The Ticking Clock of Aortic Root Replacement - Single-Center Experience After Urgent and Emergent Aortic Root Replacement Using the BioIntegral and Freestyle™ Bioconduits
Konstantina Spetsotaki, Jingjing Shi, Ajay Moza, Matthias Menne, Ali Aljalloud

TL;DR
This study examines outcomes of urgent/emergency aortic root replacement surgeries using two bioconduits, finding similar clinical results but higher mortality in reoperative cases.
Contribution
The paper provides a single-center retrospective analysis of clinical outcomes using BioIntegral and Freestyle™ bioconduits in urgent/emergency aortic root replacement.
Findings
In-hospital and 30-day mortality rates were 15.4% among 26 patients.
Primary aortic root replacement was associated with significantly higher survival compared to redo cases.
Clinical outcomes were equal for both BioIntegral and Freestyle™ bioconduits.
Abstract
Aortic root pathologies needing full aortic root replacement are challenging entities correlated to high morbidity and mortality due to their complexity and mostly refer to high-risk patients. In this retrospective study, we report our surgical experience and clinical results of patients undergoing a Bentall procedure as primary or reoperative surgery with the application of aortic bioconduits. Patients who underwent full aortic root replacement utilizing either BioIntegral (BI) or Medtronic Freestyle™ (FS) bioconduit in the Cardiothoracic Surgery Department of the University Hospital Aachen RWTH from January 2015 until September 2020, in an urgent or emergency setting, were analyzed and followed up until December 2023. Twenty-six patients underwent aortic root replacement with bioconduits (N=11 with BI, N=15 with FS) in our center. Twenty-three cases were of infective cause, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
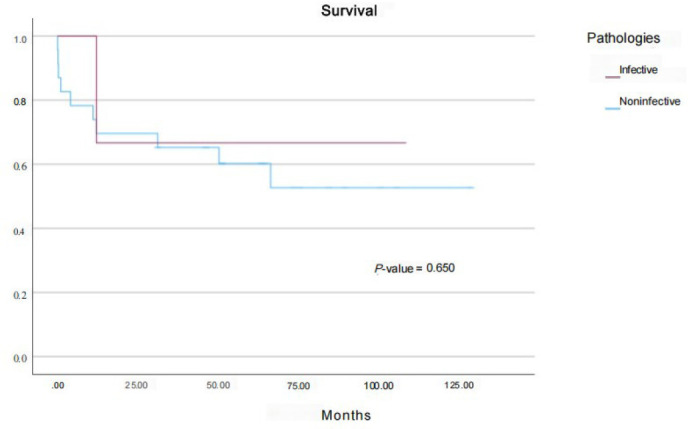 Figure 1
Figure 1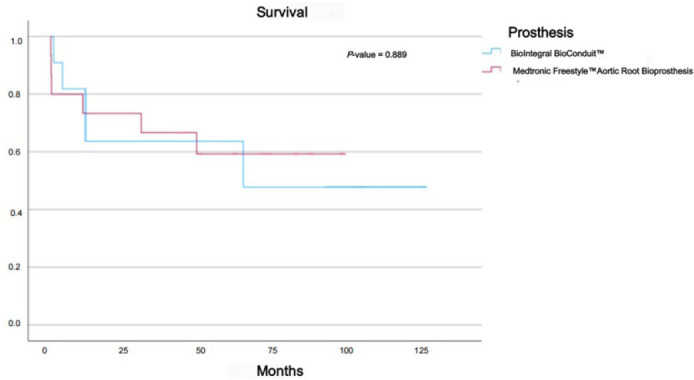 Figure 2
Figure 2| Abbreviations, Acronyms & Symbols | ||||
|---|---|---|---|---|
| AAR | = Ascending aorta replacement | IE | = Infective endocarditis | |
| AKI | = Acute kidney injury | LV | = Left ventricular | |
| AMC | = Aortomitral curtain | LSB | = Left septal block | |
| AMCR | = Aortomitral curtain reconstruction | MPG | = Mean pressure gradient | |
| AR | = Aortic root | MSSA | = Methicillin-susceptible
| |
| ARA | = Aortic root abscess | MVR | = Mitral valve repair | |
| ARR | = Aortic root replacement | MVRp | = Mitral valve replacement | |
| AV | = Aortic valve | PAOD | = Peripheral arterial occlusive disease | |
| AVR | = Aortic valve replacement | POD | = Postoperative day | |
| BI | = BioIntegra | PPG | = Peak pressure gradient | |
| BMI | = Body mass index | RCA | = Right coronary artery | |
| BSA | = Body surface area | ROSC | = Return of spontaneous circulation | |
| CABG | = Coronary artery bypass grafting | SCAAR | = Supracoronary ascending aorta replacement | |
