Impact of Losartan on Portal Hypertension and Liver Cirrhosis: A Systematic Review
Deepti Avasthi, Nicholas Zerilli, Fahad Shaikh, Taimoor Jamil, Daniyal Ishtiaq, Salil Avasthi

TL;DR
This study reviews evidence on losartan's effectiveness in reducing portal pressure and liver fibrosis in patients with cirrhosis and portal hypertension.
Contribution
The study provides a systematic review and meta-analysis of losartan's impact on portal hypertension compared to propranolol.
Findings
Losartan significantly reduced wedged hepatic venous pressure compared to propranolol.
Losartan affected mean arterial pressure, renal function, and hepatic fibrosis.
Losartan may offer benefits in treating both hemodynamic and structural aspects of liver cirrhosis.
Abstract
Portal hypertension, a complication of chronic liver disease, results from an elevated pressure gradient between the portal vein and the inferior vena cava. While non-selective beta-blockers are established for reducing portal pressure, the efficacy of losartan, an angiotensin II receptor blocker, remains debated. This study evaluated losartan's impact on portal pressure and liver fibrosis in patients with cirrhosis and portal hypertension. The goal of this meta-analysis was to appraise evidence on the role of losartan in reducing portal pressure and associated clinical outcomes in cirrhotic patients with portal hypertension. A comprehensive literature search was conducted in PubMed, Cochrane Library, Medline, and Web of Science. All the research and literature review were conducted from August 20th, 2024, through August 31st, 2024 (within one month of the paper's submission). The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
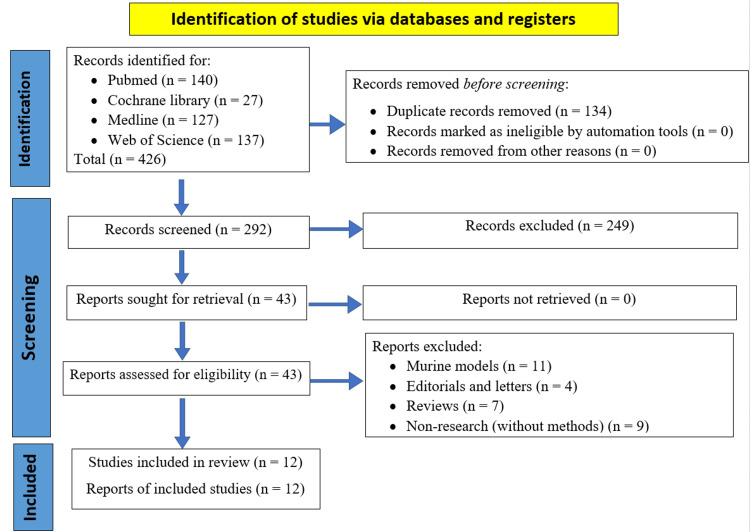 Figure 1
Figure 1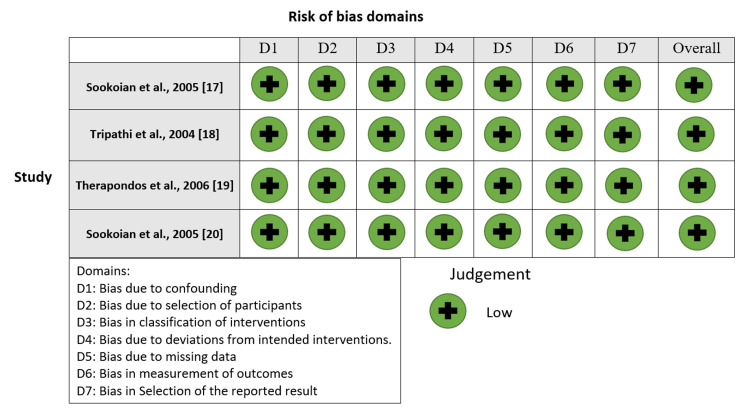 Figure 2
Figure 2 Figure 3
Figure 3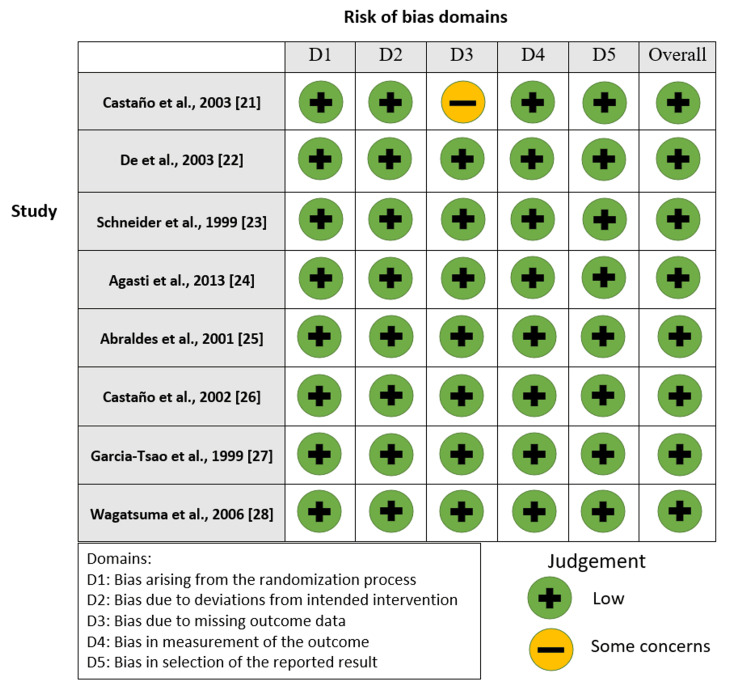 Figure 4
Figure 4 Figure 5
Figure 5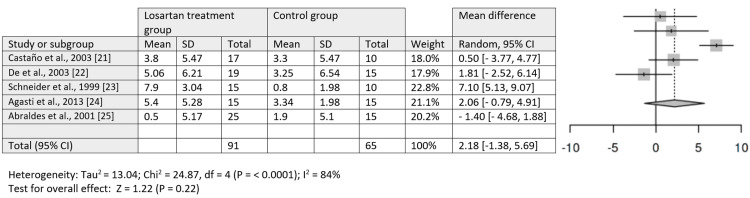 Figure 6
Figure 6 Figure 7
Figure 7 Figure 8
Figure 8| Query | Search Details | Results |
| #1 AND #2 | ("losartan"[MeSH Terms] OR "losartan"[All Fields] OR "losartan s"[All Fields] OR "losartane"[All Fields] OR "angiotensin II receptor blocker"[All Fields] OR "ARB"[All Fields]) AND ("portal hypertension"[All Fields] OR "liver cirrhosis"[All Fields] OR "hepatic fibrosis"[All Fields]) | 140 |
| ("portal hypertension" OR "liver cirrhosis" OR "hepatic fibrosis") | "portal hypertension"[All Fields] OR "liver cirrhosis"[All Fields] OR "hepatic fibrosis"[All Fields] | 142,986 |
| (losartan OR "angiotensin II receptor blocker" OR ARB) | "losartan"[MeSH Terms] OR "losartan"[All Fields] OR "losartan s"[All Fields] OR "losartane"[All Fields] OR "angiotensin II receptor blocker"[All Fields] OR "ARB"[All Fields] | 19,948 |
| Database | Search Strings | Results |
| Cochrane Library | (losartan OR "angiotensin II receptor blocker" OR ARB) AND ("portal hypertension" OR "liver cirrhosis" OR "hepatic fibrosis") | 27 |
| Medline | (losartan OR "angiotensin II receptor blocker" OR ARB) AND ("portal hypertension" OR "liver cirrhosis" OR "hepatic fibrosis") | 123 |
| Web of Science | (losartan OR "angiotensin II receptor blocker" OR ARB) AND ("portal hypertension" OR "liver cirrhosis" OR "hepatic fibrosis") | 137 |
