The Impact of Government Lockdowns on the Mental Health of the General Population: A Systematic Review and Meta-analysis
Yuji Okazaki, Yasushi Tsujimoto, Kohei Yamada, Natsumi Saka, Takashi Ariie, Shunsuke Taito, Masahiro Banno, Yuki Kataoka, Norio Watanabe

TL;DR
This study reviews how government lockdowns during disease outbreaks like COVID-19 affect mental health, finding uncertain evidence of significant impacts.
Contribution
The paper provides a systematic review and meta-analysis of lockdown effects on mental health during infectious disease outbreaks.
Findings
Government lockdowns may have little to no effect on depressive symptoms, but evidence is very uncertain.
Lockdowns may increase PTSD and insomnia symptoms, but evidence certainty is low.
Little to no effect on anxiety and alcohol use was observed, but results remain uncertain.
Abstract
Since December 2019, the COVID-19 pandemic has spread globally, prompting governments in many countries to implement lockdowns to control the transmission of the virus. Outbreaks of emerging infectious diseases, such as COVID-19, and the associated government lockdowns may have significant negative impacts on mental health. A comprehensive review of the available evidence on this topic can provide useful information for policymakers. This review aimed to assess the effects of government lockdowns on the mental health of the general population during emerging infectious disease outbreaks. On April 11, 2022, we conducted a systematic search of CENTRAL, MEDLINE, PsycINFO Ovid, and two clinical trial registries, supplemented by reference checking and citation searching. We included non-randomized studies of interventions (NRSIs) involving adults and adolescents, regardless of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
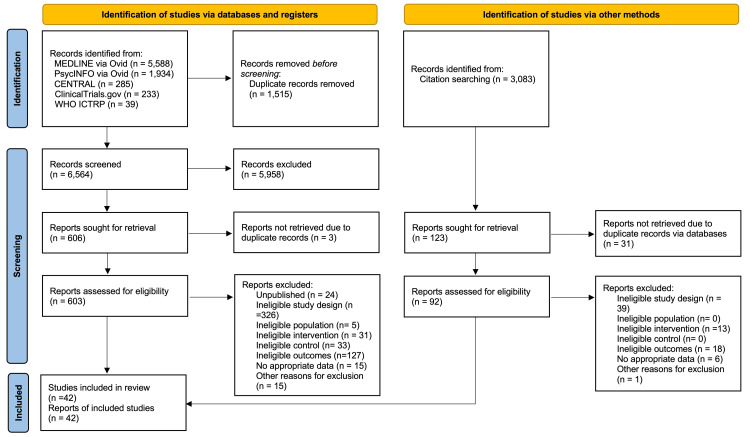 Figure 1
Figure 1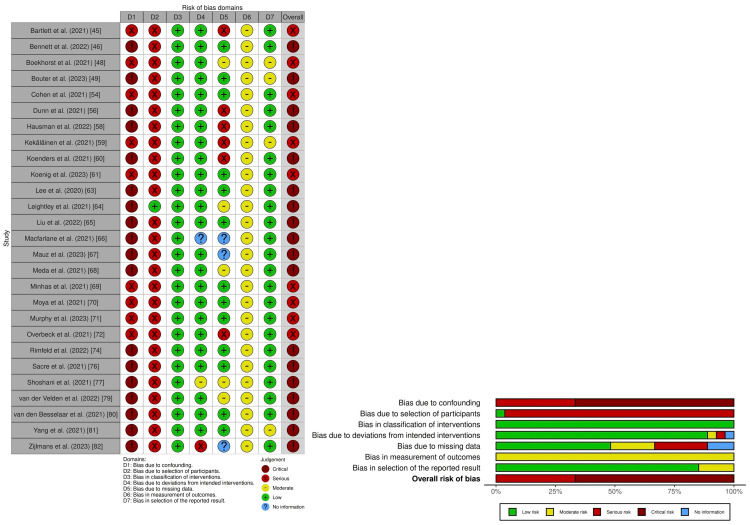 Figure 2
Figure 2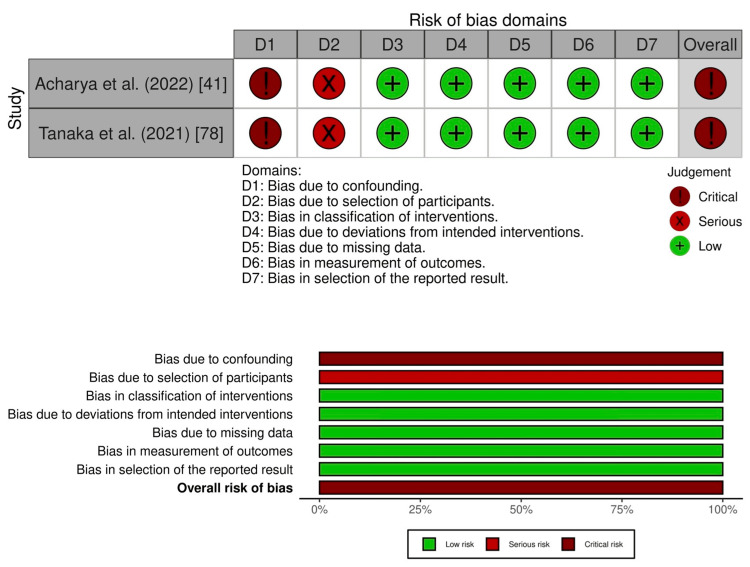 Figure 3
Figure 3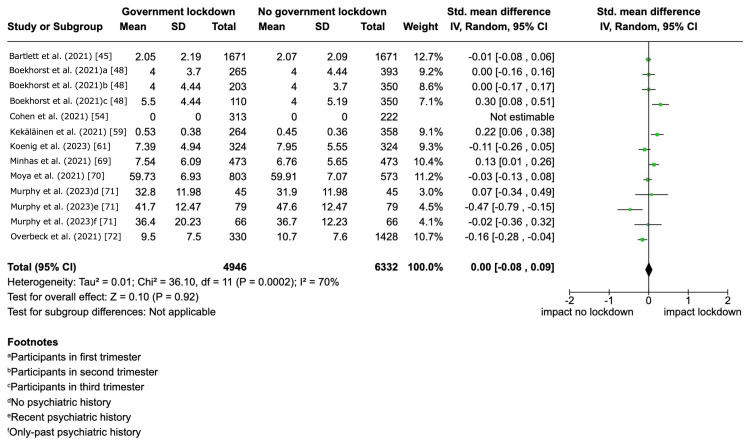 Figure 4
Figure 4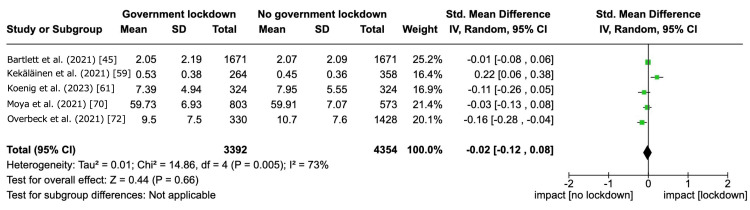 Figure 5
Figure 5| Study (year) | Country* | Methods (design, key design feature) | Participants | Interventions | Outcomes |
| Acharya et al. (2022) [ | Nepal (low or middle income) | Retrospective (time differences) | General population | Lockdown | Suicide |
| Albrecht et al. (2022) [ | Switzerland (high income) | Cross-sectional surveys (time differences) | 12,238 high school students | Lockdown | Substance use (tobacco, alcohol) |
| Arad et al. (2021) [ | Israel (high income) | Longitudinal (time differences) | 99 undergraduate freshmen | COVID-19 lockdown | Anxiety symptoms |
| Barbosa et al. (2021) [ | United States (high income) | Cross-sectional (time differences) | 556 adults | Stay-at-home orders | Alcohol use |
| Bartlett et al. (2021) [ | Australia (high income) | Longitudinal (time differences) | 1,671 adults (50+ years) | Lockdown restrictions | Depressive symptoms, anxiety symptoms, alcohol use |
| Bennett et al. (2022) [ | United Kingdom (high income) | Longitudinal (time differences) | 6,330 university students | National lockdown | Depressive symptoms, anxiety symptoms |
| Berthelot et al. (2020) [ | Canada (high income) | Longitudinal (time differences) | 2,078 pregnant women | Public health emergency | Post-traumatic stress disorder symptoms |
| Boekhorst et al. (2021) [ | Netherlands (high income) | Longitudinal (time differences) | 669 pregnant women | Nationwide lockdown | Depressive symptoms |
| Bouter et al. (2023) [ | Netherlands (high income) | Longitudinal (time differences) | 445 adolescents | Lockdown | Depressive symptoms, anxiety symptoms |
| Burdzovic Andreas and Brunborg (2022) [ | Norway (high income) | Longitudinal (time differences) | 2,536 adolescents | Nationwide lockdown | Alcohol use |
| Cellini et al. (2021) [ | Italy and Belgium (high income) | Cross-sectional (time differences) | 1,622 (Italy) and 650 (Belgium) adults | Lockdown | Insomnia symptoms |
| Cellini et al. (2021) [ | Italy (high income) | Cross-sectional (time differences) | 299 mothers | National lockdown | Insomnia symptoms |
| Cody et al. (2021) [ | Switzerland (high income) | Cross-sectional (time differences) | 165 individuals with depression | COVID-19 lockdown | Insomnia symptoms |
