Mapping stakeholders, services, data, and the information system for adolescent health in the West Bank
Aisha Shalash, Maysaa Nemer, Niveen Abu-Rmeileh, Mohammad Kittaneh, Dervla Kelly, Khalifa Elmusharaf

TL;DR
This study maps adolescent health services and stakeholders in the West Bank to improve coordination and data collection for better healthcare delivery.
Contribution
The first comprehensive mapping of adolescent health services and stakeholders in the West Bank.
Findings
Governmental providers, NGOs, and private entities deliver adolescent health services through various channels like schools and youth centers.
The health information system is fragmented, with inconsistent data collection and reliance on population-based surveys.
Youth centers and schools play key roles in health promotion, and there is a need for updated indicators and integrated data systems.
Abstract
Adolescent health plays a crucial role in shaping lifelong well-being, yet significant gaps exist in addressing adolescent health needs. In conflict-affected regions like the West Bank, fragmented service delivery, inconsistent data collection, and lack of coordination between providers undermine the effectiveness of health services. An efficient health information system ensures accurate data collection, stakeholder integration, and evidence-based decision-making. This study aims to map the landscape of available adolescent health services in the West Bank, clarify the key service providers, determine the existing data sources, and describe the health information system supporting adolescent health. This study utilized a comprehensive landscape analysis to assess adolescent health services in the West Bank. Stakeholder mapping and interviews identified key stakeholders and assessed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
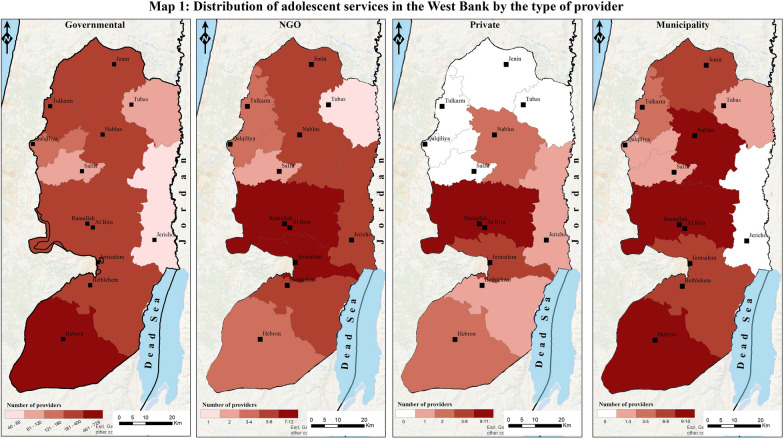 Figure 1
Figure 1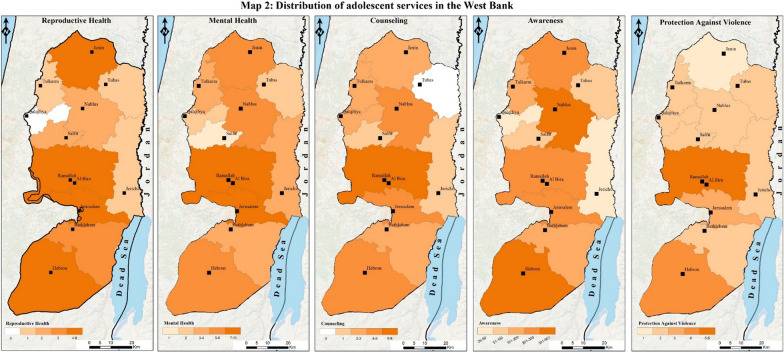 Figure 2
Figure 2- —International Development Research Centre (IDRC)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdolescent Sexual and Reproductive Health · Child and Adolescent Health · Global Maternal and Child Health
Background
The World Health Organization defines adolescence as the age of 10–19 when they face biological, psychological, and physical changes that create the imprint of a person who will eventually lead an independent adult life [1, 2]. Adolescents must have adequate access to proper comprehensive health services during this rapidly changing, vulnerable developmental stage. Investing in the health of adolescents is like investing in generations to come [1, 3–5]. The WHO defines health services as “any service (not limited to medical or clinical services) aimed at contributing to improved health or the diagnosis, treatment, and rehabilitation of individuals and populations” [6]. Successful health services occur when adolescent experiences and cooperation are integrated into the design process [7]. This ensures all needs and wants are met. While providing comprehensive health services is vital to the upbringing of adolescents and the overall improvement of society, the primary objective should be to guarantee these services are accessible, affordable, confidential, and of high quality [8].