| Study | Study design | Study settings | Sample characteristics | Mean age/age range | Sample size | Intervention | Comparator | Study purpose | Outcome measures | Findings |
| Abraldes et al., 2001 [ | Randomized controlled trial | Spain | Patients with cirrhosis who had bled from esophageal varices | 18-75 years | 40 | Losartan (6.25 mg-50 mg)/day | Propranolol (20 mg-160 mg) twice daily | To compare the hemodynamic and renal effects of losartan vs. propranolol in portal hypertensive patients with cirrhosis treated after a variceal bleeding episode | HVPG, systemic hemodynamics, renal function, and vasoactive factors | Losartan did not significantly reduce HVPG but decreased MAP and GFR in Child B patients. Propranolol reduced HVPG and cardiac output but did not modify MAP or renal function. |
| Agasti et al., (2013) [ | Randomized controlled trial | India | Patients with Child-Pugh B cirrhosis and large varices | 30-60 years | 30 | Losartan (12.5 mg once daily). After three days, 25 mg daily | Propranolol (40 mg daily). 20 mg increase after every three days | To compare the efficacy of losartan with propranolol on portal hypertension in patients with decompensated chronic liver disease | HVPG, WHVP, MABP, FHVP | Losartan and propranolol were equally effective in reducing portal pressure. Both groups had 40% responders. WHVP and HVPG reduction was greater in the losartan group, but no significant difference was observed between the two groups. |
| Castaño et al. (2003) [ | Randomized controlled trial | Argentina | Patients with cirrhosis and endoscopically proven esophageal varices and permeability of portal vein. | 18-75 years | 27 | Losartan (25 mg daily) | Propranolol | To compare the effectiveness of losartan versus propranolol in the treatment of portal hypertension. | Heart rate, cardiac output, and hepatic portal venous gradient. | Administration of losartan is effective in lowering portal pressure in patients with compensated cirrhosis, especially those with severe portal hypertension. |
| De et al. (2003) [ | Randomized controlled trial | India | Individuals with cirrhosis and esophageal varices | Age range: 15-65 years | 39 | Losartan (25 mg once daily) | Propranolol (40 mg twice a day) | To evaluate the effect of losartan on portal pressure after 14 days and compare it with propranolol | HVPG reduction | Losartan showed higher response rates (78.94%) than propranolol (45%). Losartan was more effective in non-ascitic and alcohol-abusing cirrhotic patients. |
| García–Tsao (1999) [ | Prospective | Germany | Patients with cirrhosis | Not specified | 70 | Losartan (25 mg daily oral) | No treatment | To evaluate the effect of losartan on portal pressure (HVPG) | HVPG, blood pressure, heart rate, body weight, liver and kidney function | Losartan significantly decreased HVPG in both severe (46.8%) and moderate (44.1%) portal hypertension. No significant changes in controls. Slight decrease in MABP. |
| Castaño et al. (2002) [ | Randomized trial | Argentina | Cirrhotic patients with portal hypertension | Not provided | 18 | Losartan (25 mg/day for 12 weeks) | Propranolol | To compare the effects of losartan vs. propranolol on HVPG in cirrhotic patients with portal hypertension | HVPG, MAP, cardiac output, portal blood flow, SVR, heart rate | Losartan led to a decrease in HVPG and SVR. There was no significant change in MAP. Propranolol showed a significant decrease in HVPG. |
