]133.6 (40)29 (15%)31 (1.7%)Number of veins**Intraoperative bleeding153 (88.3%)Yes4 (8.7%)27 (11.7%)No56 (91.3%)
More than 80% of the patients had only one artery or one vein and the eight vascular patterns are depicted in Fig. 1. Type 1R and 1L were characterised as easy anatomy and represented more than half of the patients (56.7%).
We observed a median THC of 22.7 min, representing 15.1% of TOT. A significant correlation was found between previous renal surgery and longer THC (p = 0.033), as presented in Table 2.Table 2. Factors correlated with time to hilum control and the percent from total operative timeVariableNTHCPercent THC/TOTMean(minutes) /CorrelationpMean (%)/Correlation. pGender0.2650.281Male 4324.917.2Female1721.217.7Previous surgery0.0330.010Yes5623.116.7No435.626.5Previous inflammationYes5823.50.12917.10.061No236.127.1Previous radiationYes5923.90.98117.40.588No124.213.1Previous immunotherapyYes5824.10.62117.40.673No219.915.1Side*0.2310.672Right3122.216.9Left2925.717.7Renal arteries15021.90.00716.30.0512934.722.93125.417.8Renal veins0.4820.44615324.317.62721.015.3AnatomyEasy3419.70.00114.80.002Complex2629.420.7*Vascular patternType 1RType 2RType 3RType 4RType 1LType 2LType 3LType 4L1616.50.0213.10.03634.525.9620.615.8330.722.01822.516.3224.318.9223.812.8735.122.6Operator0.7530.22011425.919.522523.417.932123.115.2Surgical approach0.3870.062Transperitoneal4923.316.5Retroperitoneal1126.621.1Intraoperative bleeding*****0.050.242Yes5623.117.2No434.618.7Age60.0850.5160.0160.902BMI60.0890.4990.0860.514Bold and bold Italic for "p" means p<0.05THC time to hilum control, TOT total operative time, BMI body mass indexANOVA/t-test***Pearson
Having a complex vascular anatomy (p = 0.001) with a particular vascular pattern (p = 0.02) and more than one kidney artery (p = 0.007) correlated with longer THC. The Bonferroni multiple comparisons of the vascular patterns demonstrated that type 2R (renal artery bifurcation behind the IVC) and 4L (more than one main artery on the left side) were significantly associated with longer THC compared to the other vascular patterns (Table 3).Table 3. Bonferroni multiple comparisons having time to hilum control as the dependent variable(I) Vascular pattern(J) Vascular patternMean difference (I-J)Std. errorSig95% Confidence IntervalLower boundUpper boundType 1RType 2R−18.01354.73790.011−33.616−2.411Type 3R−4.06084.73791.000−19.66411.542Type 4R−14.19136.22680.750−34.6976.315Type 1L−5.97563.40061.000−17.1745.223Type 2L−7.74697.42281.000−32.19216.698Type 3L−7.31357.42281.000−31.75817.131Type 4L−18.52784.48500.004−33.298−3.758Type 2RType 1R18.01354.73790.0112.41133.616Type 3R13.95285.71410.505−4.86532.771Type 4R3.82226.99831.000−19.22526.869Type 1L12.03804.66550.357−3.32727.403Type 2L10.26678.08091.000−16.34636.879Type 3L10.70008.08091.000−15.91237.312Type 4L−0.51435.50621.000−18.64817.619Type 3RType 1R4.06084.73791.000−11.54219.664Type 2R−13.95285.71410.505−32.7714.865Type 4R−10.13066.99831.000−33.17712.916Type 1L−1.91484.66551.000−17.27913.450Type 2L−3.68618.08091.000−30.29822.926Type 3L−3.25288.08091.000−29.86523.360Type 4L−14.46715.50620.316−32.6003.666Type 4RType 1R14.19136.22680.750−6.31534.697Type 2R−3.82226.99831.000−26.86919.225Type 3R10.13066.99831.000−12.91633.177Type 1L8.21576.17191.000−12.11028.541Type 2L6.44449.03481.000−23.30936.198Type 3L6.87789.03481.000−22.87636.631Type 4L−4.33656.82961.000−26.82818.155Type 