| CPB | = Cardiopulmonary bypass | STS | = Society of Thoracic Surgeons | |
| EF | = Ejection fraction | TAPSE | = Tricuspid annular plane systolic excursion | |
| EuroSCORE II | = European System for Cardiac Operative Risk Evaluation | TAVI | = Transcatheter aortic valve implantation | |
| FS | = Freestyle™ | TVR | = Tricuspid valve reconstruction | |
| HLM | = Heart-lung machine | VT | = Ventricular tachycardia | |
| ICU | = Intensive care unit | |||
| Parameters | BI | FS | |
|---|---|---|---|
| Age at time of current surgery | 68.00 ± 16.66 | 58.13 ± 15.82 | 0.138 |
| Male sex | 9 (81.8%) | 12 (80%) | 0.907 |
| Height, m | 172.91 ± 7.61 | 175.20 ± 6.61 | 0.421 |
| Weight, kg | 78.00 ± 12.75 | 78.67 ± 9.47 | 0.879 |
| BMI, kg/m2 | 26.16 ± 4.85 | 25.61 ± 2.80 | 0.718 |
| BSA, m2 | 1.90 ± 0.18 | 1.94 ± 0.13 | 0.479 |
| PAOD | 1 (9.1%) | 2 (13.3%) | 0.738 |
| EuroSCORE II | 23.76 ± 24.40 | 11.53 ± 10.91 | 0.097 |
| STS score | 4.84 ± 6.25 | 1.58 ± 0.71 | 0.048 |
| Previous cardiac surgery | 7 (63.6%) | 9 (60%) | 0.851 |
| Previous aortic surgery | 0.343 | ||
| Previous Bentall procedure | 1 (9.1%) | 2 (13.3%) | |
| Previous David procedure with hemiarch | 0 (0%) | 1 (5.7%) | |
| Previous David procedure | 1 (9.1%) | 0 (0%) | |
| Previous SCAAR by type A dissection | 1 (9.1%) | 0 (0%) | |
| Aortic valve | 0.908 | ||
| Native | 5 (45.4%) | 5 (33.3%) | |
| Previous AV prosthesis | 4 (36.4%) | 7 (46.7%) | |
| Previous AR conduit | 1 (9.1%) | 2 (13.3%) | |
| Previous David procedure, preserved AV | 1 (9.1%) | 1 (6.6%) | |
| ARA presence | 0.599 | ||
| ARA | 7 (63.6%) | 8 (53.3%) | |
| Non-ARA | 4 (36.4%) | 7 (46.7%) | |
| Redo surgery (year after last cardiac surgery) | 4.33 ± 6.92 | 2.13 ± 2.07 | 0.329 |
| Embolic complications before surgery | 0.325 | ||
| Νone | 11 (100%) | 11 (73.3%) | |
| Pulmonary septic embolic complications due to IE | 0 (0%) | 2 (13.3%) | |
| Kidney, spleen, and cerebral septic embolic | 0 (0%) | 1 (6.7%) | |
| Limb and intestinal ischemia due to septic | 0 (0%) | 1 (6.7%) | |
| Main diagnosis | 0.944 | ||
| Native AR IE + ARA | 2(18.2%) | 2 (13.3%) | |
| Native AV IE without ARA | 2 (18.2%) | 1 (6.7%) | |
| AV prosthesis IE after AVR + ARA | 3 (27.3%) | 4 (%) | |
| AV prosthesis IE after AVR without ARA | 1 (9.1%) | 3 (%) | |
| IE after previous David procedure + ARA | 1 (9.1%) | 1 (6.7%) | |
| Conduit IE after Bentall surgery without ARA | 0 (0.0%) | 1(6.7%) | |
| Conduit IE after Bentall surgery + ARA | 1 (9.1%) | 1(6.7%) | |
| Aorta ascending aneurysm with mixed severe AV | 1 (9.1%) | 2 (13.3%) | |
| Underlying condition | 0.364 | ||
| Infective | 9 (81.8%) | 14 (93.3%) | |
| Noninfective | 2 (18.2%) | 1 (6.7%) | |
| Urgency status | 0.597 | ||
| Urgent | 4 (36.4%) | 4 (26.7%) | |
| Emergency | 7 (63.6%) | 11 (73.3%) | |
| Blood culture | 0.139 | ||