| Schneider et al. (1999) [ | Randomized controlled trial | Germany | Cirrhotic patients with portal hypertension | Not specified | 30 | Losartan (25 mg daily for 1 week) | No treatment | To evaluate the effect of losartan on portal pressure in cirrhosis | HVPG, blood pressure, heart rate, body weight, liver and kidney function | Significant decrease in HVPG in losartan-treated patients with severe and moderate portal hypertension. No significant change in controls. There is a slight but significant decrease in mean arterial blood pressure. |
| Sookoian et al. (2005) [ | Non-randomized longitudinal study | Argentina | Patients with cirrhosis and portal hypertension | 18-75 years | 23 | Losartan, a dose of 25 mg daily | None | To investigate the relationship between genetic polymorphisms of the renin-angiotensin system and the effects of losartan on portal and systemic hemodynamics in patients with cirrhosis and portal hypertension. | Hepatic portal venous gradient, wedged hepatic venous pressure, free hepatic venous pressure. | A significant relationship exists between AT1R A1166C polymorphisms and the therapeutic response to losartan. |
| Sookoian et al. (2005) [ | Non-randomized controlled design | Argentina | 14 patients with chronic hepatitis C non-responders | 49.6 ± 13 years | 14 | Losartan (50 mg/d for 6 months) | A control group of untreated patients | To evaluate the safety and efficacy of losartan on hepatic fibrosis in chronic hepatitis C patients | Changes in fibrosis stage and blood pressure | Significant decrease in fibrosis stage in losartan group (decrease of 0.5 ± 1.3) compared to controls (increase of 0.89 ± 1.27; p < 0.03) |
| Therapondos et al. (2006) [ | Non-randomized experimental study | Canada | 10 post-TIPS ascites-free patients with cirrhosis (9 male patients, 1 female patient) | 52.2 ± 3.2 years | 10 | Single oral low-dose losartan (7.5 mg) | None | To investigate the role of posture in sodium retention in post-TIPS ascites-free patients and to study the effect of losartan on sodium handling. | Sodium excretion, PTRNa, plasma renin, angiotensin II, aldosterone levels | Losartan blunted PTRNa (supine 69.7% to 63.9%, p < 0.01; erect 81.1% to 73.8%, p < 0.01), but sodium retention remained. |
| Tripathi et al. (2004) [ | Non-randomized controlled design | United Kingdom | 12 patients with parasitic cirrhosis | 53.8 ± 3.3 years | 12 | Losartan (daily administration of 25 mg) | None | To investigate the systemic and portal hemodynamics and tolerability after chronic administration of losartan. | Hepatic portal venous gradient, WHVP, MAP. | Chronic administration of low-dose losartan does not lead to a significant reduction in the portal pressure gradient. |
| Wagatsuma et al. (2006) [ | Randomized experimental study | Japan | 16 patients with portal hypertensive gastropathy | Not specified | 16 | Losartan (daily administration of 25 mg or 50 mg dose) | 50 mg losartan compared to 25 mg. | To evaluate the efficacy of losartan in the treatment of portal hypertensive gastropathy. | Mean portal vein blood flow and congestion index. | Losartan was found to be effective in the treatment of portal hypertensive gastropathy. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Liver Disease Diagnosis and Treatment · Cardiovascular, Neuropeptides, and Oxidative Stress Research
