Combined Cytomegalovirus Retinitis and Vitreous Hemorrhage in an Immunocompromised Patient
Abdulrahman Y. Alhoumaily, Abdulsalam M. Dheyab

TL;DR
This case study highlights a rare combination of CMV retinitis and vitreous hemorrhage in an HIV patient, emphasizing the need for careful diagnosis to avoid treatment delays.
Contribution
The paper presents a novel case highlighting the importance of considering concurrent infectious retinitis in immunocompromised patients with vitreous hemorrhage.
Findings
A 38-year-old HIV patient presented with vitreous hemorrhage and preretinal hemorrhage linked to CMV retinitis.
The case emphasizes that vitreous hemorrhage in immunocompromised individuals may not be solely due to ischemic vasculitis.
Combined CMV retinitis and vasculitis was diagnosed and treated after initial treatment failure.
Abstract
Purpose: This study is aimed at describing a case of combined CMV retinitis and vitreous hemorrhage in an immunocompromised patient. Observations: A 38-year-old male who is known to have HIV presented to our emergency department complaining of decreasing vision in his left eye. Vitreous hemorrhage and preretinal hemorrhage were observed upon examination and were thought to be caused by CMV retinitis. After initial treatment and worsening condition upon follow-up, a diagnosis of combined CMV retinitis and vasculitis was considered and was treated accordingly. Conclusions: The presence of vitreous hemorrhage in immunocompromised patients should not be attributed to just an ischemic vasculitis alone, and the possibility of concurrent infectious retinitis should be looked for carefully to avoid delay in treatment.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
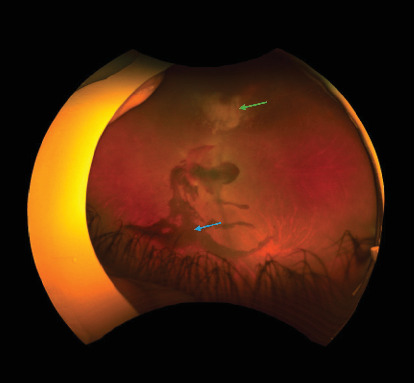 Figure 1
Figure 1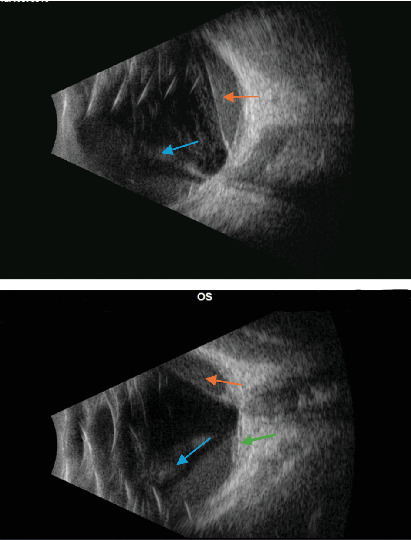 Figure 2
Figure 2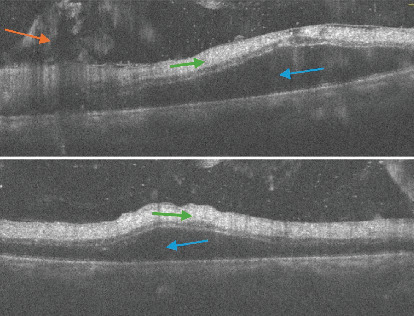 Figure 3
Figure 3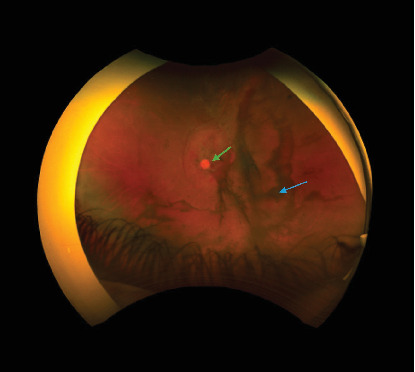 Figure 4
Figure 4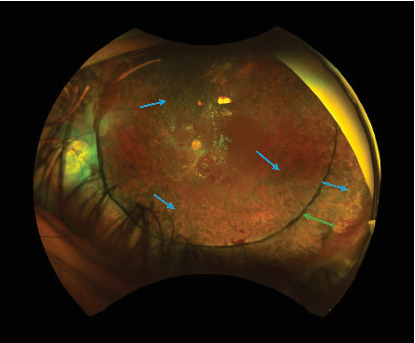 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Ocular Diseases and Behçet’s Syndrome · Toxoplasma gondii Research Studies
1. Introduction
Cytomegalovirus is a double stranded DNA virus attributed to the Herpesviridae group of viruses. Usually, it is asymptomatic in immunocompetent individuals, but in a low percentage, it can cause mononucleosis [1]. Other manifestations, which are increased in immunosuppressed states, include hepatitis, esophagitis, pneumonitis, and transverse myelitis [2]. Ophthalmic manifestations include CMV iridocyclitis, CMV endotheliitis, CMV retinitis, and CMV retinal vasculitis [3]. CMV iridocyclitis and CMV endotheliitis are typically linked to immunocompetent individuals, while CMV retinitis and CMV retinal vasculitis are more likely to be associated with immunocompromised patients. Vitreous hemorrhage has been described in a minority of cases of CMV retinitis, mostly secondary to retinal ischemia and occlusive vasculitis.