| Positive | 3 (37.3%) | 10 (66.7%) | |
| Negative | 3 (27.3%) | 2 (13.3%) | |
| IE focus | 0.395 | ||
| Unknown | 6 (54.5%) | 10 (66.7%) | |
| Pacemaker IE | 0 (0%) | 1 (6.7%) | |
| Orthopedic implant focus | 0 (0%) | 1 (6.7%) | |
| Thrombophlebitis | 0 (0%) | 1 (6.7%) | |
| Spondylodiscitis | 1 (9.1%) | 0 (0%) | |
| Pathogens | 0.215 | ||
| Not found | 4 (36.4%) | 2 (13.3%) | |
| MSSA | 0 (0%) | 5 (33.3%) | |
|
| 0 (0%) | 1 (6.7%) | |
|
| 0 (0%) | 1 (6.7%) | |
|
| 0 (0%) | 1 (6.7%) | |
|
| 1 (9.1%) | 1 (6.7%) | |
|
| 1 (9.1%) | 1 (6.7%) | |
|
| 0 (0%) | 1 (6.7%) | |
|
| 1 (9.1%) | 0 (0%) | |
| Bicuspid native valve | 1 (9.1%) | 4 (26.7%) | 0.043 |
| Previous AV block | 1 (9.1%) | 2 (13.3%) | 0.738 |
| Drug use history (negative) | 11 (100%) | 15 (100%) | 0.738 |
| Preoperative EF | 0.498 | ||
| Normal | 6 (54.5%) | 9 (60%) | |
| Borderline | 3 (27.3%) | 3 (20%) | |
| Moderately reduced | 0 (0%) | 2 (13.3%) | |
| Severely reduced | 2 (18.2%) | 1 (6.7%) | |
| 30-day survival | 10 (90.9%) | 12 (80%) | 0.446 |
| Parameters | BI (N=11) | FS (N=15) | |
|---|---|---|---|
| Prosthesis size | 24.45 ± 2.70 | 25.66 ± 1.79 | 0.181 |
| Type of surgery | 0.881 | ||
| Current surgery type: primary | |||
| Combined Bentall + AMC | 1 | 3 | |
| Combined Bentall + CABG | 3 | 1 | |
| Combined Bentall + MVR | 0 (0%) | 1 (6.7%) | |
| Combined Bentall + MVRp + | 1 (9.1%) | 1 (6.7%) | |
| Combined Bentall + AAR | 0 | 1 (6.7%) | |
| Current surgery type: redo | |||
| Bentall after previous AVR | 4 (36.4%) | 5 (33.3%) | |
| Redo-Bentall after previous | 1 (9.1%) | 1 (6.7%) | |
| Redo-Bentall after previous | 1 (9.1%) | 1 (6.7%) | |
| Redo-Bentall + CABG+ AMCR | 1 (9.1%) | 1 (6.7%) | |
| Re-redo-Bentall | 0 (0%) | 1 (6.7%) | |
| HLM cannulation site | 0.391 | ||
| Central | 7 (63.6%) | 7 (46.7%) | |
| Peripheral | 4 (36.4%) | 8 (53.3%) | |
| CPB time | 162.82 ± 34.96 | 265.36 ± 90.66 | 0.002 |
| Intraoperative death | 1 (9.1%) | 1 (6.7%) | 0.89 |
| Preoperative LV systolic function | 0.299 | ||
| Normal | 6 (54.5%) | 11 (73.3%) | |
| Moderately reduced | 5 (45.5%) | 3 (20%) | |
| Severely reduced | 0 (0%) | 1 (6.7%) | |
| Parameters | BI | FS | |
|---|---|---|---|
| Mechanical ventilation, hours | 16.18 ± 15.24 | 33.26 ± 28.48 | 0.084 |
| ICU stay, days | 4.27 ± 3.85 | 9.71 ± 14.68 | 0.245 |
| Postoperative in-hospital stay | 33.09 ± 30.63 | 31.33 ± 24.25 | 0.872 |
| Revision surgery during the first postoperative week | 0.209 | ||
| Not needed | 11 (100%) | 10 (66.7%) | |
| Yes, due to coronary artery- | 0 (0%) | 1 (6.7%) | |
| Yes, due to pacemaker-related | 0 (0%) | 1 (6.7%) | |
| Yes, due to bleeding | 0 (0%) | 3 (20%) | |
| 30-day postoperative valve function | 0.337 | ||
| Normal | 9 (71.8%) | 14 (93.3%) | |
| Abnormal | 1 (9.1%) | 0 (0%) | |
| No evaluation of possible | 1 (9.1%) | 1 (6.7%) | |
| Postop LV systolic function | 0.629 | ||
| Normal | 7 (70%) | 11 (73.3%) | |