Introduction and background
Portal hypertension is a serious complication of chronic liver diseases that can lead to life-threatening conditions like variceal bleeding and ascites. It arises from an increased pressure gradient between the portal vein and the inferior vena cava, often due to elevated intrahepatic vascular resistance and vasodilation of splanchnic blood vessels [1]. This condition can cause liver distortions, secondary fibrosis, and elevated portal blood pressure, particularly in cirrhosis [2]. The pathogenesis of liver cirrhosis is strongly associated with cardiovascular morbidity and shares a common pathologic pathway [3].
Current treatment primarily involves non-selective beta-blockers to reduce portal pressure [4]. Non-selective beta-blockers reduce portal pressures through both beta-1 receptor blockade and beta-2 receptor blockade. Beta-1 blockade is due to decreases in the following: pulse rate, cardiac output, portal venous flow, portal venous pressure, and the gradient between portal venous pressure and free hepatic venous pressure [5]. Beta-2 blockade results in unopposed alpha-1 receptor activation, resulting in splanchnic vasoconstriction [6].
Although non-selective beta-blockers are the first-line treatment, not all patients have optimal hepatic venous pressure gradient (HVPG) response (a decrease of more than 20% of HVPG from baseline or less than 12 mm Hg) to treatment. In a meta-analysis by Turco et al., cirrhotic patients without ascites showed that roughly 50% of patients had optimal HVPG decreases, and 42% of cirrhotic patients with ascites had optimal HVPG decreases [7]. Optimal HVPG reduction is necessary for cirrhotic patients to prevent complications of cirrhosis and to prevent early mortality. In a meta-analysis by Abraldes et al., results of a multivariate analysis showed that being a non-responder was independently associated with the risk of developing variceal rebleeding, ascites, spontaneous bacterial peritonitis, and lower survival [8].
Given the need for optimal HVPG reduction, other therapeutic options are in need of either replacing non-selective beta-blockers (NSBB) or being an addition to NSBB. The renin-angiotensin system presents another therapeutic target, with angiotensin II receptor blockers (ARBs) like losartan showing promise in experimental studies [9,10]. Research has investigated losartan's effects on portal pressure and clinical outcomes in cirrhotic patients, revealing mixed results regarding its impact on HVPG, which is the gold-standard measure of the severity of portal hypertension. This variation was likely due to the variations in patient demographics and study designs.
Angiotensin II receptor blocker significantly influences the pathogenesis of hepatic fibrosis, vasoconstriction within the liver sinusoids, and sodium balance in portal hypertension [11]. However, angiotensin receptor blockers can cause complications such as hypotension and renal impairment [12]. The pathogenesis of fibrosis may be reduced by losartan because it could potentially inhibit the angiotensin II receptors and offer a new treatment opportunity for liver cirrhosis.