The incidence of the various manifestations caused by this virus is highly dependent on patient immune status. In regard to ocular involvement, posterior segment involvement, that is retinitis and ischemic vasculitis, is correlated with lower CD4+ counts in comparison to anterior segment involvement. In these states, CD4+ counts are usually < 200 cells/microliter [4]. Systemic anti-CMV treatment is usually needed in CMV retinitis and vasculitis, while in anterior segment involvement, systemic, topical, and local antiviral medications are tried, with no consensus about the best modality of treatment [5].
2. Case Description
Our patient is a 38-year-old male, a known case of HIV, for which he is currently on emtricitabine/tenofovir, alafenamide, and dolutegravir treatment for the past 2 months. The patient's past ophthalmic history is unremarkable. He presented to our emergency department complaining of decreasing vision in the left eye. His UCVA in the left eye was counting fingers (CFs) and 20/20 in the right eye. He reported no flashes, floaters, or any history of trauma. Slit lamp examination of the left eye showed mutton-fat keratic precipitates as well as an anterior chamber reaction. Fundus examination showed vitritis associated with vitreous hemorrhage and areas of retinitis (Figures 1 and 2). An area of preretinal hemorrhage over the disk and part of the macula was detected, but proper visualization of the disk and retina was not possible because of the vitreous hemorrhage. OCT of the left eye showed vitreous opacities, preretinal hyperreflective material suggestive of preretinal hemorrhage, subretinal fluid, hyperreflectivity of inner retinal layers, and loss of retinal layer stratification, suggestive of severe retinal ischemia (Figure 3).
Because of the immune status of the patient and the presence of hemorrhagic retinitis, the diagnosis of cytomegalovirus retinitis was considered and speculated. Although vitreous and preretinal hemorrhage was not explained by this preliminary diagnosis, our initial thought was that it may be due to posterior vitreous detachment secondary to the vitritis or due to the inflammation. The patient was treated as a case of CMV retinitis and was started on valganciclovir 900 mg BID and a series of intravitreal injections of ganciclovir. Upon follow-up, retinitis seemed to improve but the preretinal hemorrhage as well as the hemorrhage over the disk seemed to persist (Figure 4). One month later, slit lamp examination showed neovascularization on the iris (NVI). Fluorescein angiography revealed ischemic retina, and the patient was planned to have panretinal photocoagulation as well as intravitreal injection of Avastin.
On the next follow-up appointment, the patient presented with rapidly decreasing vision and increasing vitreous hemorrhage. Pars plana vitrectomy was planned and done. After vitrectomy and aspiration of the preretinal hemorrhage, a fibrovascular membrane over the disk and macula was found. Peeling of the membrane, augmentation with laser photocoagulation, and silicone oil injection were done (Figure 5).
These intraoperative findings, along with the angiography findings, suggested ischemic retinitis and vasculitis, most likely secondary to the CMV infection. During the postoperative follow-up period, the patient demonstrated improving vision, but the macula appeared to be atrophic, most likely due to the ischemia and vasculitis. At final follow up, the patient had a UCVA of 20/200, and the elements of retinitis and vasculitis resolved.