Making proper health services available to adolescents globally could result in health equity for all [9]. Moreover, access to proper health services in low- and middle-income countries (LMICs) is crucial because adolescents in LMICs make up 35–50% of the population. Researchers have suggested that modifying existing interventions to serve as a preventive measure would help provide better health services for adolescents in LMICs [10]. One way that has been found to improve health services is by improving the health information system (HIS) [11]. An HIS is a crucial element of a comprehensive health system that collects, processes, and reports data to support policy-making, program development, interventions, and research [12]. The HIS is considered one of the six building blocks of health systems [13]. A well-functioning HIS can provide policymakers with valuable information to guide evidence-based decisions on the different policies and programs that will aid in improving adolescent health outcomes [14]. An effective HIS enables organizations to efficiently coordinate, monitor, and evaluate the humanitarian response in a timely manner [15].
During humanitarian crises, whether they are human-made or caused by natural disasters, women and children are at a heightened risk of violence and vulnerability. This is worsened by limited access to health care, food insecurity, and an absence of autonomy [16]. Many are required to flee their homes, often seeking shelter in schools and hospitals [17]. Countries’ health systems see a strain, an influx of injuries, deaths, disabilities, and a lack of essential medications [18]. Amidst a rise in global crises, with 12 out of the 22 Eastern Mediterranean region countries dealing with armed conflict, the occupied Palestinian territory—encompassing the West Bank, East Jerusalem, and the Gaza Strip—stands as one of these conflict-affected areas [19].
Approximately 50% of the population (5,350,000) in the West Bank and the Gaza Strip is under the age of 18, with 20% classified as adolescents [20]. This demographic composition characterizes the region as having a predominantly young population and requiring tailored healthcare services [21]. Healthcare delivery is provided by four major healthcare providers in the West Bank: The Palestinian Ministry of Health (PMoH), the United Nations Relief and Works Agency (UNRWA), Non-governmental organizations (NGOs), and the private sector. The PMoH and UNRWA adolescent and youth-friendly health services are integrated into primary health care centers and family-friendly services [22]. The PMoH is the main health service provider. Although there are laws that require private facilities to supply data about their services, there is no process in place to ensure this data is reliable and accurate. The combination of a strained health system in the West Bank with the proliferation of different humanitarian organizations with their data systems has resulted in deficiencies in maintaining consistent data and coordination, delivery, and assessment of the activities undertaken by these organizations [23].
The study originated from the imperative for a robust and efficient HIS that is essential for formulating effective policies to address the health requirements of adolescents in the West Bank. Despite the critical role of adolescent health in shaping lifelong well-being, there is a significant lack of understanding regarding the specific services available, the key stakeholders involved, and how these services are prioritized, particularly in conflict-affected settings like the West Bank. The absence of a coordinated HIS leads to fragmented service delivery, inconsistent data integration, and ineffective health interventions for adolescents. Reinforcing HISs enhances decision-making grounded in reliable data, thereby improving intervention strategies and health outcomes. Understanding the adolescent health services system is crucial for grasping the complexities of the HIS. A previous mapping of sexual and reproductive health services for adolescents in the occupied Palestinian territory highlighted the gaps but did not encompass the full spectrum of services and stakeholders involved [24].
The current research maps the landscape of adolescent health services, identifies key stakeholders, and evaluates the existing adolescent health information system (HIS) in the West Bank. The primary objective is to determine the HIS needs crucial for improving adolescent health, with a focus on enhancing adolescent health outcomes and stakeholder coordination. Additional objectives include providing a comprehensive overview of available services, assessing the role of various stakeholders, and analyzing how current data sources influence service delivery and priority setting.
By mapping adolescent health services, stakeholders, and the HIS, this study aims to clarify how these elements can enhance the coordination, delivery, and effectiveness of the HIS, particularly in humanitarian settings. The findings will inform the development of a comprehensive HIS that addresses adolescent needs, improves health outcomes, and facilitates coordinated healthcare delivery in the West Bank.
Methods
In order to achieve this, our study adopted a comprehensive landscape analysis methodology to gain an understanding of adolescent health services, with a specific focus on humanitarian settings [25]. The research approach encompassed stakeholder mapping and analysis, as well as key informant interviews, to explain the landscape for health services provided to adolescents. This landscape also includes the role the health information system plays in providing these services in all parts of the West Bank, including urban, rural, and camp settings.
Stakeholder mapping and analysis
Our study targets stakeholders, including service providers, policy and program decision-makers within various healthcare organizations, governmental bodies, NGOs, and private facilities. In this paper, the analysis of service providers, as one type of stakeholder, is drawn out separately in the analysis section. They refer specifically to stakeholders that directly deliver services to adolescents, such as in clinics, hospitals, youth centers, and schools.
