The Flipping Suture Technique for Reduction of Chronic Incarcerated Bucket-Handle Meniscus Tears
Francesco Bosco, Alessandro Ghirri, Domenico Lewis Battaglia, Fortunato Giustra, Alessandro Massè, Ajay Thakur

TL;DR
This paper introduces a new surgical technique to treat chronic meniscal tears in the knee using a flipping suture followed by standard repair.
Contribution
A novel outside-in flipping suture technique is proposed for treating chronically incarcerated bucket-handle meniscus tears.
Findings
The flipping suture technique enables meniscal eversion for better repair outcomes.
The method is presented as a reproducible alternative to traditional inside-out techniques.
It is particularly useful when the posterior horn of the meniscus is involved.
Abstract
Meniscal tears are the most common and most treated injuries of the knee. In the recent past, meniscectomy was considered the treatment of choice for meniscal lesions. However, this practice is progressively being discontinued in favor of meniscal repair, which has shown high success rates. Several techniques are currently used individually or in association to treat bucket-handle meniscal tears. The inside-out technique has been considered the gold standard for this kind of lesion, especially if the posterior horn of the meniscus is involved. This article aims to describe a reproducible surgical technique for chronically incarcerated bucket handle meniscal tears that consist of an outside-in reduction suture for meniscal eversion, the “flipping suture”, followed by additional standard meniscal repair sutures.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
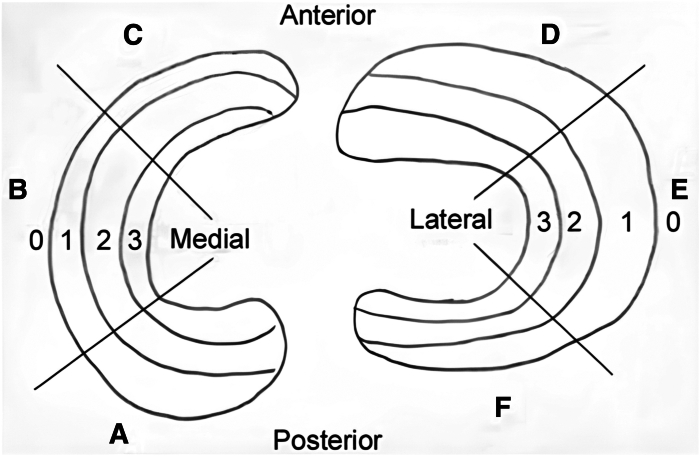 Figure 1
Figure 1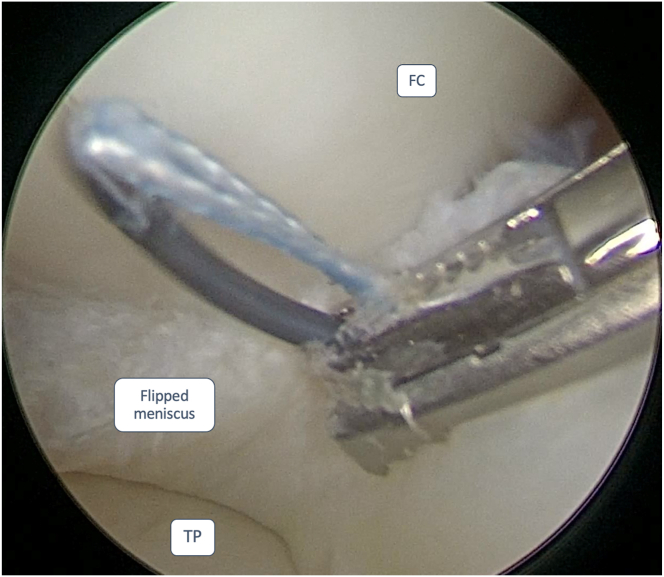 Figure 2
Figure 2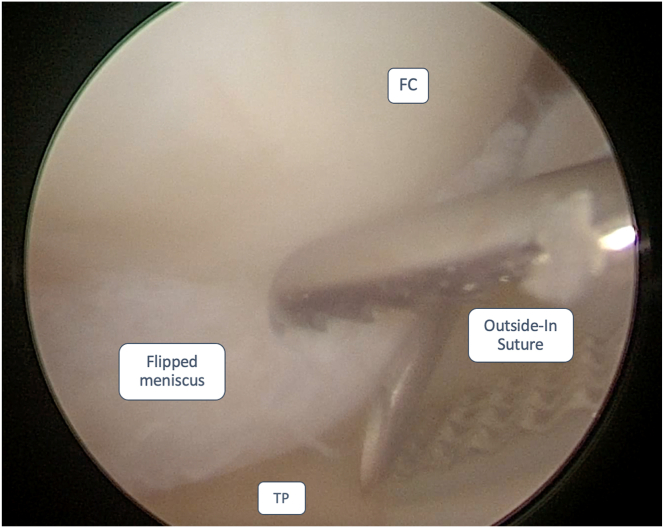 Figure 3
Figure 3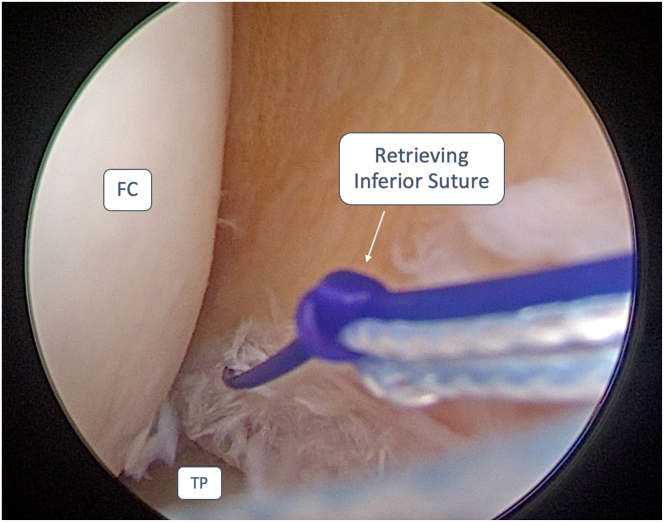 Figure 4
Figure 4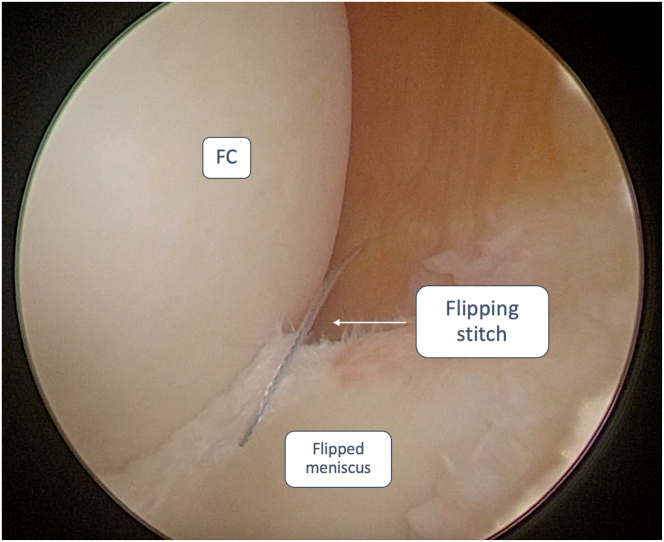 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Orthopedic Surgery and Rehabilitation · Total Knee Arthroplasty Outcomes