| Cohen et al. (2021) [ | Netherlands (high income) | Cohort (time differences) | 535 patients with hand/wrist conditions | Intelligent lockdown | Depressive symptoms, anxiety symptoms |
| Cousijn et al. (2021) [ | Netherlands (high income) | Cross-sectional | 120 cannabis users | Dutch lockdown | Cannabis use |
| Dunn et al. (2021) [ | United States (high income) | Longitudinal (time differences) | 48 adults with cochlear implant | State of public health disaster emergency | Depressive symptoms, anxiety symptoms |
| Gonzalez-Martinez et al. (2021) [ | Spain (high income) | Longitudinal (time differences) | 158 patients with epilepsy | Lockdown | Anxiety symptoms, Insomnia symptoms |
| Hausman et al. (2022) [ | United States (high income) | Longitudinal (time differences) | 189 older adults | Stay-at-home orders | Depressive symptoms, anxiety symptoms, insomnia symptoms |
| Kekäläinen et al. (2021) [ | Finland (high income) | Longitudinal (time differences) | 358 women (47-55 years) | Lockdown | Depressive symptoms, alcohol use |
| Koenders et al. (2021) [ | Netherlands (high income) | Ecological (time differences) | 36 patients with bipolar disorder | Lockdown | Depressive symptoms |
| Koenig et al. (2023) [ | Germany (high income) | Longitudinal (time differences) | 324 children and adolescents (≥12 years) | Lockdown | Depressive symptoms |
| Leatherdale et al. (2023) [ | Canada (high income) | Longitudinal (time differences) | 7,653 adolescents | Lockdown | Vaping |
| Lee et al. (2020) [ | United States (high income) | Longitudinal (time differences) | 546 young adults | Mitigation policies | Depressive symptoms, anxiety symptoms |
| Leightley et al. (2021) [ | United Kingdom, Spain, Netherlands (high income) | Longitudinal (time differences) | 252 individuals with MDD | Lockdown | Depressive symptoms |
| Liu et al. (2022) [ | United States (high income) | Longitudinal (time differences) | 175 adolescents | Stay-at-home orders | Depressive symptoms |
| Macfarlane et al. (2021) [ | United Kingdom (high income) | Re-surveyed cohorts (time differences) | 1,054 individuals with musculoskeletal disease | National lockdown | Depressive symptoms, anxiety symptoms, insomnia symptoms |
| Mauz et al. (2023) [ | Germany (high income) | Longitudinal (time differences) | 26,152 adults (18+) | Lockdown | Depressive symptoms |
| Meda et al. (2021) [ | Italy (high income) | Longitudinal (time differences) | 358 university students | COVID-19 lockdown | Depressive symptoms, anxiety symptoms |
| Minhas et al. (2021) [ | Canada (high income) | Longitudinal (time differences) | 473 emerging adults | Lockdown | Depressive symptoms, anxiety symptoms, alcohol use |
| Moya et al. (2021) [ | Colombia (low or middle income) | Longitudinal (time differences) | 1,376 primary caregivers | National lockdown | Depressive symptoms, anxiety symptoms |
| Murphy et al. (2023) [ | United States (high income) | Longitudinal (time differences) | 204 individuals from three generations | Lockdown and social distancing | Depressive symptoms, anxiety symptoms |
| Overbeck et al. (2021) [ | Denmark (high income) | Cross-sectional (time differences) | 1,758 pregnant women | COVID-19 lockdown | Depressive symptoms, anxiety symptoms |
| Pelham et al. (2022) [ | United States (high income) | Longitudinal (time differences) | 494 adolescents (12-21 years) | Stay-at-home orders | Alcohol use, tobacco use |
| Rimfeld et al. (2022) [ | England and Wales (high income) | Longitudinal (time differences) | 4,773 individuals | Lockdown | Depressive symptoms, anxiety symptoms |
| Romdhani et al. (2022) [ | 49 countries | Cross-sectional (time differences) | 3,911 athletes | Lockdown | Insomnia symptoms |
| Sacre et al. (2021) [ | Australia (high income) | Cross-sectional (time differences) | 450 adults with type 2 diabetes | Lockdown | Depressive symptoms, anxiety symptoms |
| Shoshani et al. (2021) [ | Israel (high income) | Cross-sectional (time differences) | 1,537 students (5th-11th grade) | Lockdown | Depressive symptoms, anxiety symptoms |
| Tanaka et al. (2021) [ | Japan (high income) | Longitudinal (time differences) | General population | State of emergency | Suicide |
| van der Velden et al. (2022) [ | Netherlands (high income) | Population-based (time differences) | 740 adults | Lockdown | Depressive symptoms, Post-traumatic stress symptoms |
| van den Besselaar et al. (2021) [ | Netherlands | Longitudinal (time differences) | 1,128 older adults | Social distancing measures | Depressive symptoms, anxiety symptoms |