The initial phase of our methodology involved extensive stakeholder mapping and analysis. Using the snowball method, we started with the largest organizations, and then they were able to identify other organizations. We identified and categorized key stakeholders involved in adolescent health services, considering the diverse range of contributors such as healthcare providers (doctors, nurses, mental health professionals), policymakers, educators, community leaders, and individuals from NGOs actively engaged in adolescent health. An adolescent health service provider was determined to be any organization working towards promoting health and minimizing harm to 10–19-year-old individuals [26]. Using a snowball process and conducting internet searches, we mapped stakeholder details. The principal researchers (AS) and (MN) collected the data. Both are fluent in Arabic and have previous experience in conducting stakeholder mappings and landscape analyses. We collected contact information, services and activities offered, indicators, and if any precautions were taken to maintain the confidentiality of patients and participants. All details of each stakeholder found on the internet were then verified by phone or in person by the researchers. The stakeholder details sheet used as a guide for the collection of information can be found in Additional file 1. Stakeholder mapping and analysis served as the first step to identify each stakeholder’s role as either a leading, collaborating or contributing, or funder within the adolescent health services landscape. This mapping and analysis provided a foundation for further recognition of the services that should be accommodating to adolescent health needs.
Key informant interviews
Building upon the insights derived from stakeholder mapping, we conducted key informant interviews and gained invaluable information from stakeholders. AS and a trained research assistant conducted the interviews. Both had prior experience in qualitative data collection and are also fluent in Arabic, which enabled effective communication with the participants. These insights enabled a comprehensive analysis of providers and services, thereby enriching the depth and strengthening the accuracy of our findings. The key informants included representatives of the identified organizations from diverse backgrounds, including healthcare professionals, policymakers, educators, and NGOs, offering a view of the adolescent health services landscape.
Data collected through these interviews captured in-depth perspectives, experiences, and expert opinions about the adolescent health services offered and the role of the health information system in the design and delivery of these services. The interviews were semi-structured, allowing for the questions to be adapted to discuss how the organizations selected services and what kind of health information system is employed. Interviews were done until saturation was reached—no new information from stakeholders was retrieved.
Data analysis
The stakeholder mapping information collected was extracted using Excel. The data collected through key informant interviews underwent thematic analysis using MAXQDA [27]. The interviews were transcribed, and codes were developed by two researchers (AS, KE). The findings were systematically organized to draw meaningful conclusions regarding the current state of adolescent health services and the health information system involving adolescent health. Themes were organized as service availability, data sources, challenges in the health information system, and gaps in service delivery. To validate the findings, we triangulated the data from key informant interviews with stakeholder mapping and secondary data sources, ensuring the accuracy and reliability of the conclusions. This process allowed us to cross-check different sources of information and build a more comprehensive understanding of the services provided and gaps in the system. The methodology for conducting the key informant interviews was the same as that described in our earlier publication [28], where we detailed the interview process, participant selection, and analysis.
Geovisualization method
To geovisualize the findings from the stakeholders’ and providers’ mapping and analysis, we used the geographic information system (GIS) software ArcMap 10.5. This visualization aimed to show the distribution of adolescent services and providers among the 11 Governorates in the West Bank. It will help understand where services are mostly concentrated and whether certain services are scarce in some areas of the West Bank.
To achieve this geospatial visualization, we needed to add three main data sources to the ArcMap software. First, data from the Palestinian Central Bureau of Statistics (PCBS), a reputable organization known for providing a wide range of statistical data for the occupied Palestinian territory, was taken. The data used in this study covers the period up to the year 2022, ensuring the inclusion of the most recent and up-to-date information about the organization and providers within the West Bank and their distribution in the different Governorates, which was available during the analysis phase. Prior to analysis, the data obtained from PCBS underwent preprocessing and preparation to make it compatible with ArcMap 10.5. Second, to obtain the necessary data layers (shapefiles) at the governorate level, the official website for the spatial data of the Ministry of Local Government (MoLG), called GeoMoLG, was accessed. Third, data collected about the number of services and providers were classified by Governorates based on the information obtained about each service. This classification was done using Excel sheets, which were organized in the same order as the other two components (PCBS data files and the shapefiles) so that for each of the 11 Governorates of the West Bank, the number of providers (for each of the four main providers) and the number of services (for each of the five main services) were identified.
To effectively communicate the desired information, careful consideration was given to the map design and symbolism used for the thematic maps. These design choices considered both the intended audience and the research objectives. By utilizing ArcMap 10.5, the collected quantitative data was visualized and analyzed in a spatial context. This approach facilitated the creation of meaningful visual representations that supported the research objectives and provided valuable insights.