| Moderately reduced | 3 (30%) | 3 (20%) | |
| Non evaluated due to | 0 (0%) | 1 (6.7%) | |
| In-hospital death | 0.446 | ||
| No | 10 (90.9%) | 12 (80%) | |
| Yes | 1 (9.1%) | 3 (20%) | |
| Cause of in-hospital death | 0.012 | ||
| Cardiac death, intraoperative | 1 (9.1%) | 1 (33.3%) | |
| Non-cardiac death, septic shock | 0 (0%) | 1 (33.3%) | |
| Non-cardiac death, intestinal | 0 (0%) | 1 (33.3%) | |
| Postoperative day of death | - | 5.5 ± 2.12 |
| Complications | BI (n=11) | FS (n=15) | 0.733 |
|---|---|---|---|
| None | 1 (6.67) | 2 (5.00) | |
| Septic shock | 2 (13.33) | 2 (5.00) | |
| Myocardial infarction | 0 (0.00) | 0 (0.00) | |
| Stroke | 0 (0.00) | 0 (0.00) | |
| Atrial fibrillation | 1 (6.67) | 2 (5.00) | |
| AV block III | 4 (26.67) | 1 (2.50) | |
| AV III with PPI | 1 (6.67) | 2 (5.00) | |
| Recurrent IE | 0 (0.00) | 0 (0.00) | |
| Cardiac arrest | 1 (6.67) | 0 (0.00) | |
| Acute heart failure | 0 (0.00) | 2 (5.00) | |
| Pericardial tamponade | 1 (6.67) | 0 (0.00) | |
| Delirium | 0 (0.00) | 3(7.50) | |
| Neutropenic sepsis | 0 (0.00) | 1 (2.50) | |
| Hemothorax | 0 (0.00) | 1 (2.50) | |
| Cardiogenic shock | 0 (0.00) | 1 (2.50) | |
| Cerebral hemorrhage | 0 (0.00) | 2 (5.00) | |
| Pulmonary bleeding | 0 (0.00) | 1 (2.50) | |
| RCA ostial narrowing | 0 (0.00) | 1 (2.50) | |
| Ventricular fibrillation | 0 (0.00) | 2 (5.00) | |
| Acute liver failure | 0 (0.00) | 1 (2.50) | |
| Non-relevant pericardial effusion | 0 (0.00) | 1 (2.50) | |
| Postoperative pacemaker malfunction | 0 (0.00) | 1 (2.50) | |
| Intracranial bleeding of an embolic lesion | 0 (0.00) | 1 (2.50) | |
| LSB | 0 (0.00) | 1 (2.50) | |
| VT | 0 (0.00) | 2 (5.00) | |
| Minimal pericardial effusion | 0 (0.00) | 1 (2.50) | |
| ROSC | 1 (6.67) | 1 (2.50) | |
| Pericardial effusion needing pericardiocentesis | 1 (6.67) | 1 (2.50) | |
| Same-day reoperation | 1 (6.67) | 1 (2.50) | |
| AKI | 1 (6.67) | 1 (2.50) | |
| Intraoperative death due to severely damaged heart basis rupture | 1 (6.67) | 1 (2.50) | |
| Candidemia sepsis | 0 (0.00) | 1 (2.50) | |
| Paravalvular abscess | 0 (0.00) | 1 (2.50) | |
| Abdominal compartment syndrome | 0 (0.00) | 1 (2.50) | |
| Mesenteric ischemia | 0 (0.00) | 1 (2.50) | |
| Total complications | 16 | 40 | 0.733 |
| Parameters | BI | FS | |
|---|---|---|---|
| 30-day LV EF, % | 50.00 ± 8.82 | 55.09 ± 10.70 | 0.253 |
| 30-day TAPSE, mm | 16.10 ± 2.28 | 15.90 ± 3.86 | 0.893 |
| 30-day PPG, mmHg | 25.10 ± 14.63 | 30.54 ± 13.27 | 0.382 |
| 30-day MPG, mmHg | 16.20 ± 7.90 | 15.45 ± 6.82 | 0.819 |
| 6-month LV EF, % | 54.75 ± 3.45 | 53.10 ± 8.29 | 0.607 |
| 6-month TAPSE, mm | 16.86 ± 2.54 | 15.90 ± 3.81 | 0.572 |
| 6-month PPG, mmHg | 30.17 ± 15.95 | 58.60 ± 15.54 | 0.849 |
| 6-month MPG, mmHg | 18.00 ± 9.08 | 14.90 ± 9.08 | 0.519 |
| 12-month LV EF, % | 59.33 ± 4.62 | 50.75 ± 11.69 | 0.260 |
| 12-month TAPSE, mm | 17.00 ± 2.64 | 15.12 ± 4.67 | 0.536 |