| Yang et al. (2021) [ | China (low or middle income) | Longitudinal (time differences) | 195 college students | Lockdown | Depressive symptoms |
| Zijlmans et al. (2023) [ | Netherlands (high income) | Longitudinal (time differences) | 2,401 children (8-18 years) | Lockdown | Depressive symptoms, anxiety symptoms, insomnia symptoms |
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risks with no government lockdown | Risks with government lockdown | |||||
| Depressive symptom severity | - | SMD 0 SD (0.08 lower to 0.09 higher) | - | 10,743 (8 non-randomized studies) | ⊕⊝⊝⊝ Very lowa,b | The evidence about the effect of government lockdown on depressive symptoms is very uncertain. |
| Suicide | Acharya et al. (2022) [ | - | Two non-randomized studies | ⊕⊝⊝⊝ Very lowc,d,e | The evidence about the effect of government lockdown on suicide rates is very uncertain. We conducted a narrative synthesis because the overall risk of bias in the two included studies, assessed by ROBINS-I, was critical. | |
| Potential sources | Included study (n = 8)* | Estimated SMD (95% CI) |
| Clinical heterogeneity | ||
| Age group‡ | Adolescent (n = 1) | 0.12 (-0.20 to 0.45) |
| Country income level** | High-income countries (n = 7) | -0.04 (-0.36 to 0.29) |
| Methodological heterogeneity (the presence or absence of adjustment for confounding factors) | ||
| Occupation | Adjusted (n = 4) | 0.10 (-0.10 to 0.29) |
| Economic status | Adjusted (n = 3) | 0.00 (-0.22 to 0.21) |
| Relationship status | Adjusted (n = 5) | 0.00 (-0.21 to 0.22) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Psychological Well-being and Life Satisfaction · COVID-19 Pandemic Impacts
Introduction and background
The coronavirus disease (COVID-19) pandemic (i.e., an epidemic that spreads across several countries or continents and affects a large number of people) began in December 2019 and led to the implementation of government lockdowns in many countries to curb the spread of the infection. Beyond its physical health consequences, the pandemic has also highlighted how outbreaks of emerging infectious diseases can significantly impact mental health. For instance, the severe acute respiratory syndrome (SARS) epidemic (i.e., an unexpected increase in the number of disease cases within a specific geographical area) was associated with symptoms of post-traumatic stress disorder (PTSD) and depression in the general population [1]. Similarly, the COVID-19 pandemic has resulted in reduced psychological well-being and increased symptoms of anxiety and depression [2]. These mental health outcomes may result from multiple factors, including fear of infection, grief due to illness or loss of relatives and acquaintances, and restrictions such as lockdowns or quarantine (i.e., the separation and restriction of movement of individuals who may have been exposed to a contagious disease) to prevent disease spread.
Non-pharmacological public health measures have been primary strategies in controlling not only the COVID-19 outbreak but also other emerging infectious diseases such as Ebola, Middle East respiratory syndrome (MERS), and influenza A (H1N1) [3-5]. Lockdowns (defined as large-scale government directives requiring individuals to stay at home and to refrain from, or limit, activities outside the home) have been widely adopted to reduce COVID-19 transmission [6]. Various governments have used different terms to describe the lockdown, including stay-at-home orders and movement control orders [7-9]. The extent and enforcement of lockdown measures varied across countries; some were mandatory, while others were voluntary. For example, in April 2022, the Japanese government declared a state of emergency due to the COVID-19 endemic (i.e., an outbreak consistently present but limited to a particular region), but this order was not mandatory [10]. In contrast, other countries enforced penalties for violations of lockdown regulations [11]. Given that lockdowns can disrupt employment and the ability to work, several governments provided direct economic and social assistance (such as public wage subsidies, price controls, distribution of goods, or a combination) to mitigate financial burdens [12]. Overall, lockdowns have played an effective role in controlling the spread of COVID-19 [13,14].