Ethical considerations
This research obtained ethical approval from the Ethical Research Committee of the Institute of Community and Public Health at Birzeit University, with reference number 2019 (4–2). Prior to their involvement, each participant offered verbal consent, acknowledging that they retained the right to terminate the interview at any stage. The recording of interviews started after participant consent was given, and individuals were able to stop the recording at any point they felt was necessary. Participants were guaranteed that their interviews would be treated with the utmost confidentiality, ensuring the preservation of their anonymity.
Results
Twenty-one key informant interviews were conducted with different stakeholders engaged in the HIS related to adolescent health. Table 1 provides the characteristics of the stakeholders interviewed.Table 1. Characteristics of stakeholders: interview length and stakeholder categoryIdentification (ID) numberInterview length (min)Stakeholder categorySex of stakeholderYears of experience181GovernmentalMale28 years242Local NGOFemale12 years327Local NGOFemale14 years435Local NGOMale33 years539International NGOFemale20 years658Local NGOMale14 years747GovernmentalFemale15 years822GovernmentalMale22 years930GovernmentalFemale17 years1048GovernmentalFemale14 years1138GovernmentalFemale3 years1229GovernmentalMale5 years1333GovernmentalFemale27 years1429GovernmentalFemale8 years1523International NGOMale13 years1694International NGOFemale20 years1755International NGOFemale5 years1826International NGOFemale15 years1932Local NGOMale12 years2049Local NGOMale23 years2143Local NGOMale24 years
Service availability
Stakeholder mapping
Over 300 different organizations’ websites, social media pages, and contact information were explored during the stakeholder mapping. The stakeholders identified were categorized into four main types: governmental, private organizations, NGOs, and municipalities. It was found that 35 major organizations provide adolescent health services in the West Bank.
Governmental organizations, making up most of the stakeholders (94.7%), are responsible for providing essential health services, often through health facilities and schools. Private organizations (0.85%) offer limited but specialized services, often in collaboration with larger agencies. NGOs (2.05%) are actively engaged in awareness campaigns and targeted interventions for adolescents. Municipalities (services in towns or cities) (2.3%) provide services through youth centers and population-based initiatives. The maps in Fig. 1 illustrate the distribution of these providers throughout the West Bank. These services usually occur in health facilities, schools, and youth centers or are population-based services. The major funders were found to be the United Nations Population Fund (UNFPA) and the United Nations Children’s Fund (UNICEF), while organizations like Oxfam and Save the Children are newly focusing on adolescent health needs. Municipality-run youth centers play a huge role in providing health awareness, counseling, and vocational training. Table 2 shows a breakdown of the major organizations that provide different adolescent health services in the West Bank and their characteristics. The five most mentioned services provided, with their respective overall percentages in the West Bank, were awareness (93.9%), mental health (2.2%), reproductive health (1.3%), counseling (1.3%), and protection against violence (1.1%). The percentages represent the proportion of service delivery points providing said services. Awareness services are health education on various topics, such as reproductive health and nutrition, and they are given in groups, usually in schools or summer camps. Mental health services refer to individual counseling or psychological support. Reproductive health services also refer to individual medical services that are given to boys and girls, usually in a clinical setting, such as family planning. We were able to map these as well, and the distribution within the West Bank can be found in Fig. 2**.**Fig. 1. Distribution of adolescent services in the West Bank by the type of providerTable 2Major organizations providing adolescent health services in the West Bank and their characteristicsName of stakeholder-organizationType of organizationLocation of servicesHealth services offeredSexual and reproductive healthMental healthCounselingProtection against violenceAwareness (educational activities)NutritionVocational and social rehabilitation1. Ministry of HealthGovernmentalSchools, Health Facilities, Population Based ServicesLLLLLL2. Ministry of EducationGovernmentalSchools, Population Based ServicesCLCLLL3. Ministry of Social DevelopmentGovernmentalSchools, Health Facilities, Population Based Services, Youth CentersCCLCL4. Higher Council for Youth and SportsGovernmentalSchools, Youth CentersLLL5. UNRWANGOSchools, Health FacilitiesLLLLLLL6. SAWANGOSchools, Health Facilities, Population-based ServicesCCCCCC7. UNFPANGOFFFFFF8. UNICEFNGOFFFFFF9. Y-PEER Youth Peer Education NetworkNGOSchools, Health Facilities, Youth CentersCCCC10. Good Shepherd Youth Club Jericho (Nadi Shabibet Al-Rai Al-Saleh-Ariha)NGOYouth CentersCCCC11. Palestinian Medical Relief SocietyNGOSchools, Health Facilities, Youth CenterCCCCCCC12. Union of Health Care Committees (UHCC)NGOHealth Facilities, Youth