3. Discussion
CMV retinitis is a common ocular opportunistic infection in immunocompromised patients. It is usually associated with retinal vascular changes, and retinitis typically starts and distributes along the retinal blood vessels. It is suggested that the retinal vascular changes are secondary to the CMV infection, leading to retinal ischemia with possible retinal neovascularization, vitreous hemorrhage, or traction retinal detachment [6]. Immunohistochemical studies detect CMV proteins in the retinal vascular endothelium adjacent to the areas of retinal involvement, with the vascular endothelium being proposed as the primary site of CMV infection in the retina. In HIV patients, the exact role of HIV vasculopathy in the development of CMV retinitis is still controversial [7]. Despite the common association with retinal vasculitis and retinal ischemia, CMV retinitis rarely presents concurrently with vitreous hemorrhage.
Ch'ng et al. reported a case of CMV retinitis presented as vitreous hemorrhage in a patient with T-cell prolymphocytic leukemia treated with a course of alemtuzumab [8]. However, most other case reports reported vitreous hemorrhage in CMV retinitis after treatment or healing of CMV retinitis, but not as a presenting sign with active CMV retinitis [9–12].
Some other case reports attributed vitreous hemorrhage in HIV-infected patients to immune recovery after starting HAART therapy, and the authors thought that the retinal neovascularization and vitreous hemorrhage were caused by retinal ischemia and were induced by an enhanced immune response to CMV in the retina after partial immunologic restoration from HAART therapy [13–15]. In our case, being an HIV patient with hemorrhagic retinitis suggestive of CMV retinitis and on HAART therapy, the role of HIV vasculopathy, CMV vasculopathy, and HAART-induced immune recovery vasculopathy cannot be ruled out, and they could all contribute to the development of this unusual presentation of combined vitreous hemorrhage with active CMV retinitis.
4. Conclusion
The presence of vitreous hemorrhage in immunocompromised patients should not be attributed to just an ischemic vasculitis alone, and the possibility of concurrent infectious retinitis should be looked for carefully to avoid delay in treatment, with the possibility of disastrous visual outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Faith S. C. Durrani A. F. Jhanji V. Cytomegalovirus Keratitis Current Opinion in Ophthalmology 201829437337710.1097/ICU.00000000000004812-s 2.0-8504925788329708927 · doi ↗ · pubmed ↗
- 2Gupta M. Shorman M. Cytomegalovirus 2017 Stat Pearls Publishing 29083720 · pubmed ↗
- 3Kobayashi R. Hashida N. Overview of Cytomegalovirus Ocular Diseases: Retinitis, Corneal Endotheliitis, and Iridocyclitis Viruses 2024167 p. 111010.3390/v 1607111039066272 PMC 11281654 · doi ↗ · pubmed ↗
- 4Kim Y. S. Sun H. J. Kim T. H. Kang K. D. Lee S. J. Ocular Manifestations of Acquired Immunodeficiency Syndrome Korean Journal of Ophthalmology 201529424124810.3341/kjo.2015.29.4.2412-s 2.0-8501285004026240508 PMC 4520867 · doi ↗ · pubmed ↗
- 5Faulds D. Heel R. C. Ganciclovir: A Review of Its Antiviral Activity, Pharmacokinetic Properties and Therapeutic Efficacy in Cytomegalovirus Infections Drugs 199039459763810.2165/00003495-199039040-000082-s 2.0-00252339182161731 · doi ↗ · pubmed ↗
- 6Riordan-Eva P. Williams C. E. Wing A. J. Graham E. M. Sanders M. D. Retinal Neovascularization Secondary to Cytomegalovirus Retinitis in Wegener's Granulomatosis Journal of the Royal Society of Medicine 199386530130210.1177/0141076893086005237685050 PMC 1294015 · doi ↗ · pubmed ↗
- 7Fabozzi L. Testi I. De Benito-Llopis L. Pavesio C. Cytomegalovirus Anterior Uveitis and Occlusive Retinal Vasculitis Without Retinitis in a Patient on Immunomodulatory Therapy Journal of Ophthalmic Inflammation and Infection 2023131 p. 3410.1186/s 12348-023-00356-z 37540447 PMC 10403449 · doi ↗ · pubmed ↗
- 8Ch’ng S. W. Brent A. Banerjee S. Cytomegalovirus RETINITIS Retinal Cases and Brief Reports 201481505110.1097/ICB.00000000000000022-s 2.0-8489804687525372208 · doi ↗ · pubmed ↗