Forced and strict isolation measures, such as lockdowns or quarantines, can negatively impact mental health [15,16]. Lockdowns often result in reduced educational opportunities and the suspension of economic or cultural activities. With the closure of schools or the transition to online learning, some students may abandon higher education due to increased anxiety about academic performance [17]. In addition, the downturn in economic activities associated with lockdowns can lead to unemployment and heightened financial concerns [18]. At the same time, the cessation of various cultural activities may impact the well-being and quality of life of many individuals, including the elderly [19,20].
A systematic review has demonstrated that quarantine can adversely affect mental health outcomes [21]. Although both quarantine and lockdown involve isolation, their mental health impacts may differ due to variations in the populations affected, the scale of implementation, and the duration of isolation. The impact of lockdown on individuals and society as a whole is likely to be significant. Several studies have reported on the mental health impacts of government lockdowns during the COVID-19 pandemic [16,22,23]. However, comprehensive evidence regarding the long-term mental health consequences of lockdowns in the general population remains limited. Therefore, we conducted this review to evaluate the effects of government lockdowns during emerging infectious disease outbreaks on the mental health of the general population. This evidence may be instrumental for policymakers in preparing for future public health emergencies.
Review
Methods
This review was conducted in accordance with the methodological standards outlined in the Cochrane Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary material 1) [24,25]. This review protocol was registered in the Cochrane Library [26].
Difference Between Protocol and Review
The following terminologies in this review were revised: “primary outcome” was changed to “critical outcome” and “secondary outcome” to “important outcome.” Consequently, in the “Certainty of the Evidence Assessment” section, what was previously referred to as “important outcomes” in the protocol is now termed “critical outcomes” in this review.
When multiple instruments measured the same outcome, we had planned to select the instruments of outcomes of interest that came first in our list in our protocol. However, studies that measured outcomes using multiple instruments were not identified.
In the before-and-after comparison design, we measured all the outcomes of interest in the control group (i.e., no government lockdown) during the period immediately preceding the intervention.
We excluded studies that compared periods of government lockdowns with post-lockdown periods, regardless of whether the lockdowns were lifted.
We conducted a literature search in the following electronic databases: Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE Ovid, PsycINFO Ovid, the US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov), and the WHO International Clinical Trials Registry Platform (ICTRP). The search strategy outlined in the protocol yielded a large number of search results. After consultation with Cochrane information specialists, we excluded Embase Ovid from the electronic database search due to practical considerations in conducting the review.
Although we had initially planned to assess the risk of bias in randomized controlled trials (RCTs) using the RoB 2 tool, this was not applicable, as there were no RCTs included. Furthermore, while we intended to conduct a separate meta-analysis and present the risk of bias for emerging infectious diseases, our search only yielded reports of lockdowns during the COVID-19 outbreak; therefore, we limited our review to this topic.
We could not carry out the planned subgroup analyses and sensitivity analyses due to limited data and the small number of included studies.
We assessed the publication bias based on unpublished studies in clinical trial registries and published protocols that were identified by a full-text screening because we could not assess publication bias using funnel plots.
Study Settings and Designs
We included RCTs and non-randomized studies of interventions (NRSIs) to investigate the impact of government lockdowns on mental health during outbreaks of emerging infectious diseases, including SARS, MERS, COVID-19, H1N1, equine influenza, avian influenza, and Ebola virus disease. Studies with design features outlined in the Appendices [27] were eligible for inclusion. We did not apply restrictions based on language, country of origin, year of publication, or publication status. Although our protocol initially planned for the inclusion of RCTs and studies conducted during outbreaks of emerging infectious diseases other than COVID-19, ultimately, only NRSIs conducted during the COVID-19 pandemic were identified.
Eligibility Criteria of Study Participants and Interventions
We included adults (aged 20 years and older) and adolescents (aged 10 years and older), irrespective of comorbidities, and infants and children were excluded. For studies that evaluated a general population and reported the age of study participants, we contacted the original study authors to obtain information on participants by age groups and outcomes of interests. When this was not possible, we categorized the study to have enrolled adults if ≥80% of the study participants were aged 20 years and older.
We included government lockdowns during emerging infectious disease outbreaks and excluded studies on terrorism, war, and natural or humanitarian disasters. We defined government lockdowns as national or regional isolation, as directed by the government, regardless of the individuals' exposure or likelihood of exposure to an emerging infectious disease. We accepted the definition of government lockdowns used by the study investigators. The comparator was no government lockdown. We excluded studies that compared periods of government lockdowns with post-lockdown periods, regardless of whether the lockdowns were lifted. We excluded studies on voluntary or mandatory quarantine because of infection by, or exposure to, an emerging infectious disease.
Outcome Measures
We assessed depressive symptom severity and suicide as critical outcomes. We defined suicide as death caused by a fatal self-injurious act, with some evidence of intent to die. We also assessed anxiety symptom severity, PTSD symptom severity, insomnia symptom severity, and substance use as important outcomes. We measured all of the above outcomes, except for suicide, at the longest follow-up within 12 months. Studies have suggested that a short follow-up duration (less than 12 months) after the intervention may not be enough to change the prevalence of suicide [28]. Thus, we measured the outcome of suicide at the longest follow-up within 24 months. In the before-and-after comparison design, we measured all of the above outcomes in the control group during the period immediately preceding the intervention. Regarding depressive symptom severity, we accepted the following assessment instruments for the measurement of depressive symptoms: (1) Patient Health Questionnaire-9 [29], (2) Beck's Depression Inventory [30], or other validated scales. Regarding anxiety symptom severity, we accepted the following assessment instruments for measuring anxiety symptoms: (1) Generalized Anxiety Disorder-7 [31], (2) Brief Fear of Negative Evaluation Scale [32], or other validated scales. Regarding PTSD symptom severity, we accepted the following assessment instruments for measuring PTSD symptoms: (1) Impact of Event Scale-Revised [33], (2) Impact of Event Scale [34], or other validated scales. Regarding insomnia symptom severity, we accepted the following clinical diagnostic instruments for measuring insomnia symptoms: (1) Pittsburgh Sleep Quality Index [35], (2) Insomnia Severity Index [36], or other validated scales. Regarding substance use, we measured substance use by the difference in the amount of substance use before and after the intervention. We focused on the following substances: (1) alcohol, (2) tobacco, (3) vape, and (4) cannabis. When multiple instruments measured the same outcome in the included studies, we selected the one that came first in our list.