Meniscal tears are the most common and most treated injuries of the knee. The treatment of these lesions depends on the tear’s localization, which may be identified through Cooper’s classification (Fig 1).1 Recently, meniscectomy was considered the treatment of choice for meniscal lesions. However, this practice is progressively discontinued in favor of meniscal repair, which has shown success rates between 85% and 90%.2 Bucket-handle meniscal tears (BHMT) can be considered a displacement of longitudinal tears, which causes locking and pain in the knee due to migration in the intercondylar notch.3 Meniscal repair surgery consists of three different techniques: all-inside, inside-out, and outside-in. The first is the most adopted worldwide for its effectiveness and efficiency, aided by technological advancement supporting this procedure. The second and third are currently used for displaced BHMT or body and posterior horn tears, the latter being preferred for anterior horn lesions.4 BHMT has a higher overall failure rate, as opposed to simple tears. This trend increases in chronic incarcerated tears, for which the failure rate is estimated at 47%, rising to 80% in complex tears.5 In recent years, biological augmentation, in the setting of meniscal repair, has gained success among surgeons; bone marrow stimulation and microperforations, platelet-rich plasma, and stem cell therapy are now being extensively adopted to ensure a better healing process of the menisci and joint cartilage. Several surgical techniques have been proposed to help surgeons accomplish an effective meniscal repair.Fig 1. Cooper's Classification of meniscal tears: The medial meniscus is identified with letters (A) Posterior horn of the medial meniscus. (B) Body of the medial meniscus. (C) Anterior horn of the medial meniscus. The lateral meniscus is identified with letters D–F. (D) Anterior horn of the lateral meniscus. (E) Body of the lateral meniscus. (F) Posterior horn of the lateral meniscus. The four circumferential zones are 0 for the meniscal-capsular junction, 1 for the outer third, 2 for the middle third, and 3 for the inner third.