There has been one other meta-analysis/systematic review completed on the comparison of propranolol and losartan regarding their impact on HVPG [13]. This review found that losartan is equivalent to propranolol in lowering HVPG with a mean HVPG difference of -0.59 (CI: -2.73 to -3.04). Losartan usage was also associated with a statistically significant drop in MAP (mean arterial blood pressure), with the difference of 0.53 (CI: -2.47 to -3.54). Losartan was also shown to be non-inferior to propranolol in preventing portal hypertensive bleeding [RR: 2.02 (CI: 0.38 to 10.89)]. Finally, propranolol was found to have a statistically significant heart rate decrease of 18.62 (CI: 10.10 to 27.74). Although, this study did analyze the significance of propranolol versus losartan regarding wedged hepatic venous pressure (WHVP) [13].
We believe that there is a lack of high-quality evidence regarding the influence of losartan on liver fibrosis and the complications of portal hypertension. This study aims to evaluate losartan's effect on HVPG, systemic hemodynamics, renal function, and clinical events like variceal bleeding and ascites, through a systematic review and meta-analysis of the existing literature, while also assessing the management of risks associated with its use.
Disclaimer
It should be noted that this article was pre-printed on September 27, 2024, on the medRxiv pre-print server.
Review
Research approach
The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [14].
Identification and Selection of Studies
Literature was sourced from PubMed, Cochrane Library, Medline, and Web of Science focusing on losartan's effect on portal hypertension. Figure 1 displays the PRISMA flow diagram that shows how studies were identified, screened, and included in our meta-analysis.
PRISMA flow diagramPRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Search Strategy
Keywords used included losartan, ARB, portal hypertension, liver cirrhosis, and hepatic fibrosis (Tables 1, 2).
Study Selection
Retrieved results were managed using Zotero version 6.0.36 (Corporation for Digital Scholarship, Vienna, VA), which helped exclude retracted records and merge duplicates.
Eligibility Criteria
Research included in the study adhered to modified Population, Intervention, Comparison, Outcomes, Study Design (PICOS) criteria [15]:
Population (P): Patients with portal hypertension.
Intervention (I): Losartan.
Comparison (C): Propranolol
Primary Outcomes (O): Portal pressure, response rates, disease progression.
Study Design (S): Quantitative, qualitative, and mixed methods.
Inclusion Criteria
Peer-reviewed original research articles published in English (or translatable) on losartan's effect on portal hypertension.
Exclusion Criteria
Excluded were non-research articles, study protocols, reviews, meta-analyses, opinion pieces, conference abstracts, and editorials.
Methodological Quality Assessment: The Risk of Bias
The risk of bias was evaluated using the Robvis 2.0 tool and the Risk of Bias in Non-randomized Studies (ROBINS) [16].
The review of literature was conducted from August 20th, 2024, through August 31st, 2024.
Figures 2-5 show the risk-of-bias visualization tool (Robvis 2.0) and the ROBINS with the intervention assessment results.
Risk-of-bias traffic light plotTraffic light plot of the Risk of Bias in Non-randomized Studies (ROBINS) with the intervention assessment results [17-20].
Summary plot of the risk of biasRisk of Bias in Non-randomized Studies (ROBINS) with the intervention assessment results [16-19].
Risk-of-bias traffic light plot Traffic light plot of the risk-of-bias visualization tool assessment results [21-28].
Summary plot of the risk of biasSummary plot of the risk-of-bias visualization tool assessment results [20-27].
Data Extraction
Data were systematically extracted by one reviewer independently and entered manually into an Excel sheet using Microsoft Excel 2019 (Microsoft Corporation, Redmond, WA), including study ID, design, settings, sample characteristics, mean age or age range, sample size, intervention details, purpose, outcome measures, and findings.
Data Analysis
The extracted qualitative data were analyzed and reported according to the predominant themes. On the other hand, quantitative data were analyzed using Review Manager 5.4.1 (Cochrane Collaboration, London, UK). An intervention review starting from the full review stage was used [29]. In addition, continuous data types were used, applying inverse variance statistical, random effects analysis model, and mean difference effect measure.
Study Selection
The literature search yielded 431 records, with 134 duplicates removed. Following the title and abstract screening, 255 records were excluded, leaving 42 articles for retrieval. Ultimately, 12 studies met the eligibility criteria, as illustrated in Figure 1.
Thematic analysis of outcomes and study characteristics
The summarization of studies and analysis of outcomes can be found in Table 3.