1LType 1R5.97563.40061.000−5.22317.174Type 2R−12.03804.66550.357−27.4033.327Type 3R1.91484.66551.000−13.45017.279Type 4R−8.21576.17191.000−28.54112.110Type 2L−1.77137.37681.000−26.06522.522Type 3L−1.33807.37681.000−25.63222.956Type 4L−12.55224.40850.176−27.0701966Type 2LType 1R7.74697.42281.000−16.69832.192Type 2R−10.26678.08091.000−36.87916.346Type 3R3.68618.08091.000−22.92630.298Type 4R−6.44449.03481.000−36.19823.309Type 1L1.77137.37681.000−22.52226.065Type 3L0.43339.89711.000−32.16033.027Type 4L−10.78107.93531.000−36.91415.352Type 3LType 1R7.31357.42281.000−17.13131.758Type 2R−10.70008.08091.000−37.31215.912Type 3R3.25288.08091.000−23.36029.865Type 4R−6.87789.03481.000−36.63122.876Type 1L1.33807.37681.000−22.95625.632Type 2L−0.43339.89711.000−33.02732.160Type 4L−11.21437.93531.000−37.34714.918Type 4LType 1R18.52784.48500.0043.75833.298Type 2R0.51435.50621.000−17.61918.648Type 3R14.46715.50620.316−3.66632.600Type 4R4.33656.82961.000−18.15526.828Type 1L12.55224.40850.176−1.96627.070Type 2L10.78107.93531.000−15.35236.914Type 3L11.21437.93531.000−14.91837.347Bold and bold Italic for "p" means p<0.05
Intraoperative bleeding during RHC was low (8.7%) and correlated with longer THC (p = 0.05), though no significant difference was found between surgeons (p = 0.753) or surgical approach (transperitoneal vs. retroperitoneal, p = 0.87).
After stepwise regression, the best model identified to predict THC included anatomical complexity and previous surgery (R-square = 0.281, p = 0.006), as shown in Table 4.Table 4. Stepwise regression analyses for warm ischemia time, excision time, reconstruction time and intermediate timeModel summaryModelRR squareAdjusted R squareStd. error of the estimateChange statisticsR square changeF changedf1df2Sig. F Change10.423^a^0.1790.165628.4900.17912.673158 < 0.00120.530^b^0.2810.256593.2830.1028.0881570.006^a^Predictors: (Constant), Anatomy Complexity^b^Predictors: (Constant), Anatomy Complexity, Previous Surgery
Discussion
Our present study identified, on CT scan, several patterns according to the disposition of the vascular structures in the renal hilum. The analyses revealed which patterns correlate to a more complex anatomy and longer THC.
To the best of our knowledge, no data are available on intraoperative video documentation review for RHC assessment during RAPN. Previous studies have assessed the importance of SVR. For example, De Backer et al. [5] considered 100 RAPNs and showed that surgical phase duration can be correlated with certain clinical outcomes. Kim et al. [6] tested SVR to assess the Mayo adhesive probability score and perirenal fat dissection time. Additionally, our group used SVR to evaluate WIT during RAPN and its impact on surgical margins and complication rate, in a previous study [7].
We found THC to be a relatively short portion (15%) of the TOT. For the present study, TOT depicts the total console surgery time as the time used to achieve pneumoperitoneum or docking the robot were not taken into account. De Backer et al. [5] also found a short time to hilum control with a median of 16 (±11.5) minutes, as compared to 22 min in our study. This could be due to including patients with redo RAPN and complex vascular anatomy in our cohort. Of the 100 patients in the cohort of De Backer et al., 77 procedures were performed offclamp that requires less dissection of all the hilar structures.