This article aims to describe a reproducible surgical technique for chronically incarcerated bucket handle meniscal tears. It consists of an outside-in reduction suture for meniscal eversion, followed by standard meniscal repair techniques.
Surgical Technique
The video illustrates the surgical technique in detail (Video 1).
Preoperative Assessment
The patient was evaluated preoperatively with clinical examination and standard knee x-rays. The patient experienced knee instability, stiffness, swelling, and pain in the affected compartment, locking, and inability to achieve full extension of the knee. Long leg radiographs should be considered if, upon clinical examination, a lower limb deformity is suspected. Magnetic resonance imaging (MRI) is mandatory for a complete preoperative assessment to assess the morphology of the tear and its complexity, possible associated lesions, such as cruciate ligament tears, ramp, or meniscal root lesions and chondral injuries.
Patient’s Positioning and Anesthesia
The procedure is conducted under spinal or general anesthesia. The patient is placed in a supine decubitus position with a pneumatic tourniquet applied around the proximal thigh of the affected limb. Side support is positioned at the distal third of the thigh as a pivot point for valgus stress maneuvers during the surgery. A side pad is also placed near the contralateral greater trochanter to enhance stability and reduce pelvic tilting during valgus strain. The leg is then left hanging over the edge of the operating table during the arthroscopic procedure. The affected limb may be positioned on a leg holder, removing the distal portion of the operating table if no associated procedures are needed on the patient.
Diagnostic Arthroscopy
A standard arthroscopic examination is performed through anterolateral (AL) and anteromedial (AM) portals. The patellofemoral joint is evaluated for abnormal patellar tracking or chondral damage. The central pivot is then thoroughly examined and palpated to ascertain its integrity and tension, as cruciate ligament tears are often associated with meniscal tears. The medial and lateral compartments are fully scouted for meniscal and root lesions and to assess cartilage joint degeneration (ICRS scale). Ramp lesions are examined through an anterior view from the medial compartment and a trans-notch view. An accessory posteromedial portal may be considered to assess possible ramp lesions. In case of a medial meniscus tear with low visibility of the medial compartment, the surgeon should feel a release of the medial collateral ligament through a pie-crust technique.6
Surgical Note—Step by Step
Once the bucket-handle fragment is identified, the surgeon carefully attempts its reduction using a probe or blunt trocar. If successful, the tear site is debrided with 4.5-mm shaver blades, followed by needling at the meniscal-capsular junction. The surgeon may then proceed with the meniscal repair technique of choice. Scar tissue around the displaced tear fragment may prevent reduction. Therefore, accurate rasping and debridement need to be performed before the reduction maneuver. This meticulous approach ensures the best possible outcome for the patient.
If the reduction is not successful, hence the necessity of meniscal-reduction suture techniques, the authors advise using an antegrade self-retrieving suture device (Scorpion Suture Passers; Arthrex, Naples, FL) and applying a suture at the base of the meniscus fragment (Fig 2). The aforementioned suture needs to be positioned at the base of the fragment, along the femoral condyle, where the bucket-handle tear is flipped in the intercondylar notch.Fig 2. Anterolateral portal view of a medial meniscus bucket-handle tear of a left knee. The surgeon is positioning a suture wire through an antegrade self-retrieving suture device, applying a suture at the base of the meniscus fragment. The patient was placed in a supine decubitus position. The leg was then left hanging over the edge of the operating table during the arthroscopic procedure. FC, femoral condyle; TP, tibial plateau.
An 18-gauge spinal needle is inserted at the meniscal-capsular junction, where the meniscal body is normally seated, to insert a nylon suture shuttle, which is then retrieved through the AM portal (Fig 3).Fig 3. Anteromedial portal view of a medial meniscus bucket-handle tear of a left knee. Outside-in technique suture shuttle positioning at the meniscal-capsular junction. The patient was placed in a supine decubitus position. The leg was then left hanging over the edge of the operating table during the arthroscopic procedure. FC, femoral condyle; TP, tibial plateau.