Changes in HVPG and WHVP
Research indicated varying effects of losartan on HVPG, WHVP, and mean arterial pressure (MAP). The study conducted by Tripathi et al. showed no significant change in HVPG after four weeks of losartan treatment, with a reduction from 15.4 ± 1.5 to 13.6 ± 1.6 mmHg (p = 0.1). There was a significant reduction in WHVP, falling from 20.3 ± 1.8 to 17.3 ± 1.8 mmHg (p < 0.05) and a significant decrease in MAP, from 97 ± 3.0 mmHg to 89 ± 4.0 mmHg (p = 0.02) [18]. Another study found a significant reduction in HVPG in patients with severe portal hypertension, dropping from 24.8 ± 3.6 to 13.1 ± 4.1 mmHg (p < 0.001), compared to the control group with a minor decline from 23.9 ± 4.1 to 23.1 ± 4.2 mmHg and WHVP reduction from 22.1 ± 2.6 to 14.1 ± 2.9 mmHg (p < 0.001) in patients with moderate hypertension. The control group demonstrated a smaller reduction from 22.0 ± 2.2 to 21.4 ± 2.6 mmHg [23].
In other studies, losartan reduced HVPG in moderate cases by 46.8%, from 17.9 ± 1.4 to 10.0 ± 2.7 mmHg [26]. Comparatively, losartan reduced HVPG from 15.6 ± 4.2 mmHg to 11.8 ± 3.5 mmHg, while propranolol reduced it from 16.4 ± 4.1 to 13.1 ± 3.6 mmHg, showing a more significant reduction of -10% ± 11% (p = 0.003) compared to losartan's non-significant change of -2% ± 12% [21]. The study conducted by De et al. showed that losartan decreased HVPG from 19.21 ± 3.82 to 14.15 ± 4.91 mmHg, while propranolol reduced it from 18.7 ± 3.77 to 15.45 ± 5.35 mmHg. Losartan also reduced WHVP from 32.42 ± 6.61 to 28.31 ± 5.09 mmHg, and propranolol lowered it from 34.55 ± 5.41 to 32.75 ± 8.13 mmHg [22].
Losartan significantly decreased MAP from 97 ± 3.0 to 89 ± 4.0 mmHg (p = 0.02) and from 90.9 ± 5.5 to 87.4 ± 4.6 mmHg in two other studies who compared its effect with propranolol. A reduction in systolic arterial pressure from 134 ± 22.7 to 124 ± 18.1 mmHg was noted, along with minor increases in diastolic pressure and MAP. In comparison, propranolol led to significantly lower HVPG and MAP, with HVPG remaining higher in the losartan group. Losartan reduced the heart rate from 79.6 ± 1.5 to 78.1 ± 2.5 BPM, while propranolol led to a larger decrease from 80.8 ± 6.2 to 68.3 ± 5.5 BPM [17,24].
Patient Demographics and Genetic Factors
The study conducted by Sookoian et al., on genetic polymorphisms of the angiotensin II type 1 receptor gene, provided some insights on the variable effect of losartan in different genotypes. According to this study, losartan significantly decreased HVPG in portal hypertension patients with genotype AA from 15.7 ± 4.3 to 10.6 ± 3.4, in contrast to patients with genotypes AC and CC, who showed minor reductions from 15.9 ± 1.6 to 15.4 ± 2.8. A similar trend was observed in WHVP, where genotype AA patients showed significant improvement from 26.0 ± 4.4 to 21.9 ± 6.1 mmHg, while no significant changes were noted in patients with AC and CC genotypes [17].
Impact on Renal Markers and Sodium Handling
The renal function markers like glomerular filtration rate (GFR), blood urea nitrogen, and creatinine were not affected by propranolol. However, losartan significantly decreased GFR in Child B patients, particularly those with reduced MAP and systemic vascular resistance. Additionally, there were no significant changes in GFR during diuretic use [25]. The effect of losartan on sodium handling in kidneys was also noted by Tripathi et al. during their study on HVPG (quoted above). According to their findings, there was no significant change in creatinine clearance after four weeks of losartan, and it was recorded that losartan caused reduction of sodium excretion from 154 ± 61 mmol/day to 122 ± 36 mmol/day [18]. Similar findings were recorded by another study in which losartan administration resulted in decreased proximal tubular reabsorption of sodium in both supine and erect positions, with significant decreases noted in both positions (supine: from 69.7 ± 3.1% to 63.9 ± 3.9 %, p = 0.01; erect: from 81.1 ± 1.8% to 73.8 ± 2.4%, p = 0.01) [19].