| 12-month PPG, mmHg | 36.00 ± 13.11 | 23.37 ± 9.95 | 0.116 |
| 12-month MPG, mmHg | 21.33 ± 7.50 | 14.50 ± 8.55 | 0.257 |
| 24-month LV EF, % | 49.50 ± 13.43 | 47.25 ± 9.57 | 0.820 |
| 24-month TAPSE, mm | 19.00 ± 5.65 | 15.00 ± 3.92 | 0.355 |
| 24-month PPG, mmHg | 34.00 ± 18.38 | 22.50 ± 9.88 | 0.350 |
| 24-month MPG, mmHg | 19.00 ± 8.48 | 12.75 ± 5.31 | 0.313 |
| Survival in months | 52.82 ± 45.26 | 51.56 ± 36.18 | 0.938 |
| Parameters | ARA | NON-ARA | |
|---|---|---|---|
| Prosthesis size | 24.33 ± 2.35 | 26.2 ± 1.68 | 0.021 |
| Redo (year after last surgery) | 4.7 ± 6.18 | 1.83 ± 2.5 | 0.106 |
| Age | 67 ± 15.68 | 55.1 ± 17.00 | 0.043 |
| In-hospital stay, days | 27.2 ± 20.77 | 41 ± 33.63 | 0.108 |
| Intubation, hours | 26.06 ± 24.87 | 27.4 ± 27.18 | 0.450 |
| ICU stay, days | 9.14 ± 14.19 | 5.3 ± 6.65 | 0.218 |
| EuroSCORE II | 18.16 ± 18.22 | 14.48 ± 20.66 | 0.322 |
| STS score | 2.68 ± 3.13 | 3.57 ± 5.96 | 0.316 |
| Height, m | 173.66 ± 8.34 | 175.4 ± 4.94 | 0.281 |
| Weight, kg | 76.86 ± 12.29 | 79.8 ± 8.43 | 0.259 |
| BMI, kg/m2 | 25.52 ± 4.21 | 25.93 ± 3.00 | 0.398 |
| BSA, m2 | 1.89 ± 0.18 | 1.95 ± 0.09 | 0.175 |
| CPB time, minutes | 228.26 ± 98.24 | 212.77 ± 74.52 | 0.344 |
| Cross-clamping time, minutes | 144.2 ± 55.14 | 136.1 ± 41.35 | 0.348 |
| POD of death | 2.2 ± 3.19 | - | 0.282 |
| 30-day LV EF, % | 55.27 ± 7.37 | 52.11 ± 10.05 | 0.214 |
| 30-day TAPSE, mm | 16.72 ± 2.72 | 15.33 ± 3.67 | 0.171 |
| 30-day PPG, mmHg | 30.27 ± 14.19 | 26.66 ± 13.96 | 0.288 |
| 30-day MPG, mmHg | 17.09 ± 7.82 | 15.22 ± 6.30 | 0.285 |
| 6-month LV EF, % | 55.33 ± 6.18 | 52 ± 7.17 | 0.160 |
| 6-month TAPSE, mm | 16.33 ± 3.46 | 16 ± 3.51 | 0.426 |
| 6-month PPG, mmHg | 30.75 ± 10.23 | 28.71 ± 20.88 | 0.405 |
| 6-month MPG, mmHg | 16.87 ± 4.76 | 16 ± 12.84 | 0.430 |
| 12-month LV EF, % | 55.5 ± 5.00 | 51.71 ± 13.22 | 0.301 |
| 12-month TAPSE, mm | 17 ± 3.36 | 14.85 ± 4.63 | 0.221 |
| 12-month PPG, mmHg | 35.5 ± 13.20 | 21.85 ± 8.05 | 0.029 |
| 12-month MPG, mmHg | 21.25 ± 10.87 | 13.57 ± 6.07 | 0.080 |
| 24-month LV EF, % | 55.66 ± 4.93 | 40.33 ± 5.50 | 0.011 |
| 24-month TAPSE, mm | 17 ± 2.00 | 15.66 ± 6.65 | 0.378 |
| 24-month PPG, mmHg | 36 ± 9.84 | 16.66 ± 5.13 | 0.020 |
| 24-month MPG, mmHg | 19.66 ± 5.03 | 10 ± 3.00 | 0.023 |
| Postoperative survival in months | 47.29 ± 43.01 | 58.1 ± 36.62 | 0.261 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Cardiac Valve Diseases and Treatments · Aortic aneurysm repair treatments
INTRODUCTION
**: **
Aortic root (AR) and aortic valve (AV) pathologies encompass a wide spectrum including noninfective and infective diseases, such as AR dilation, dissection, and infective endocarditis (IE) which constitute a surgical challenge, with the indication for AR replacement (ARR)^[1^,^2]^. De Bono and Bentall first described composite valve and graft replacement in 1968^[3]^.