Information Sources and Search Strategy
The following electronic databases were searched on April 11, 2022: (1) CENTRAL; (2) Medline Ovid; (3) PsycINFO Ovid; (4) US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov); and (5) WHO ICTRP. We describe the full search strategies in Supplementary material 2. We checked the reference lists of all included studies and relevant systematic reviews to identify additional studies missed during the original electronic searches. We also run a cited reference search in citation indexes of the Web of Science and Google Scholar. We contacted the authors of identified studies and asked them to identify other relevant published and unpublished studies. We conducted a literature search to identify all published and unpublished RCTs and NRSIs, including quasi-RCTs, non-randomized cross-over studies, prospective cohort studies, retrospective cohort studies, controlled before and after studies, interrupted time series (with comparison group), and cross-sectional studies in all languages. We translated non-English articles and thoroughly assessed them for potential inclusion as necessary.
Selection Process, Data Collection Process, and Data Items
Two pairs of four review authors (YO, KY, NS, TA) independently screened the titles and abstracts of search results, and they reviewed the full texts independently and identified studies for inclusion. Disagreements were resolved by discussion or by consulting other review authors (YT, ST, MB, YK). We recorded the reasons for the exclusion of ineligible full-text studies. We excluded all duplicate publications. When we found multiple reports/publications of the same study, we checked them to ensure that each study, rather than each report/publication, was the unit of interest in the review. Two pairs of seven review authors (YO, NS, TA, YT, ST, MB, YK) extracted study characteristics and outcome data from the included studies. They entered this information into a data collection form that we had specifically piloted for this review. Two pairs of eight review authors (YO, KY, NS, TA, YT, ST, MB, YK) transferred data to the Review Manager [37] and recorded the following data for the included studies. We also extracted the results regarding the following variables. For continuous outcomes (depressive symptom severity, anxiety symptom severity, PTSD symptom severity, insomnia symptom severity, and substance use), we extracted the mean value and standard deviation (SD) of the outcome of interest before and after the intervention. For dichotomous outcomes (suicide), we extracted the number of participants in each intervention arm who had the measured outcome of interest and the number of participants assessed at the endpoint. While we had planned to extract both crude odds ratios (ORs) and adjusted ORs at the endpoint, we did not identify any studies that reported these effect sizes.
Study Risk of Bias Assessment
Two pairs of seven review authors (YO, NS, TA, YT, ST, MB, YK) independently assessed the risk of bias for each outcome of interest in this review. Disagreements were resolved by discussion or by consulting other review authors (YT, ST, MB, YK). We were interested in assessing the risk of bias for the effect of assignment to the intervention. To assess the risk of bias in NRSIs, we used the "Risk Of Bias In Non-randomized Studies - of Interventions" (ROBINS-I) tool [38]. We judged each potential source of bias as having "low," "moderate," "serious," or "critical" bias or "no information." We summarized the risk of bias judgments across different studies for each of the domains listed and provided an overall risk of bias judgment in the "risk of bias" table.
Effect Measures and Synthesis Methods
We conducted a statistical analysis using the Review Manager [37]. We conducted a meta-analysis using a random-effects model if clinically similar studies were available to ensure meaningful conclusions. We excluded studies at an overall critical risk of bias from the meta-analysis based on the recommendation of ROBINS-I [38]. For continuous data, when studies used the same continuous outcome measure for comparison, we pooled data by using an adjusted mean difference (MD). We used the standardized mean difference (SMD) to pool data from studies that measure the same outcomes of interest using different methods. We presented 95% confidence intervals (CIs) and point estimates. For suicide, we conducted a narrative synthesis due to methodological heterogeneity because we had planned to conduct a meta-analysis only when pooling to make sense and based on the recommendation of ROBINS-I [38]. We displayed the results of studies that reported that no events occurred for an outcome in the forest plot; however, it did not contribute to the effect size.
Unit of Analysis Issues
The unit of analysis was individual participants included in the studies. For included studies that should consider individuals as cluster factors, we assessed whether the clustering effect had been dealt with effectively in the analysis of the included studies. When the original authors used a statistical model such as a mixed-effects model or generalized estimating equations to take the clustering effects into account, we chose it as the estimate for the synthesis. We critically appraised the cluster-level confounding through the confounding domain of the ROBINS-I tool [38]. For studies with multiple comparisons, we included all intervention groups that were assessed to be relevant to this review as per our pre-defined eligibility criteria.
Dealing With Missing Data
We contacted authors to verify key study characteristics and obtained missing numerical outcome data. However, we were unable to obtain the data from all the authors that we contacted. We used the median as the mean and calculated the SD from the standard error, interquartile range, or p-values, according to the Cochrane Handbook for Systematic Reviews of Interventions [39], and when we were unable to calculate the SD in this way, we imputed the SD as the median SD in the remaining studies included in the outcome. We assessed the impact of included studies with missing data in a sensitivity analysis. We excluded studies from which we could not obtain and impute sufficient data to synthesize, based on the criterion of "no appropriate data."
Reporting Bias Assessment
We aimed to assess the possibility of publication bias through funnel plot analysis; however, this was not feasible, as fewer than 10 studies satisfied this review's inclusion criteria. Therefore, we assessed reporting bias as publication bias based on unpublished studies in clinical trial registries and published protocols that were identified by a full-text screening.