Antifibrotic Effects
Losartan led to a decrease in the fibrosis stage, with the treated group showing a reduction of 0.64 ± 1.3 compared to an increase of 0.89 ± 1.27 in the control group. The reduction in fibrosis was further evidenced by improvements in seven out of 14 treated patients, compared to only one out of nine in the control group. Sub-endothelial fibrosis in lobular areas significantly decreased from a baseline of 2.48 ± 1.04 to 1.00 ± 0.53 after losartan treatment, while no significant changes were observed in the control group [20].
Management of Portal Hypertension-Related Complications
According to a study conducted by Wagatsuma et al., portal hypertensive gastropathy improved in nine out of 16 patients, with an efficacy rate of 56% after losartan administration. Higher efficacy was observed with a 50 mg dose of losartan (83%) compared to a 25 mg dose (40%) [28].
Safety and Adverse Effects
Losartan and propranolol were well-tolerated by over 90% of patients, though some studies reported adverse events. Transient hypotension was commonly seen after the first dose of losartan, with no recurrence during continued treatment. Mild orthostatic hypotension, gastrointestinal bleeding, and encephalopathy were also noted, with some patients developing these conditions after using either losartan or propranolol. Severe side effects included rebleeding associated with losartan, though none of the adverse events were fatal, and treatment withdrawal was necessary in only one case. In patients with severe portal hypertension, losartan also caused nausea and dizziness. The findings from the study from Abraldes JG et al. show that the overall incidence of adverse events was similar for losartan (28%) and propranolol (27%) [25].
Meta-Analysis Findings
The meta-analysis included five studies (study numbers [20-24]) that reported quantitative data on HVPG changes. The analysis indicated no statistically significant difference in HVPG change between the losartan treatment group and the control group (p = 0.22). High heterogeneity was noted among the included studies, with an I² of 84%, likely due to variations in sample sizes and study designs. Figures 6, 7 illustrate forest plot data of HVPG comparisons and WHVP for losartan treatment groups and control groups.
Forest plot of hepatic venous pressure gradient comparisonHepatic venous pressure gradient comparison between the losartan treatment group and the control group [21-25].
Forest plot of WHVP comparison WHVP comparison between the losartan treatment group and the control group [22-24].WHVP, wedged hepatic venous pressure.
Overall, this structured analysis underscores losartan's potential efficacy in managing portal hypertension, with specific emphasis on its effects on HVPG, WHVP, and MAP, as well as its comparative efficacy against propranolol. The findings also highlight the importance of patient demographics, particularly genetic factors, and renal function in treatment outcomes.
Figure 8 illustrates the certainty of evidence using the GRADE method [30].
Certainty of evidence for meta-analysisHVPG, hepatic venous pressure gradient; WHVP, wedged hepatic venous pressure; RCT, randomized controlled trial.
Discussion
This study assessed the effects of losartan on portal hypertension. The findings of this systematic review and meta-analysis indicate that managing the condition is challenging. The variable results in terms of the effectiveness of losartan for lowering HVPG across studies relate directly to the variability in the severity and baseline characteristics of portal hypertension. Some studies showed marked reductions in HVPG, while others showed negligible changes, resulting in no statistically significant overall change in HVPG in the meta-analysis. These differences could be attributed to factors such as the variation in liver disease type and extent, initial portal hypertension severity, and differences in treatment duration and dosages [31].
Further investigation into losartan's hemodynamic effects revealed changes in WHVP. However, the impact was not statistically significant, highlighting that portal hypertension's pathophysiology is multifactorial, with various mechanisms influencing the initial improvements. Most studies noted decreases in the MAP, a potential concern for cirrhotic patients with fragile hemodynamic conditions. Thus, losartan therapy must be carefully adjusted to avoid systemic hypotension.
Losartan also showed therapeutic potential in mitigating liver disease-related fibrosis, aligning with preclinical findings that suggest that losartan could inhibit hepatic stellate cell activation [32]. This variability in effect corresponds with previous studies on the renin-angiotensin system in portal hypertension, linking it to complex pathways, high intrahepatic pressure, and splanchnic vasodilation [33].
Genetic factors, such as the AT1R A1166C polymorphism, may influence losartan effectiveness, suggesting personalized treatment options for portal hypertension [34]. The significant plasticity of hepatic circulation leads to compensatory reactions that might minimize losartan's initial hemodynamic effects [35], which does not guarantee long-term outcomes.
Dose optimization remains inconclusive, as higher doses reduce portal pressure but increase the risk of systemic hypotension. The timing of intervention is also crucial, with early intervention potentially offering benefits before disease progression.