Patient age is one of the strongest deciding factors for the type of prosthesis. The guidelines set forth by the European Society of Cardiology designate 65 years as the threshold for initial consideration when selecting biological AV prostheses^[4^,^5]^. The field of development and evolution of aortic prostheses has seen great progress, with the stentless bioprostheses having superior hemodynamics and beneficial left ventricular remodeling results^[6^,^7]^. However, the results from previous studies regarding AV prostheses should not be generalized for patients needing ARR due to the differences between blood flow and pathophysiological changes adaptation after ARR^[8]^.
Bioprosthetic valves can degenerate structurally, requiring a full redo ARR. Older patients are requiring more redo cardiac operations, leading to an increase in AR reoperations^[9]^. As transcatheter aortic valve implantation (TAVI) rates continue to rise in the modern era of transcatheter cardiac surgery, it is expected that a greater number of young patients will receive xenografts. The utilization of Bioroots is highly rewarded in cases requiring redo surgeries, as it facilitates the application of transcatheter alternatives over an extended period^[10^-^12]^. Moreover, given the benefits of avoidance of anticoagulation and the alternative of valve-in-valve TAVI instead of a high-risk reoperation, the use of Bioroots technology is becoming more prevalent as a popular solution for patients in need of ARR^[8]^. And although first generation xenografts had a limited durability^[8]^, new generation bioconduits have proven to be equivalent to both their mechanical and stented conduits analogs, in terms of long-term outcome, reoperation rates, functional performance, and longevity^[13]^.
However, the commercially available bioconduits that can be utilized for the Bentall procedure are still limited^[14^,^15]^. One of the most extensively studied and frequently utilized commercially available bioconduits is the Freestyle™ (FS) conduit by Medtronic (Irvine, California, United States of America), offering a xenogeneic whole ARR biological conduit^[12^,^16]^. An alternative is by surgeons' choice, the application of self-manufactured conduits that were created by suturing biological aortic prostheses onto a Dacron® graft^[17]^. Another commonly utilized complete biologic substitute was the BioIntegral (BI) prosthesis developed by BioIntegral Surgical, Inc. (Mississauga, Ontario, Canada). The BI is an enhanced iteration of the Shelhigh® bioconduit developed by Shelhigh®, Inc. (Milburn, New Jersey, United States of America). It is composed of a compound xenograft made up of a porcine AV and bovine pericardium, which has been treated with No-React® preservation technology, providing reduced rates of reinfection and improved biocompatibility^[18]^.
AR IE carries an ominous prognosis and recurrence rates^[19]^. Moreover, reoperative ARR conducted in a number of complex clinical scenarios is related to high morbidity and mortality^[20]^. There is still limited evidence regarding the clinical results. More data is needed comparing the results after the application of different bioconduits in challenging urgent or emergency cases of ARR. Here, we report our experience and the clinical results of patients undergoing urgent or emergent complete ARR surgery with BI and FS bioconduits.
METHODS
Data and Patient Cohort
We conducted a retrospective collection of patient data, including demographic details, clinical outcomes, perioperative protocols, postoperative recovery, imaging findings, and laboratory results from our institutional databank. The research was granted approval by the Ethics Committee of RWTH University Hospital Aachen, in compliance with the IRBP regulations 10/2014 and EK151/09-Version-1.3 guidelines. Due to the retrospective design of our study, the requirement for informed consent was waived by our institutional review board. In this single-center, retrospective, observational study, adult participants (aged over 18 years) who underwent an isolated or combined full ARR with a bioconduit of either FS or BI type, in our Department of Cardiothoracic Surgery, University Hospital of Aachen RWTH, from January 2015 until September 2020, were analyzed and followed up until December 2023.
We obtained subsequent data by conducting direct telephone interviews with either the referring cardiologists and general physicians or the patients. All patients who survived underwent transthoracic assessment using two-dimensional echocardiography in accordance with the institutional protocol post-discharge, at six months post-surgery, and subsequently on an annual basis.
Statistical Analysis
All quantitative variables were presented by mean values and standard deviations, and all qualitative variables were presented as frequencies and percentages (N, %). Comparisons between continuous variables of two groups were conducted using the Student’s t-test analysis for the comparison of categorical variables; Chi-square (X^^2^^) test was used. Kaplan-Meier survival analysis was conducted for different cohorts throughout the duration of the follow-up period. P values < 0.05 were considered as statistically significant. IBM Corp Released 2023, IBM SPSS Statistics for Windows, version 29.0, Armonk, NY: IBM Corp. was used for all the analyses.