The “flipping-stitch” is achieved using an outside-in technique, retrieving the inferior suture end first (Fig 4), followed by the superior suture, using the suture shuttle previously inserted. Once both the suture ends are retrieved from the skin, the everted meniscal bucket-handle fragment is flipped, maintaining a constant tension on the threads and a gentle varus or valgus stress with a blunt trocar or probe (Fig 5). Once complete reduction of the fragment is achieved, maintain minimum tension during stressing maneuvers to avoid redisplacement of the fragment. The fragment is stabilized using all-inside or inside-out suturing techniques (FiberStitch or ZoneNavigator system with 0.9-mm SutureTape, Arthrex, respectively). Sutures can be configured in either vertical or horizontal mattress patterns to ensure adequate repair stability and anatomical fixation. When employing the outside-in technique, a vertical suture should be positioned at the terminal end of the tear on the anterior horn of the meniscus, followed by a second vertical suture placed on the posterior horn. These sutures are strategically placed to prevent the anterior and posterior propagation of the meniscal fragment (Table 1).Fig 4. Anterolateral portal view of a medial meniscus bucket-handle tear of a left knee. To obtain a “Flipping Stitch”, the inferior end of the suture wire is retrieved at the meniscal-capsular junction with an outside-in technique. This step is repeated for the superior end of the suture wire. The patient was placed in a supine decubitus position. The leg was then left hanging over the edge of the operating table during the arthroscopic procedure. FC, femoral condyle; TP, tibial plateau.Fig 5. Anterolateral portal view of a medial meniscus bucket-handle tear of a left knee. Both ends of the suture wire are retrieved out of the skin, and while maintaining constant tension on the threads, the everted meniscal bucket-handle fragment is flipped. The patient was placed in a supine decubitus position. The leg was then left hanging over the edge of the operating table during the arthroscopic procedure. FC, femoral condyle.Table 1. Highlights of the Surgical Technique
-
•Perform diagnostic arthroscopy to rule out concomitant intra-articular injuries and assess the extent of the meniscal tear.
-
•Visualize and attempt to reduce the bucket-handle fragment using gentle manipulation techniques.
-
•If the reduction is not achieved, employ an antegrade self-retrieving suture device to stabilize the fragment. Apply a suture at the base of the meniscus fragment, where it turns along the femur condyle.
-
•Use an 18-gauge spinal needle to retrieve the inferior suture first, followed by the superior suture using the outside-in technique.
-
•Once both suture ends are retrieved, maintain constant pull on the threads while pushing the meniscus fragment from the inside using a probe or trocar.
-
•Ensure successful reduction of the fragment without causing damage to the femur condyle or the meniscus fragment.
-
•With successful reduction achieved, repair the remainder of the meniscus using appropriate techniques.
Postoperative Protocol
After surgery, the patient is allowed 0–90° range of motion for 4 weeks. Full extension needs to be achieved in the first 15 postoperative days. The surgeon should consider 2 weeks of immobilization in a knee brace locked in full extension for patients with a preoperative locked knee and an extension deficit. Isokinetic exercises should be started immediately from postoperative day 1. Non–weight-bearing is advised for 4 weeks postoperatively, followed by protected weight-bearing for the following 2 weeks. A broader range of motion (0–120°) is allowed from the fourth postoperative week. Range of motion >120°, kneeling, and squatting should be avoided up to the fourth postoperative month. The patient is followed up at 2 weeks, 1 month, 6 months, and 1 year. Return to sports activities is allowed, depending on the physiotherapy achievements of the patient.
Discussion
Bucket-handle tears are complex meniscal injuries, constituting about 10% of cases.7 MRI is essential for diagnosis, revealing signs like the double posterior cruciate ligament (PCL) and flipped meniscus sign. Missing meniscal bodies in sagittal cuts indicate the absence of the bow tie sign.7^,^8
Long-term studies show increased arthritis after partial meniscectomy.8 Logan et al.9 found higher peak contact pressures after medial BHMT resection during ACL reconstruction. Patients who undergo BHMT repair have less knee pain and better outcomes than those with meniscectomy.8, 9, 10
The literature describes preferred treatment techniques, including inside-out and all-inside repair techniques.2^,^11^,^12 Studies show both techniques effectively restore meniscus biomechanics, with no significant difference in contact area or pressure.12^,^13
Regarding clinical outcomes, good long-term results have been demonstrated for BHMT repairs, both inside-out and all-inside techniques. Samuelsen et al.14 showed clinical success rates of 80% for inside-out and all-inside repairs. They found no difference in clinical success rates, clinical outcome scores, or complication rates between the two techniques. Cetinkaya et al. reported a clinical healing rate of 77% and a radiological healing rate of 81% with MRI for 26 patients, with chronic BHMT repaired using all-inside or inside-out techniques at 6 months postoperatively.15
BHMT is often displaced and unstable, requiring inside-out suture repair with or without all-inside repair.7^,^12^,^16, 17, 18, 19 The rationale for inside-out suture repair is that, unlike all-inside meniscal repair, it permits accurate reduction, stabilization, and coaptation of the tear edges.16 The disadvantages of using an inside-out suture repair include the need for skin incisions either posterolaterally or posteromedially, where there is a risk of common peroneal nerve and saphenous nerve palsy, respectively. Overall, the risk of infections or neurovascular complications has been reported as high as 21%12 (Table 2).Table 2. Pearls and PitfallsPearls
-
•Ensure the patient is well positioned with lateral support and a side pad near the contralateral greater trochanter to facilitate stress maneuvers and ensure proper visualization of the menisci.