The safety profile of losartan showed good tolerability, though episodes of hypotension, reduced renal function, and gastrointestinal hemorrhage were reported. These findings correlate with the renin-angiotensin system inhibition effects in cirrhotic patients emphasizing careful patient evaluation and monitoring [36,37].
Overall, the variability in response underscores the need to consider multiple factors in managing portal hypertension, including patient characteristics, disease etiology and severity, and genetic predispositions. Losartan's antifibrotic effects point to potential therapeutic approaches in the disease's early stages. Combination therapy targeting hemodynamic and fibrotic features might enhance treatment outcomes. However, safety concerns necessitate meticulous patient selection, especially for those with unstable hemodynamics. The findings of our study build upon and confirm the broader findings of Tandon et al. regarding the effects of angiotensin-converting enzyme (ACE) inhibitors and ARBs on portal hypertension in liver cirrhosis [38].
Further studies should explore the factors affecting losartan response, optimal dosing, and intervention timing in liver disorders. Future research should include large randomized controlled trials (RCTs) with comparisons of losartan, propranolol, and combination of both losartan and propranolol treatments.
Limitations of the study
The heterogeneity among included studies regarding patient populations and dosing impacts the generalizability of the findings. In addition, the variability in disease etiology, severity, and baseline portal pressures across studies limit direct comparisons through meta-analyses. Further research is needed to ensure accurate interpretation of data to guide clinical decision making.
Moreover, the lack of data on specific subgroups, such as patients with different stages of liver disease or various comorbidities, limits the generalizability of the findings of losartan's efficacy to all subgroups.
Conclusions
This study highlights losartan's potential efficacy in treating portal hypertension. Its antifibrotic properties and ability to reduce portal pressure highlight its potential to address both hemodynamic and structural aspects of the disease, especially in the early stage of liver cirrhosis.
Losartan’s effects on MAP and natriuresis could also be relevant in managing associated cardiomyopathies in cirrhotic patients. Further research is needed to fully explore losartan's comprehensive therapeutic benefits in this complex patient population, particularly focusing on its dual role in liver and cardiovascular health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pathophysiology and management of liver cirrhosis: From portal hypertension to acute-on-chronic liver failure Front Med (Lausanne) Jagdish RK Roy A Kumar K 10600731020233739691810.3389/fmed.2023.1060073 PMC 10311004 · doi ↗ · pubmed ↗
- 2Correlation of pressure gradient in three hepatic veins with portal pressure gradient World J Clin Cases Wang HY Song QK Yue ZD 446044691020223566309410.12998/wjcc.v 10.i 14.4460 PMC 9125293 · doi ↗ · pubmed ↗
- 3Cirrhotic cardiomyopathy: Pathogenesis and clinical relevance Nat Rev Gastroenterol Hepatol Wiese S Hove JD Bendtsen F Møller S 1771861120142421734710.1038/nrgastro.2013.210 · doi ↗ · pubmed ↗
- 4Cirrhotic portal hypertension: From pathophysiology to novel therapeutics World J Gastroenterol Gunarathne LS Rajapaksha H Shackel N Angus PW Herath CB 611161402620203317778910.3748/wjg.v 26.i 40.6111 PMC 7596642 · doi ↗ · pubmed ↗
- 5Effects of propranolol on portal hemodynamics in patients with chronic liver disease Am J Gastroenterol Ohnishi K Nakayama T Saito M 132135801985 https://pubmed.ncbi.nlm.nih.gov/3881933/3881933 · pubmed ↗
- 6Effects of alpha-adrenergic stimulation and beta-adrenergic blockade on azygos blood flow and splanchnic haemodynamics in patients with cirrhosis J Hepatol Mastai R Bosch J Navasa M Kravetz D Bruix J Viola C Rodés J 717941987303306110.1016/s 0168-8278(87)80012-0 · doi ↗ · pubmed ↗
- 7Lowering portal pressure improves outcomes of patients with cirrhosis, with or without ascites: A meta-analysis Clin Gastroenterol Hepatol Turco L Villanueva C La Mura V 3133271820203117601310.1016/j.cgh.2019.05.050 · doi ↗ · pubmed ↗
- 8Hemodynamic response to pharmacological treatment of portal hypertension and long-term prognosis of cirrhosis Hepatology Abraldes JG Tarantino I Turnes J Garcia-Pagan JC Rodés J Bosch J 9029083720031266898510.1053/jhep.2003.50133 · doi ↗ · pubmed ↗