Investigation of Heterogeneity and Subgroup Analysis
We conducted a univariate meta-regression analysis to explore the relationship between the critical outcome (i.e., depressive symptom severity) and the potential sources of heterogeneity. Potential sources of clinical heterogeneity examined included age groups (i.e., adolescents (aged 10 years and older) versus adults (aged 20 years and older)) and country income levels (i.e., high-income countries versus low- or middle-income countries). For methodological heterogeneity, the presence or absence of adjustment for confounding factors (i.e., occupation, economic status, and relationships) was considered. We conducted the analysis using the metafor package, Version 4.4-0, in R software, Version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria, https://www.R-project.org/). We tabulated the results from the meta-regression analysis. We evaluated the assumptions of the meta-regression using residual plots, Cook’s distance, and visual inspection of moderator linearity. Due to the limited number of included studies and the lack of sufficient information on government lockdowns, we were unable to perform the meta-regression analysis for suicide outcomes or for depressive symptom severity based on the following potential sources of heterogeneity: the duration of government lockdowns, enforcement of lockdowns with penalties for non-compliance, provision of public subsidies for wages during lockdowns, methods of allocation to study groups, and overall risk of bias. We also assessed statistical heterogeneity by calculating the I^2^.
Sensitivity Analysis
We conducted a sensitivity analysis for the critical outcomes by excluding studies with imputed data. Due to the limited number of studies included and the lack of information, we could not conduct sensitivity analysis for suicide and for depressive symptom severity under the condition that studies classified as having an overall serious risk of bias were excluded. In addition, we could not conduct a responder analysis for both outcomes.
Certainty of the Evidence Assessment
We summarized the body of evidence for critical outcomes using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system [40]. Using the GRADEpro software, we created a "summary of findings" table for summarizing outcome-specific information. To inform the GRADE levels of evidence, we used the overall risk of bias evaluated by ROBINS-I because we identified only NRSIs in our review.
Results
A total of 8,079 records were identified from the electronic database search, and 3,083 records were identified from the citation search. We retrieved full texts of 603 reports from the electronic database and 92 reports from citation searches for full assessment. Of these 695 full-text articles, we included 42 studies in our review (Figure 1). We excluded 653 reports (Supplementary material 3) and identified 24 ongoing studies (Supplementary material 4).
PRISMA flow diagram
Characteristics of Included Studies
Of the 42 studies that met our review criteria, all the included studies were NRSIs (Table 1; Supplementary material 5) [41-82].
All the included studies assessed the impact of the COVID-19 pandemic on mental health outcomes. Key study design features (i.e., how groups of individuals or clusters were formed) in all included studies were time differences. Among the 42 studies, we found that the study participants were from the general population in 27 studies [41-46,49-52,54,55,58,59,62,63,65,67-70,73,77,78,80-82]. Interventions were explicitly defined as "lockdown" in 33 studies [41-43,45,46,48-55,57,59-62,64,66-72,74-77,79,81,82], and as "stay-at-home order" in four studies [44,58,65,73]. We identified 21 studies that reported government lockdown periods exceeding one month [43,45-51,53,56,59,60,62,64-66,68,72,76,80,82]. A total of 27 studies reported on depressive symptom severity [45,46,48,49,54,56,58-61,63-72,74,76,77,79-82], 2 on suicide [41,78], 20 on anxiety symptom severity [43,45,46,49,50,56-58,63,66,68-72,74,76,77,79,82], 2 on PTSD symptom severity [47,79], 8 on insomnia symptom severity [51-53,57,58,66,75,82], and 9 on substance use [42,44,45,50,55,59,62,69,73].
Excluded Studies
We excluded a total of 653 full-text studies. For the electronic database search, we excluded 576 studies due to the following reasons: unpublished (N = 24), ineligible study design (N = 326), ineligible population (N = 5), ineligible intervention (N = 31), ineligible control (N = 33), ineligible outcomes (N = 127), no appropriate data (N = 15), and other reasons (e.g., narrative review) (N = 15). For the citation research, we excluded 77 studies due to ineligible design (N = 39), ineligible intervention (N = 13), ineligible outcomes (N = 18), no appropriate data (N = 6), and other reasons (N = 1). We describe the reasons for exclusions and the characteristics of 629 excluded studies in Supplementary material 3.
Risk of Bias Assessment for Critical Outcomes
We summarize the risk of bias for depressive symptom severity in Figure 2, and a detailed risk of bias assessment is provided in Supplementary material 6.
Risk of bias assessment using the ROBINS-I for depressive symptom severity
Nine studies had an overall serious risk of bias [45,48,55,59,61,69-72], and 18 studies had an overall critical risk of bias [46,49,56,58,60,63-68,74,76,77,79-82]. For suicide, two studies had an overall critical risk of bias (Figure 3; Supplementary material 7) [41,78].
Risk of bias assessment using the ROBINS-I for suicide
Risk of Bias Assessment for Important Outcomes
For anxiety symptom severity, six studies had an overall serious risk of bias [45,54,69-72], while 14 studies had an overall critical risk of bias (Supplementary materials 8 and 9) [43,46,49,56-58,63,66,68,74,76,77,79,82]. For PTSD symptom severity, one study had an overall serious risk of bias [47], while other studies had an overall critical risk of bias (Supplementary materials 10 and 11) [79]. For insomnia symptom severity, two studies had an overall serious risk of bias [51,52], and six studies had an overall critical risk of bias (Supplementary materials 12 and 13) [53,57,58,66,75,82]. For substance use, five studies had an overall serious risk of bias [44,45,50,59,69], and four studies had an overall critical risk of bias (Supplementary materials 14 and 15) [42,55,62,73].
Synthesis of Critical Outcomes
Among the 27 included studies that reported depressive symptom severity, 18 studies were excluded from the meta-analysis due to an overall critical risk of bias as per our protocol [26]. Government lockdowns may have little to no effect on depressive symptom severity within the 12-month follow-up, but the evidence was very uncertain (SMD 0.00, 95% CI -0.08 to 0.09, I^2^ = 70%; 8 studies, 10,743 participants) (Figure 4; Table 2).
Government lockdown versus no government lockdown during the COVID-19 pandemic: depressive symptom severityWe pooled the standardized mean difference (SMD) in eight studies. The study by Cohen et al. (2021) [54] was not included in the meta-analysis because the SMD could not be estimated due to zero scores in both the intervention and control groups.
Table 3 shows the result from a univariate meta-regression analysis assessing the heterogeneity based on age groups, country income levels, and adjustment for confounding factors (i.e., occupation, economic status, and relationship status).
