Impact of Calcified Plaque Distribution on Symmetrical Stent Expansion After Intravascular Lithotripsy
Takeshi Yamada, Norimasa Taniguchi, Tetsuya Hata, Shunsuke Nakajima, Shiori Kawakami, Akihiko Takahashi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
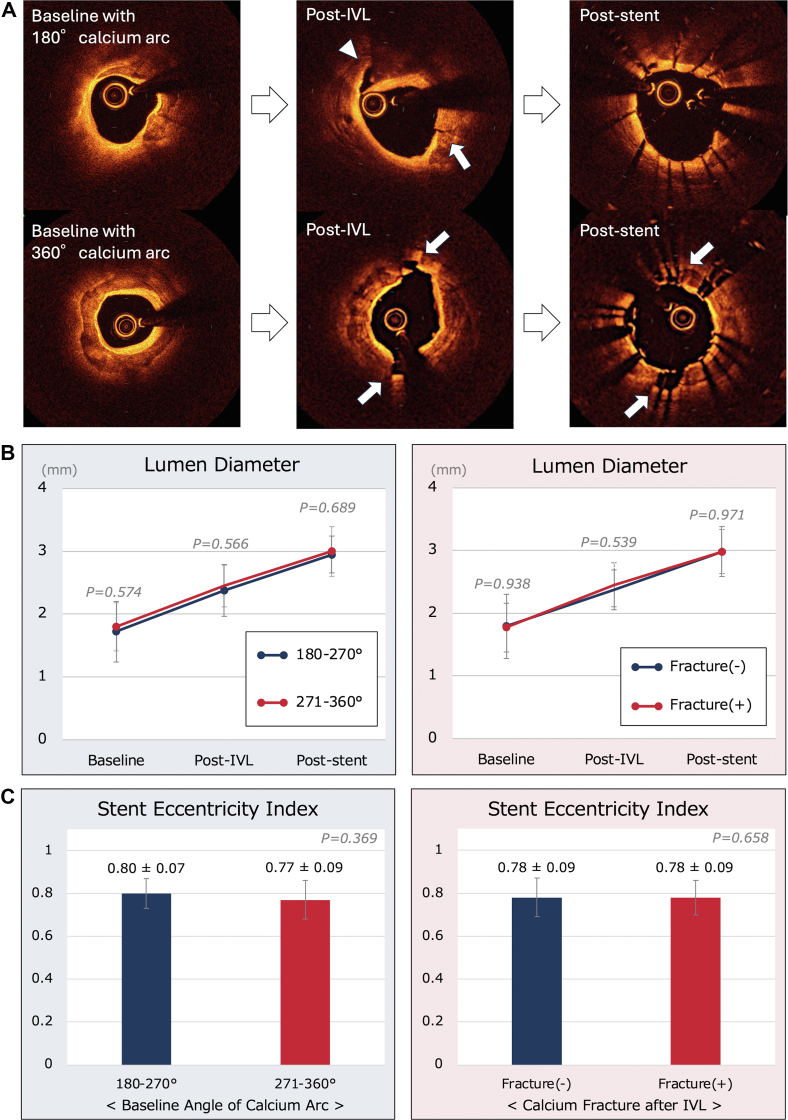 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Coronary Interventions and Diagnostics · Vascular Procedures and Complications
Introduction
The goal of stent implantation in percutaneous coronary intervention is to achieve a large stent lumen area with symmetrical, round-shaped expansion to minimize adverse events and improve clinical outcomes.1 Recently, intravascular lithotripsy (IVL) has emerged as a promising alternative to existing devices for treating calcified coronary arteries, modifying calcifications, and facilitating sufficient stent expansion.2 However, residual calcium plaques may still affect the subsequent stent expansion. This study aimed to investigate the impact of the baseline calcium angle and calcium fractures created by IVL on stent expansion with cross-sectional roundness in patients with calcified coronary lesions assessed using optical coherence tomography (OCT).
Methods
This single-center retrospective study included 49 consecutive patients who underwent OCT-guided percutaneous coronary intervention with IVL from June 2022 to April 2024. Baseline and final OCT findings were obtained for all patients; images were taken immediately after IVL in 47 (94.9%) patients. OCT images were obtained for every 0.2 mm using a Dragonfly or Dragonfly OpStar catheter (Abbott Medical Japan) and were analyzed using Ultreon console version 2.0 (Abbott Medical Japan). In cases requiring rotational atherectomy, OCT images after atherectomy were assessed for baseline OCT findings. They were divided into 2 groups according to the maximum angle of calcium plaques in the maximum calcified segment among the target lesions observed on baseline OCT images: 180° to 270° and 271° to 360°. The lumen and vessel areas at baseline and after IVL, incidence of calcium fractures after IVL, stent area, and stent eccentricity index were evaluated.