CentersCCCCC13. Juzoor for Health and Social DevelopmentNGOSchools, Health Facilities, Youth CenterCCCCCC14. Hebron Youth Development Resource Center (YDRC)NGOSchools, Health Facilities, Youth CentersCCCC15. Youth Development Association (YDA)NGOYouth CentersCC16. Young Men’s Christian Association (YMCA)NGOSchools, Health Facilities, Youth CentersCCCCCC17. Independence Youth UnionNGOYouth CentersCC18. Al-Ofoq foundation for youth developmentNGOYouth CentersCC19. Al-Sadiq Al-Taieb AssociationNGOSchools, Health Facilities, Youth CentersCCCC20. Caritas CenterNGOSchools, Health Facilities, Youth CentersCCCC21. Save the ChildrenNGOSchools, Health Facilties, Youth CentersCCCCCCC22. OxfamNGOFFFFF23. SharekNGOSchools, Youth CentersCCC24. Palestinian Family Planning & Protection Association (PFPPA)NGOHealth FacilitiesCCCCC25. Palestinian Counseling CenterNGOHealth FacilitiesCCCC26. Sourif MunicipalityMunicipalityYouth CentersCC27. Ramallah MunicipalityMunicipalitySchools, Youth CentersCCC28. Al-Bireh MunicipalityMunicipalitySchools, Youth CentersCCC29. Taqoua’ MunicipalityMunicipalitySchools, Youth CentersCC30. As-Samua' MunicipalityMunicipalitySchools, Youth CentersCC31. Kufr Thulth MunicipalityMunicipalitySchools, Youth CentersCCC32. Kufur Rai' MunicipalityMunicipalitySchools, Youth CentersCC33. As-Sawahreh Ash-Sharqiyeh Local CouncilMunicipalitySchools, Youth CentersCC34. Beit Ula MunicipalityMunicipalitySchools, Youth CentersC35. Tomorrow’s Youth OrganizationNGOYouth CentersCCCC^^L = Leading services, F = Funding services, C = CollaboratingFig. 2Distribution of adolescent services in the West Bank
The analysis of the distribution of adolescent health services across the West Bank, as illustrated in Figs. 1 and 2, reveals several patterns. Services are predominantly concentrated in certain areas, reflecting the centralization of resources and infrastructure in these regions. This bias is evident in the clustering of facilities and programs in cities and towns, leaving rural regions underserved. The unequal geographic distribution leaves adolescents in certain areas facing limited access to essential health services. The type of service provider also shows patterns in governmental organizations providing most of the adolescent health services. NGOs, while fewer in number, appear to target areas with identified gaps in governmental service delivery, suggesting a complementary role. Private organizations and municipality-run youth centers provide additional, limited services focused on specific health needs or community initiatives. The presence of multiple providers in the same region, however, raises concerns about potential overlap and duplication, highlighting the need for improved coordination among stakeholders.
The maps demonstrate that specialized services, such as mental health and reproductive health, are concentrated in areas, while rural areas are primarily limited to general health awareness and counseling. These patterns collectively point to the urgent need for targeted interventions to expand adolescent health services in underserved regions and strengthen coordination mechanisms to optimize resource use and service delivery. After a comprehensive understanding of the major organizations and their distribution, the following exploration focuses on the specific settings where adolescent health services are delivered: health facilities, schools, youth centers, and population-based services.
Service settings
Health facilities
Adolescent health services are provided in all primary health care clinics and mobile clinics as part of family health services and not exclusively for adolescents. Primary health care services are mainly offered by the PMoH, UNRWA, the Palestinian Medical Relief Society (PMRS), and the Union of Health Care Committees (UHCC). The PMRS mobile clinics are also available to provide medical and psychological consultations to underserved communities and regions with inadequate medical care. These clinics are staffed by a general practitioner who performs medical examinations and consultations and a psychologist who provides psychological consultations. The locations of these clinics are determined according to an annual plan, ensuring that they are accessible to those who require them the most.
Schools
As of the 2022/2023 school year, there are a total of 2394 schools in the West Bank. These include 1896 governmental, 96 operated by UNRWA, and 402 private schools. In the school-focused health initiatives, the organizations prioritize comprehensive health education for adolescents, directing efforts towards 9th to 11th-grade students in all government and private schools on an annual basis. The seamlessly integrated school health program is an integral part of their broader child health initiative, offering health checks for students up to the age of 18. They encompass students from kindergarten to 12th grade, addressing critical issues such as adolescence and early marriage awareness. Recognizing the pivotal role of nutrition in schools, policies underscore balanced nutrition and the promotion of healthy habits. Implementation of health awareness campaigns, electronic monitoring systems for students' nutritional status, and vaccination programs for 6th, 8th, and 9th-grade students all align with the overarching commitment to comprehensive adolescent health within the school environment.