For the clinical heterogeneity, the estimated SMD was as follows: 0.12 (95% CI -0.20 to 0.45) for age groups and -0.04 (95% CI -0.36 to 0.29) for country income levels. For the methodological heterogeneity, the estimated SMD was as follows: 0.10 (95% CI -0.10 to 0.29) for occupation, 0.00 (95% CI -0.22 to 0.21) for economic status, and 0.00 (95% -0.21 to 0.22) for relationship status. For the sensitivity analysis by excluding studies with imputed data, we pooled SMD of five studies [45,59,61,70,72]. Government lockdowns may have little to no effect on depressive symptom severity within the 12-month follow-up (SMD -0.02, 95% CI -0.12 to -0.08, I^2^ = 73%; 5 studies, 7,746 participants) (Figure 5). These findings were consistent with the result of the main analysis.
Sensitivity analysis. Government lockdown versus no government lockdown during the COVID-19 pandemic: depressive symptom severity
Regarding suicide, we presented a narrative synthesis of two studies as a summary of findings in Table 2. Acharya et al. showed that government lockdowns may have a negative impact on suicide at 15-month follow-up (incidence rate ratio (IRR) 1.33, 95% CI 1.2-1.48) [41]. Tanaka et al. showed that government lockdowns may also have a negative impact at 3- to 6-month follow-up (IRR 1.16, 95% CI 1.11-1.21) [78]. However, these two studies had an overall critical risk of bias, and we judged the evidence on this outcome as very low certainty.
Synthesis of Important Outcomes
Among the 20 included studies that reported anxiety symptom severity, we pooled SMD in only five studies, except for exclusion, due to an overall critical risk of bias [45,69-72]. The study by Cohen et al. was not included in the meta-analysis because the SMD could not be estimated due to zero scores in both the intervention and control groups [54]. Government lockdowns may have little to no effect on anxiety symptom severity within the 12-month follow-up (SMD 0.08, 95% CI -0.10 to 0.26; I^2^ = 91%; 5 studies, 10,471 participants) (Supplementary material 16A), but the evidence was very uncertain.
Two studies reported PTSD symptom severity [47,79]. Berthelot et al. showed that government lockdowns may increase the outcome within the 12-month follow-up (MD 0.18, 95% CI 0.08-0.28; 1 study, 1,754 participants) (Supplementary material 16B), but the evidence was very uncertain [47].
Among the eight included studies that reported insomnia symptom severity, we pooled MD in two studies [51,52]. Government lockdowns may increase the outcome within the 12-month follow-up (MD 1.28, 95% CI 0.62-1.94; I^2^ = 91%; 2 studies, 5,142 participants) (Supplementary material 16C), but the evidence was very uncertain.
Among the nine included studies that reported on the amount of substance use, we pooled SMD in five studies that reported on alcohol [44,45,50,59,69]. Government lockdowns may have little to no effect on the outcome within the 12-month follow-up (SMD 0.03, 95% CI -0.05 to 0.11; I^2^ = 66%; 5 studies, 8,261 participants) (Supplementary material 16D), but the evidence was very uncertain. We considered two studies that reported on tobacco [42,73]: Leatherdale et al. who reported on vape use [62] and Cousijn et al. who reported on cannabis as having an overall critical risk of bias [55]. Therefore, these outcomes were not pooled in our review due to the limited number of studies.
Reporting Biases
We identified 24 ongoing studies (Supplementary material 4). In addition, we found two published protocols that were identified by a full-text screening [83,84]. However, one protocol was not published as an original article [84].
Discussion
This review assessed the impact of government lockdowns on mental health in the general population during outbreaks of emerging infectious diseases. Only studies during the COVID-19 outbreak met the inclusion criteria in our review. Overall, we found no evidence of the impact of government lockdown on mental health during the outbreak of emerging infectious diseases. Government lockdowns during the COVID-19 outbreak may have little to no effect on the depressive symptom severity in the general population; however, this evidence is very uncertain. In addition, the evidence about the impact of government lockdowns on suicide was very uncertain. The evidence about the impact on important outcomes was also very uncertain.
Interpreting the results of this review requires considering the follow-up period following the initiation of a government lockdown. Multiple lockdowns were implemented in various countries during the COVID-19 pandemic, and we did not examine the cumulative impact (i.e., the intensity of lockdowns) in this review. Individuals who experienced multiple lockdowns may have been more affected in terms of mental health; however, it is also possible that the acute stress response to lockdowns and the pandemic may have diminished over time, leading to a reduction in mental health impacts. In this review, among the pooled studies that reported depressive symptom severity, four studies [45,48,70,72] had follow-up periods of up to two months, and four studies [54,59,61,69] had follow-up periods ranging from two to six months, suggesting that the pooled effect size may predominantly reflect outcomes within six months from the start of lockdowns.
Two existing systematic reviews addressed a similar scope during the COVID-19 outbreak [85,86]. One review reported that the impact on mental health was not negligible [85], while another reported an initial increase in the average symptoms of depression and anxiety after the lockdown [86]. Potential reasons for the discrepancies may be attributed to differences in the included studies and the varying timing of outcome measurements after the lockdown. While this review only incorporated studies that adjusted for confounders affecting outcomes to mitigate the risk of bias inherent in unadjusted studies, the other two reviews were not restricted to such studies. Moreover, this review encompassed studies of the general population regardless of comorbidities. Concerning the timing of outcome measurements, one review encompassed only studies conducted between 1 and 60 days post-lockdown initiation [85]. Another review, which had the same observation period as ours, reported that the average symptoms of anxiety and depression worsened up to two months post-lockdown. However, the impact of the lockdown remained uncertain for periods extending beyond three months after the lockdown [86]. It is possible that the impact of government lockdowns on mental health may not elicit a uniform response among individuals after more than two months have passed since the initiation. This variability could depend on the magnitude of an individual's stress response and their specific circumstances.