-
•In case of a medial meniscal bucket-handle tear, perform a release of the medial collateral ligament using the pie-crusting technique. If a ramp lesion is suspected, perform the posteromedial portal.
-
•Scar tissue around the displaced tear fragment may prevent reduction; therefore, accurate rasping and debridement must be performed before the reduction maneuver.
-
•If the initial reduction attempt is unsuccessful, prompting the need for meniscal-reduction suture techniques, the authors recommend utilizing an antegrade self-retrieving suture device to apply a suture at the base of the meniscus fragment
-
•After an outside-in suture reduces the meniscal fragment, apply minimal traction during stress maneuvers to prevent its redisplacement. Pitfalls
-
•Errors in patient positioning and the omission of placing the side pad near the contralateral greater trochanter could lead to difficulties performing arthroscopy and visualizing intra-articular lesions.
-
•In the presence of a medial meniscus lesion, refraining from performing a release of the medial collateral ligament could hinder the accurate diagnosis of the injury.
-
•If two vertical stitches are not placed at the end of the tear on the meniscus’s anterior and posterior horns using an outside-in technique, there is a risk of lesion propagation.
-
•Granting early weight-bearing on the operated lower limb could lead to failure of the meniscal suture.
In conclusion, the technique described in this study involves using an antegrade self-retrieving suture device along with an outside-in stitch. The goal is to enhance control over reducing the meniscal lesion, which may not be entirely achievable with traditional all-inside stitches alone. Additionally, the method aims to fixate the lesion using all-inside sutures, thereby reducing risks and complications associated with the inside-out technique.
Disclosures
The authors declare (F.B., A.G., D.L.B., F.G., A.M., A.T.) that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rao A.J.Erickson B.J.Cvetanovich G.L.Yanke A.B.Bach B.R.Cole B.J.The meniscus-deficient knee: Biomechanics, evaluation, and treatment options Orthop J Sports Med 32015232596711561138610.1177/2325967115611386 PMC 471457626779547 · doi ↗ · pubmed ↗
- 2Laddha M.S.Shingane D.Modified outside-in repair technique for chronic retracted, unstable bucket-handle anterior horn lateral meniscal tear Arthrosc Tech 112022 e 1747 e 17523631131610.1016/j.eats.2022.06.010PMC 9596603 · doi ↗ · pubmed ↗
- 3Cerciello S.Morris B.J.Panni A.S.Corona K.The rising moon sign is specific and sensitive in the diagnosis of bucket handle tears of the medial meniscus Knee Surg Sports Traumatol Arthrosc 292021111411193255643210.1007/s 00167-020-06108-z · doi ↗ · pubmed ↗
- 4Yik J.H.Koh B.T.H.Wang W.A novel technique for modified all-inside repair of bucket-handle meniscus tears using standard arthroscopic portals J Orthop Surg Res 1220171882920276510.1186/s 13018-017-0692-y PMC 5715506 · doi ↗ · pubmed ↗
- 5Abolaji Alabi I.Chernchujit B.Kanokvaleewong C.Artha A.Pena R.J.Arthroscopic procedure for chronic isolated bucket-handle meniscal tears Arthrosc Tech 102021 e 375e 3833368076910.1016/j.eats.2020.10.011PMC 7917027 · doi ↗ · pubmed ↗
- 6Bosco F.Giustra F.Ghirri A.The pie-crust surgical technique for medial collateral ligament release: Enhancing visualization of the medial compartment in knee arthroscopy Ann Jt 92024143869481210.21037/aoj-23-54PMC 11061655 · doi ↗ · pubmed ↗
- 7Muckenhirn K.J.Kruckeberg B.M.Cinque M.E.Arthroscopic inside-out repair of a meniscus bucket-handle tear augmented with bone marrow aspirate concentrate Arthrosc Tech 62017 e 1221 e 12272935442110.1016/j.eats.2017.04.014PMC 5622027 · doi ↗ · pubmed ↗
- 8FaunøP.Nielsen A.B.Arthroscopic partial meniscectomy: A long-term follow-up Arthroscopy 81992345349141820710.1016/0749-8063(92)90066-k · doi ↗ · pubmed ↗