Youth centers
Youth centers in the West Bank, operated by community-based organizations, serve as invaluable hubs providing free services for adolescents and youth, fostering a secure environment for skill development and leisure activities. We were able to map ten youth centers throughout the West Bank, and they were mainly municipality initiatives. These centers deliver educational programs spanning gender equality, mental health, and sexual/reproductive health, with a particular emphasis on encouraging peer-driven knowledge exchange. Complementing these initiatives are awareness programs addressing various health topics. Specific programs, such as the Youth Empowerment Program for girls aged 14–18 and the Big Brother-Big Sister Program, offer targeted support, aiding adolescents in overcoming challenges like social stigma and gender-based violence. These centers not only strengthen community and familial bonds but also provide psychological assistance for issues ranging from sexual/reproductive health to family relationships, ultimately empowering adolescents to navigate societal pressures authentically.
In response to the evolving healthcare landscape in the West Bank, essential services have been established that are accessible to all residents, irrespective of their affiliation with health facilities, schools, or youth centers. Among these newly introduced services is a comprehensive vaccination program, which extends free vaccination services to all children and adolescents. In addition to the introduction of the 121 Hotline by the NGO, Sawa addresses medical concerns by offering free consultations for individuals of all ages, with a dedicated focus on child protection for those under 18. This listening line, complemented by a user-friendly phone application, facilitates virtual appointments with healthcare professionals, which are bookable through WhatsApp. Notably, the 121 Hotline has forged partnerships with major social media platforms, including Facebook, Instagram, and TikTok, enabling the swift removal of harmful content, electronic bullying, or inappropriate material within 72 h.
Gaps in service delivery
Significant gaps exist in the delivery of services in the West Bank, such as comprehensive sexual education and contraceptive access. Comprehensive sexual education programs are absent, leaving adolescents without a full understanding of sexual health. In primary healthcare clinics, married adolescent girls have access to contraceptive services, but these are not available to unmarried adolescents. Data collection in health facilities is limited because adolescents, who are generally healthy, rarely attend these facilities for services. Health information related to awareness and counseling is typically not recorded, further limiting the availability of comprehensive data on adolescent health.
Many services for adolescents are funded based on international priorities rather than local needs. These services often depend on project-based funding aligned with donor priorities, which may not necessarily reflect the specific needs of the local population. The reliance on external funding results in a lack of continuity when priorities shift and was highlighted by funders. When asked how they decide on the projects to implement, the majority indicated that the availability of external funding primarily drives their decisions.“We mainly fund projects, but we do not provide direct services. Our funds usually come from a call or grant that we have applied for and are granted. We then find the most appropriate organization to provide this service.” Stakeholder ID # 16.
Data sources
Population-based surveys/census
Most of the adolescent health statistics come from population-based surveys, which are household and school-based. The most popular school-based surveys are the Global Health School Survey and the Global Youth Tobacco Survey. The Multiple Indicator Cluster Survey in occupied Palestinian territory only included married women 15–19 from the adolescent age group. A youth survey was also done in Palestine, but the focus was on the ages 18–29. The last census was in 2010, and no adolescent health statistics were obtained from the survey. Surveys are the most used source to understand behavior risk facts such as smoking, nutritional status, educational level, and employment. Population-based surveys are funded by organizations such as UNICEF and UNFPA.“An organization comes to the PCBS and asks us to do this survey…This is how we decide which surveys are done.” Stakeholder ID #19
A gap of information in the population-based surveys was found amongst the 10–14 age group. When asked about why there was a lack of data and indicators for this age group, a few of the stakeholders recalled that the country's definition of adolescents starts at the age of 15.“You will find a gap in the health information of 10–14 because the country defines adolescents and youth as starting at the age of 15. You will find information on work indicators even though the age starts at 15 because 10–14 years is considered to be child labor and taken into consideration.” Stakeholder ID #20.
Challenges in the health information system
A variety of providers offer adolescent health care services. Each provider is tasked with gathering data from their respective facilities, such as the type of service provided, the number of adolescents treated, and supply statistics. This data must be included in the annual report. However, providers utilize different health management information systems, with the Ministry of Health facilities using AVICENNA in hospitals and DHIS2 in primary health care clinics. This variance in systems presents a challenge for integrating data from primary and secondary facilities. When the different organizations were asked about the system of sharing data with others, all answered that they submit an annual report to the MoH every year.“We submit an annual report to the Ministry of Health every year.” Stakeholder ID #6“There is a yearly report, and in the yearly report, we give a summary of the statistics and what programs were offered and who attended these programs.” Stakeholder ID #18.