Regarding emerging infectious diseases other than COVID-19, there was no evidence of the impact of government lockdowns. Non-pharmacological public health policy interventions are often implemented to control the spread of emerging infectious diseases, and lockdown is one such measure. However, despite extensive searches using various terms related to lockdown, there were no studies that investigated the mental health impacts of lockdown during outbreaks of SARS, MERS, H1N1, equine influenza, avian influenza (e.g., H7N9), or Ebola virus disease, leaving the effects of such interventions on mental health unclear. Therefore, we were not able to compare the effect of government lockdowns between emerging infectious diseases.
We could not find any studies that examined the impact of government lockdowns that mitigated the impact of the COVID-19 pandemic. In other words, we were unable to examine the impact of lockdown alone on mental health; during outbreaks of emerging infectious diseases such as COVID-19, where lockdown occurs at the time of spread, the effect may be due to both the lockdown and the pandemic [85]. An ideal study design would compare an area under government lockdown during an emerging infectious disease outbreak with another area without government lockdown but in a comparable epidemic state. While practically challenging, such a comparison would require not only confounding adjustments but also refined study design to truly examine the impact of government lockdowns.
The duration of the government lockdown was unclear in 20 studies, and the pre-specified co-interventions were not described in 41 studies. While this intensity and duration should be considered when examining the effects of lockdowns, many of the studies included in this review did not provide sufficient information. During an outbreak of emerging infectious diseases, it may be difficult to measure the effect of a uniform intervention due to the global spread of the disease and the different modalities of each lockdown in different countries.
The timing of measurement of outcomes in no government lockdown was varied. We defined the control group as the period immediately prior to the lockdown, while some included studies used several years prior to the lockdown as the control group. It is possible that local and global situations at this time (e.g., economic or political situations) may have affected the mental health of individuals, making it an inappropriate time for the control group. In that sense, comparisons between groups that underwent lockdowns and those that did not may be preferable as a design than comparative studies before and after lockdown (e.g., longitudinal studies).
The included studies in this review had an overall serious or critical risk of bias. Although 42 studies met our review criteria, only a limited number were adjusted for three pre-specified confounders. Using the ROBINS-I tool, we judged these studies to have an overall critical risk of bias when all pre-specified confounders were not adjusted. Consequently, we could not synthesize the effect sizes of these studies in a meta-analysis.
In our investigation of the heterogeneity of critical outcomes, we found inconsistent results across different assessments of heterogeneity. Although the meta-analysis shows substantial statistical heterogeneity regarding I^2^ among the included studies on depressive symptom severity, we could not identify the source of clinical and methodological heterogeneities by our meta-regression.
Several limitations should be considered when interpreting the findings of this review. First, we excluded the Embase database as part of our systematic literature search. Consequently, there is a risk that some relevant studies may have been missed. Nevertheless, the volume of research that required screening was substantial, and including Embase would have been impractical for the scope of this review. Second, we were unable to conduct all planned analyses, particularly subgroup and sensitivity analyses, due to insufficient data. In addition, it is important to note that for the subgroup analyses of depressive symptom severity, we had to exclude two studies due to a lack of sufficient data. Third, many studies were excluded due to "ineligible study design" in the before-and-after studies that did not adjust for confounding factors. Many studies reported the impact of government lockdowns on mental health during the COVID-19 outbreak, but we included and pooled data from studies that met a strict criterion in this review. Finally, we could not quantitatively evaluate reporting bias as per the protocol and instead had to consider the potential for publication bias qualitatively.
Conclusions
Available evidence suggests that the impacts of government lockdowns on mental health in the general populations are very uncertain. While the social benefits of implementing government lockdowns to prevent the spread of emerging infectious diseases are evidently substantial, the potential adverse effects on mental health may not be taken into account. Future studies should employ rigorous research design, including comparisons between areas with and without government lockdowns during outbreaks, to provide stronger evidence. These studies should also consider the intensity of lockdowns, associated compensation measures, and potential confounders such as socioeconomic status, occupation, and relationships. Systematic reviews that include studies employing rigorous research designs with a low risk of bias will yield more trustworthy conclusions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1SARS control and psychological effects of quarantine, Toronto, Canada Emerg Infect Dis Hawryluck L Gold WL Robinson S Pogorski S Galea S Styra R 120612121020041532453910.3201/eid 1007.030703 PMC 3323345 · doi ↗ · pubmed ↗
- 2COVID-19 pandemic and mental health consequences: systematic review of the current evidence Brain Behav Immun Vindegaard N Benros ME 5315428920203248528910.1016/j.bbi.2020.05.048PMC 7260522 · doi ↗ · pubmed ↗
- 3Community quarantine to interrupt ebola virus transmission-Mawah village, Bong County, Liberia, August-October, 2014 MMWR Morb Mortal Wkly Rep Nyenswah T Blackley DJ Freeman T 179182642015 https://www.cdc.gov/mmwr/preview/mmwrhtml/mm 6407 a 4.htm 25719679 PMC 5779591 · pubmed ↗
- 4Public health measures during the influenza A(H 1N 1)2009 pandemic 3 2025 World Health Organization(2011 2010 https://www.who.int/publications/i/item/public-health-measures-during-the-influenza-a(h 1n 1)2009-pandemic
- 5Infection prevention and control during health care for probable or confirmed cases of Middle East respiratory syndrome coronavirus (MERS-Co V) infection 3 2025 World Health Organization(2015 2015 https://www.who.int/publications/i/item/10665-174652
- 6Poli Map: a taxonomy proposal for mapping and understanding the global policy response to COVID-19Open Science Framework Peña S Cuadrado C Rivera-Aguirre A 1332020 https://osf.io/preprints/osf/h 6mvs_v 1
- 7Comparison of estimated rates of coronavirus disease 2019 (COVID-19) in border counties in Iowa without a stay-at-home order and border counties in Illinois with a stay-at-home order JAMA Netw Open Lyu W Wehby GL 03202010.1001/jamanetworkopen.2020.11102 PMC 722952132413112 · doi ↗ · pubmed ↗
- 8Reducing onward spread of COVID-19 from imported cases: quarantine and 'stay at home' measures for travellers and returning residents to Singapore J Travel Med Chiew CJ Li Z Lee VJ 027202010.1093/jtm/taaa 049PMC 718436632297942 · doi ↗ · pubmed ↗