Results
The mean patient age was 75.7 ± 9.9 years. The maximum calcium angle at baseline OCT was 180° to 270° in 12 patients and 271° to 360° in 37 patients. Rotational atherectomy was performed in 5 (10.2%) patients prior to IVL catheter crossing, and the IVL catheter was successfully delivered in all patients; the mean IVL balloon diameter was 3.19 ± 0.39 mm, and a mean number of 82.1 ± 28.2 IVL pulses were delivered. Coronary stents were implanted in all patients after IVL; the mean stent diameter was 3.21 ± 0.41 mm. Postdilation of the stents was performed in 35 patients (71.4%). There were no significant differences in those patients' background and procedural characteristics between 2 groups according to baseline calcium angle using the χ^2^ test or the unpaired t test.
Assessment of the baseline OCT images indicated a mean reference diameter of 3.37 ± 0.53 mm (3.48 ± 0.53 in 180°-270° calcium group vs 3.33 ± 0.53 in 271°-360° calcium group; P = .395). The mean calcium angle, calcium length, and calcium thickness were 311° ± 59° (225° ± 35° vs 339° ± 31°; P < .001), 19.6 ± 9.4 mm (16.5 ± 7.5 mm vs 20.6 ± 9.8 mm; P = .199), and 1.05 ± 0.24 mm (0.93 ± 0.28 mm vs 1.09 ± 0.21 mm; P = .033), respectively. Calcified nodules were detected in 7 patients (16.7% vs 13.5%; P = .786). Calcium fractures were observed on OCT images after IVL in 40 (81.6%) patients and was more frequently observed in the group with circumferential calcium (45.5% vs 94.4%; P = .001).
On baseline OCT images of the maximum calcified segment, the mean lumen diameter was 1.78 ± 0.40 mm (1.72 ± 0.48 mm vs 1.80 ± 0.38 mm; P = .574), and the mean stent diameter on final OCT images was 2.99 ± 0.37 mm (2.95 ± 0.29 mm vs 3.00 ± 0.40 mm; P = .689). In the overall cohort, the mean stent area and mean stent eccentricity index were 7.18 ± 1.82 mm^2^ and 0.78 ± 0.09, respectively, with no significant difference between the 2 groups (Figure 1). Analysis of the impact of calcium fractures detected by OCT after IVL on stent expansion and stent eccentricity index (n = 47) revealed no significant difference (Figure 1). No complications related to the IVL procedure, such as coronary perforation and slow-flow/no-reflow phenomenon, were detected.Figure 1Representative optical coherence tomography images, the changes in lumen diameter, and stent eccentricity index. (A) Optical coherence tomography images. In the case of eccentric calcium, a small calcium fracture (white arrow) and medial dissection at the edge of sheet calcification (white arrowhead) were observed after intravascular lithotripsy (IVL). In the case of full circumferential calcium, 2 wide fractures (white arrow) were observed after IVL. Stents are well-expanded in both cases. (B) Lumen diameter in the maximum calcified segment. No significant differences were found between the groups according to the baseline calcium angle or optical coherence tomography–detected calcium fractures after IVL. (C) Stent eccentricity index in the maximum calcified segment. There were no significant differences between the groups according to the baseline calcium angle or calcium fractures after IVL.
Discussion
In this study, calcium fractures detected using OCT were more likely to be observed in the group with circumferential calcium than in the group without. However, the final stent expansion and eccentricity were not related to the calcium fractures detected using OCT after IVL. These findings may be attributable to the following: (1) IVL causes microfractures in calcium that are invisible with the resolution of OCT, and (2) approximately half of the major calcium fractures cannot be detected by OCT because of the presence of guidewire artifacts or the poor penetration depth of OCT, as reported in the micro–computed tomography study of cadaver heart.3 Thus, stents deployed after IVL are considered to have favorably expanded, regardless of OCT-detected calcium fractures.
Conclusions
Coronary stents expanded favorably and concentrically without adverse events, irrespective of the baseline maximum calcium angle and the presence of OCT-detected calcium fractures after IVL.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hamana T.Kawamori H.Toba T.Predictors of target lesion revascularisation after drug-eluting stent implantation for calcified nodules: an optical coherence tomography study Euro Intervention 1922023 e 123e 13310.4244/EIJ-D-22-00836 PMC 1024072736876497 · doi ↗ · pubmed ↗
- 2Kereiakes D.J.Di Mario C.Riley R.F.Intravascular lithotripsy for treatment of calcified coronary lesions: patient-level pooled analysis of the disrupt CAD studies JACC Cardiovasc Interv 141220211337134810.1016/j.jcin.2021.04.01533939604 · doi ↗ · pubmed ↗
- 3Kawai K.Sato Y.Hokama J.Y.Histology, OCT, and micro-CT evaluation of coronary calcification treated with intravascular lithotripsy: atherosclerotic cadaver study JACC Cardiovasc Interv 161720232097210810.1016/j.jcin.2023.06.02137704295 · doi ↗ · pubmed ↗