Surgical Technique
The same experienced team of cardiac surgeons performed all procedures. The team decided on the surgery technique after daily meeting evaluation. The selection of the bioconduit was contingent upon the surgeon's individual preference. Standard surgical strategies with median sternotomy approach and application of cardiopulmonary bypass (CPB) were used. The selection of the cannulation technique for CPB was dictated by the patient's medical condition and the complexity of the surgical procedure, with consideration given to direct aortic, subclavian, or femoral cannulation. When needed, in redo cases, the CPB was applied before resternotomy through peripheral cannulation. Depending on the extent of the anticipated aortic reconstruction required, the optimal cannulation and cerebral protection strategy were implemented in each case. Mild (28-32 °C) or moderate (25-28 °C) hypothermia were implemented. During hemiarch or total arch replacement procedures, hypothermic circulatory arrest with antegrade cerebral perfusion was employed. Myocardial preservation and cardiac arrest were achieved with the use of antegrade and optional retrograde crystalloid cardioplegia (Custodiol®, Dr. F. Köhler Chemie, Bensheim, Germany). The aorta was incised 4 cm above the right coronary ostium, and the AR was extensively freed from the surrounding tissue, down to the subvalvular plane. The prosthetic or native AV was completely excised, and both coronary ostia were prepared, suspended, and mobilized as buttons. The excision of the aortic sinuses was followed by the selection of an appropriate biological pericardial conduit. The BI conduit was implanted with single, interrupted 3-0 Ethibond® (Ethicon, Johnson & Johnson Medical, Brussels, Belgium) pledged U-stitch sutures. Everted sutures with pledgets located outside of the conduit were used. For the FS application, running 3-0 PROLENE® (Ethicon) was applied. On the former left ostium of the FS graft, the left coronary artery button was implanted. In cases of BI, the holes for coronary buttons were cut open on the respective sinuses of the conduit. Great care was taken to prevent any tension or kinks on the right button. A 4 mm punch was used for the opening pericardial conduit, matching the left coronary button. After trimming the coronary button, a 2-3 mm aortic cuff was ensured, followed by a parachute anastomosis with a 5-0 (or 6-0) polypropylene running technique.
In the case of AR abscess (ARA), the proximal suture line utilized for the implantation of the bioconduit must run continuously in the left ventricular outflow tract along the robust nadir of the abscess. The bites taken during this procedure encompass both the complete muscular septum and a small margin of AML. In some cases, a pericardial plastic patch of the aortomitral curtain (AMC) was applied. The right coronary artery was re-attached, and the bioconduit was shortened to match the aorta, then sutured with 4-0 polypropylene. Once all distal anastomoses were finished, the patient was gradually rewarmed.
Valve size was determined through imaging and confirmed during surgery. Priority is given to maximizing orifice area and optimizing the hemodynamics in aneurysmal root disease cases.
RESULTS
Twenty-six patients are reported in this study; 23 (88.46%) patients had an infective underlying cause; 21 (80.8%) were males, and five (19.2%) were females. Demographic and clinical data are detailed and presented in Table 1. The average age was 62.31 ± 16.61 years in the total cohort, 58.13 ± 15.82 in the FS group, and 68.00 ± 16.66 in the BI group; 30.76% were urgent and 69.23% were emergency cases.
Before surgery, one (3.8%) patient suffered severe complications - critical limb ischemia and intestinal ischemia by septic cardioembolic closure of the common iliac artery and right common femoral artery.
Of the sample group (N=26), 26.9% underwent primary stand-alone Bentall surgery, while others had previously undergone an aortic surgery or a Bentall procedure after a previous AV replacement. Some patients also underwent other procedures such as mechanical Bentall, supracoronary ascending aorta replacement (SCAAR), David procedure with hemiarch replacement, and SCAAR for type-A aortic dissection. Four patients had AMC with pericardial plastic patch during their primary operation, and some required coronary artery bypass grafting or mitral valve repair. Among those who had redo surgeries within the sample group, five took place less than one year from their last cardiac procedure. The detailed data of the previous procedures is summarized in Table 1. Operative variables are summarized in Table 2. Ten patients received primary surgery. The mean period between the previous and the last cardiac surgery was 3.12 ± 4.87 years, after the previous surgery, while 4.33 ± 6.92 years for the BI and 2.13 ± 2.07 years for the FS prosthesis. Fifteen patients had a native AV, eight had an AV bioprosthesis, one had a mechanical prosthesis, and two had a mechanical conduit. Twelve (46.10%) patients were placed on CPB through peripheral cannulation before resternotomy. ARA was present in 15 (57.7%) patients. In five (19.23%) patients, an additional pericardial plastic patch of the AMC was applied due to extensive abscessed damage of the AR. Postoperative complications are summarized in Table 3. Most of the patients presented a combination of serious postoperative complications. The median ICU stay was four days, and the median duration of hospital stay was 29 days. The mortality rate during hospitalization was identical to the 30-day mortality rate, which stood at four out of 26 cases (15.40%). Two (7.70%) patients died intraoperatively due to irreversible AR damage. The most dominant postoperative complication was AV III block (N=9, 34.62%), while in four (15.4%) patients permanent pacemaker implantation was needed. The second most common was septic shock (N=4, 15.4%). Seven (26.93%) patients required new dialysis, and two patients (7.7%) suffered from transient neurologic dysfunction.