When asked if data is used to decide if a program is a priority, many organizations described using internal needs assessments. When the researchers asked for a copy of these assessments, they were told they were not for publication. It was clear that in most organizations, some monitoring and evaluation is used but has not been published.“We do need assessments, before and after, to monitor and evaluate our projects internally…. These reports are not published.” Stakeholder ID #4
Also, many health organizations and providers do not have a unified system for data sharing, which results in fragmented data collection efforts, making it hard to make evidence-based decisions. Many stakeholders reported adolescent health data comes from population-based surveys, and the available indicators are derived from these surveys.
In the final phase of the interviews, key informants were queried about the utilization of adolescent health indicators in the decision-making process for implementing services. Several stakeholders expressed concern over the absence of up-to-date adolescent health indicators, emphasizing the necessity of adopting priority indicators. It was noted that adolescent health services, being a new focus, have garnered increasing interest from international organizations and funders in recent years.“We prioritize which indicators we should focus on, which ones are more relevant and publicize it to all organizations. This will help us when we design new projects, interventions, and programs, refer to these indicators, and see that they are the most relevant to the Palestinian context. Those are the more relevant to SDGs and to the future interventions that we want to make, and then we can unify them for all the organizations.” Stakeholder ID #3.
When asked what indicators they would like to see available on the priority list, a few stakeholders mentioned the importance of mental health indicators as well as employment indicators."… Unfortunately, they are out there, and nobody knows what they are doing. So, I think statistics related to adolescence in the labor force would be another important indicator to see how it is influencing their future and how that is influencing their health status, mental status, you know, social, and economic status." Stakeholder ID #15."Definitely, mental health and psychosocial status of science would be another area, and indicators around that would be important given the reality. Unfortunately, that and the Palestinian people are facing, you know, violence on a daily basis, and the mixed results most recently has also indicated the increase of domestic violence." Stakeholder ID #13.
The findings of this study offer an understanding of the adolescent health services landscape, highlighting gaps in service delivery and coordination. These results serve as a foundation for discussing the implications of improving adolescent health outcomes and strengthening the HIS in the West Bank for evidence-based service allocations.
Discussion
The stakeholder mapping involved exploring over 300 organizations and revealed 35 major organizations that delivered adolescent health services in the West Bank. Primary funders included UNFPA and UNICEF, with emerging focus from Oxfam and Save the Children. Youth centers play a significant role in health awareness and vocational training. Reproductive health, mental health, counseling, awareness, and protection against violence were the services that were most provided. Settings for service delivery included health facilities, schools, and youth centers. Key informant interviews revealed international priorities influencing funding decisions, while surveys and health facility data shaped national priorities. Challenges included integrating data from diverse systems and a need for updated indicators.
Understandably, the most provided services were reproductive health, mental health, counseling, and protection against violence, as these are found to be the most needed services for adolescents in humanitarian settings [29–31]. The primary types of services that are offered are awareness programs, which align with most adolescents being healthy and needing programs to advocate prevention and not treatment [32]. Advances in reproductive health in humanitarian settings have improved access to services, but significant gaps remain in maternal and newborn health, family planning, gender-based violence, and HIV/STIs [33]. Water, sanitation, and hygiene (WASH) interventions are also considered to be important [34], but no adolescent WASH interventions were found or documented in the West Bank. A great focus is placed on reproductive health and mental health during crisis times because adolescents are more vulnerable to risks and conditions and sometimes must play the role of an adult before passing through the developmental phase of adolescence [35]. This occurred in Lebanon amongst Syrian refugees, with adolescents dropping out of educational establishments and adolescent girls getting married [36]. The Palestinian Educational System is currently working on incorporating sexual education, mental health, gender roles, and gender equity and equality into the educational curriculum [37]. There currently is no sexual education program in the current system. Furthermore, two studies have been done on the perception of sexual education and knowledge of university students in different geographical regions in the occupied Palestinian territory [38, 39]. A potential reason for the disparity in SRH knowledge was noted between students who attended private schools in the occupied Palestinian territory, where co-educational settings and some sexual education might be provided [38, 39].
Developing programs and encouraging service delivery in these areas is essential. Mobile clinics are used in some rural areas, but one recommendation could be the use of telehealth. In a systematic review done to measure the satisfaction of rural patients with telehealth, it was found that they were satisfied with their access to health care and had less travel time [40]. A hotline is currently available, but it would be necessary to advertise widely as most adolescents do not know about this service. A current evaluation of the hotline's use would allow for suggestions to improve and increase use. Schools and youth centers are found to be the best places for adolescents to receive services, given that is where they spend most of their time. Youth centers can be an alternative to health facilities as most adolescents are seen as healthy and are less likely to go to health facilities, especially girls, in fear of the stigma of being unwell [41].