Previous renal surgery was registered in four of the patients who underwent a redo RAPN for tumour resection elsewhere in the kidney than previous resection bed. It correlated to longer THC as more fibrosis around the vascular structures in the hilum needed to be dissected in order to achieve RHC. No statistical correlation was found between longer THC and previous inflammation like pyelonephritis or pancreatitis, previous radiotherapy, or previous immunotherapy. This finding could be biased by the low number of patients (only one or two) who did not have such previous conditions. Though previous abdominal surgery poses surgical challenges for PN [8], several studies identified no impact on the outcomes of RAPN [9, 10]. Redo RAPN is considered an effective approach [11], and evidence indicates good feasibility and safety, though it is a challenging procedure [12]. One challenge is RHC and it makes sense that more time is used to dissect the vascular structures, as more fibrosis around the hilar structures is present from previous RHC. Though RAPN remains the preferred option for treating small renal masses, percutaneous cryoablation is a valid alternative, particularly for challenging patients, as shown by Iossa et al. [13]. Two out of four patients who underwent redo RAPN were performed retroperitoneally. This could have biased our results together with a disproportioned percent of only 18% of the patients performed a retroperitoneally approach. This could also explain why we registered longer THC in the retroperitoneal group.
The anatomy of the renal vascular system and its application to PN was initially presented by Graves in 1954 with a special focus on segmental branching of the renal artery and its role in achieving selective ischemia [14]. Later, Trivedi et al. [15] identified six vascular branching patterns of segmental renal artery in an anatomical study and stated that knowledge of these patterns is essential to effective surgical planning in cases of PN and preventing complications. Clamping the segmental renal artery instead of the main renal artery during PN is a promising technique to decrease WIT, and understanding vascular branching patterns is essential for an appropriate hilar approach. However, selective or superselective clamping do not provide better renal function preservation than renal artery conventional clamping, as shown in systematic reviews [16] and randomized controlled trials [17]. This places doubt on the benefit of these techniques which additionally has higher risk of bleeding. To the best of our knowledge, no data are available on renal vascular anatomy with focus on conventional clamping, and our study identified vascular patterns that help for a more detailed understanding of renal vascular anatomy including cases of renal hilar masses, where RAPN is a promising technique [18].
Multiple authors have described the arrangement of renal hilar structures, through anatomical studies, identifying several patterns [4, 19] which included the renal pelvis into their classifications. We used vascular structures in our classification as only the vein and artery are dissected during the RHC for PN. We identified eight patterns, four for each side, including both the normal structure and variations. A complete understanding of underlying normal and aberrant renal anatomy, coupled with patient- and tumour-specific anatomical characteristics, represents the foundation for proper preoperative surgical planning for PN [20]. We determined that having more than one renal artery requires longer THC as more time is expected to be used to dissect all the arteries to be clamped. In our classification, we did not include small accessory arteries that did not need to be clamped during WIT. An early bifurcation of the renal artery on both sides but especially on the right side, as the artery passes behind the IVC made the dissection of the main artery more difficult, and longer THC was observed.
We did not register a statistical significance between the three surgeons. Larcher et al. [21] indicated that RAPN outcomes might be affected by surgeon experience by shortening WIT and lowering the complication rate. The inhomogeneous surgical experience among the surgical team members and the small sample size caused us to evaluate the surgeons as an independent variable, instead of surgeon’s expertise, and that may have biased our results. Intraoperative bleeding rate was low during RHC and correlated with longer THC as more time was needed to control the bleeding before controlling the renal hilum.
Some patient characteristics and comorbidities were not recorded due to the retrospective design of this study. The study was not blinded because SVR requires a trained kidney surgeon to identify the specific steps of the procedure and no interobserver validation of pattern assignment was attempted. The vascular patterns identified in our study are valuable for cases when clamping of the main artery is chosen; for selective clamping, different intrarenal anatomical patterns should be considered. Despite these limitations, our results can be used to optimise preoperative surgical planning for RAPN and provide a basis for developing a hilum complexity score in the future.
Conclusion
THC represents a relatively short part of total console time during RAPN. Previous renal surgery and a complex vascular pattern with artery bifurcation behind IVC on the right side and more than one main renal artery on the left side can lead to longer THC. A detailed understanding of renal vascular patterns can provide patient-specific surgical planning and optimise surgical strategies for RAPN.