With the main programs being of international priority, there can sometimes be seen as a lack of local ownership, leading to unsustainability of the programs lasting beyond the funding of the programs being offered [42]. A recent study described the health response in Yemen as being more effective when the local community was involved, allowing for the sustainability of health services in the future [43]. It has also been observed that involving local youths in humanitarian responses and providing them with support within the system elicits a more positive reaction, fostering a sense of belonging during challenging times. This was evident in Sierra Leone during the response to the Ebola outbreak [44]. Integrating locals into the decision-making processes would be essential. It is vital to invest in the response capacity of national NGOs, which allows for a more tailored approach to addressing specific local needs rather than adhering strictly to international agendas [45]. This shift enhances program effectiveness and strengthens local capabilities, ensuring the sustainability and relevance of interventions. By capitalizing on local knowledge and expertise, international donors can better align their strategies with the actual health needs and priorities of adolescents in the West Bank, fostering a more collaborative and impactful approach to health service delivery. Also, it has shown that programs are more effective when local actors are involved in the coordination, execution, and monitoring [43].
During these times, humanitarian organizations require pre-humanitarian data to help plan their response [46]. The situation is seen as a lack of well-defined indicators concerning adolescents, especially in low- and middle-income countries [47]. The Global Action for Measurement of Adolescent (GAMA) health initiative has identified 52 priority adolescent health indicators [48]. Still, it has yet to test the feasibility and reliability of these indicators in humanitarian settings. Some of the included priority indicators are the prevalence of obesity, tobacco use, alcohol use, and anemia. Integrating adolescent health indicators and data more seamlessly into the health information system will facilitate the sharing of information, enabling a more effective response to the specific health needs of adolescents [49]. Currently, population-based surveys are identified as the most effective means of gathering comprehensive data on adolescent health, primarily targeting older adolescents 15–19 years old. However, a lack of data on younger adolescents aged 10–14 years is evident in most low-and-middle income countries, not just in humanitarian settings. Conducting surveys for this younger age group is often challenging due to their classification as children, but it is feasible to collect through school-based surveys [50].
Modifying existing surveys to include younger adolescents and males would help increase data on these age and sex groups. Instead of using household surveys, we should use school surveys to effectively reach this age and sex group, taking into consideration that you will be losing out-of-school adolescents. Using online surveys will help increase anonymity and allow adolescents to answer questions more honestly compared to being in school. It would be essential to be creative in data collection techniques.
Conclusion
In conclusion, this study underlines the critical importance of developing and integrating a comprehensive health information system to enhance the coordination, delivery, and effectiveness of adolescent healthcare services in the West Bank, particularly within humanitarian contexts. By improving accessibility, coordination among healthcare providers and humanitarian organizations, and the availability of timely data, such a system holds the potential to impact adolescents' health outcomes significantly.
The triangulation of stakeholder mapping and key informant interviews ensured a holistic exploration of the factors influencing the provision of health services to adolescents, contributing valuable knowledge to the existing literature and informing how the health information system can be used to make informed program decisions. The main challenge of the health information system regarding adolescent health was data integration. Needs assessments done by NGOs, being shared, will help combat repetition and will allow for resources to be used for other needed programs. The adoption and development of comprehensive adolescent health indicators to enhance decision-making and improve the monitoring and evaluation of programs is important. GAMA has identified a draft of the priority list, and it is important to determine the current indicators that are currently available and the feasibility of collecting these indicators in the current context. Further research will help determine the strengths and challenges the current health information system has in tailoring to the needs of adolescent health.
Strengths and weaknesses
One of the main strengths seen was the ability to accumulate major stakeholders of adolescent health in the West Bank and verify the available information—adding main stakeholder input allowed for a comprehensive understanding of the adolescent health service landscape. A more comprehensive study, including the Gaza strip, is needed. Although we are aware of certain stakeholders servicing Gaza, a comprehensive mapping of their involvement was not feasible within the scope of this study.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abou Zahr C, Boerma T. Health information systems: the foundations of public health. Bull World Health Org. 2005;83578–83.PMC 262631816184276 · pubmed ↗
- 2Chynoweth SK. Advancing reproductive health on the humanitarian agenda: the 2012–2014 global review. Conflict Health. 2015;9.10.1186/1752-1505-9-S 1-S 3PMC 433181525798189 · doi ↗ · pubmed ↗