Survival and Follow-up Results
All patients underwent surgery with ARR and bioconduit application. Of those, two died in the operation theater (7.7%) due to severe AR damage. Another two patients did not survive admission, so the total in-hospital mortality was four (15.38%). Thirty-day survival was 84.61% for all patients, 38.46% for BI, and 46.15% for FS. A comprehensive analysis of postoperative complications is presented in Table 4.
Follow-up was closed on December 31, 2023, and by then, ten (38.46%) patients were dead. Overall follow-up was 100% complete at a mean follow-up period of 4.33 ± 3.28 years (maximum follow-up was 128 months [10.67 years], and median follow-up was 4.25 years) postoperatively. Comprehensive details regarding the follow-up can be found in Table 5.
Most common cause of death was non-cardiac. One (3.8%) patient was reoperated 10 months after admission in another hospital due to leakage and died one month later of cardiac cause.
Initial echocardiographic evaluation demonstrated favorable functional outcomes. Freedom from reoperation in follow-up was 80.76%. Four-year survival rate was 57.7% (N=15). Six BI patients survived > 4 years, and nine FS patients survived > 4 years.
Correlations
There was statistically significant dependence between previous aortic surgery and previous aortic dissection with SCAAR to the 30-day survival (chi-square [4.26] 12.254, P-value 0.016 and chi-square [1.26] 5.720, P-value 0.017, respectively). Eleven patients died in the follow-up of 17.04 ± 22.47 months, ten (90.9%) of them had received an ARR as redo surgery, showing a statistically significant dependence between previous cardiac surgery and follow-up death (chi-square [1.26] 6.949, P-value 0.008). There was no significant statistical difference between the survival time of the two prosthesis types, P-value was > 0.05 (0.889). We didn’t prove any significant difference (P-value > 0.005) regarding the survival between the infective and noninfective groups, as seen in Figure 1.
Fig. 1. Survival per pathology type.
Comparison Between the Groups
BioIntegral vs. Freestyle™ Bioconduit
A comparison of different variables between the two conduits is to be seen in Tables 1-5. CPB time is shorter in BI vs. FS (162.82 ± 34.96 vs. 265.36 ± 90.66, P-value 0.002). As seen in Figures 1 and 2, there was no significant statistical survival difference (P-value 0.650). Mean survival for BI was 81 ± 37.81 months, and for FS it was 75.66 ± 19.65 months. There was no significant statistical difference regarding preoperative comorbidities or postoperative complications in both groups.
Fig. 2. Survival per bioconduit type.
Aortic Root Abscess vs. Non-Aortic Root Abscess
Data are shown in Table 6. Patients with ARA presented at an older age than patients without ARA (67 ± 15.68 vs. 55.1 ± 17, P < 0.043) and received bigger prosthesis sizes (26.2 ± 1.68 vs. 24.33 ± 2.35, P=0.021). Echocardiographic, 12-month peak pressure gradient in the ARA group was higher than for non-ARA patients (35.5 ± 13.20 vs. 21.85 ± 8.05, P-value=0.029).
Table 6: Comparison of operative and follow-up variables in infective endocarditis cases with and without ARA.
DISCUSSION
Surgical interventions on the AR have exhibited substantial advancements in recent years, thanks to the progress of surgical techniques and operative and postoperative approaches. However, due to the multiple severe diseases of the aortic bulb and the multi-morbid patients requiring ARR, ARR remains a challenge despite the rapid development in this field. In this study, we report our experience and results after urgent and emergent ARR with BI and FS bioconduits.
Esaki et al.^[20]^ have identified the risk factors associated with operative mortality related to ARR as including previous myocardial infarction, chronic obstructive pulmonary disease (COPD), and concurrent mitral valve surgery (MVS), while the long-term mortality increased with age and concomitant MVS. In our study, we confirmed these risk factors as well. Reoperative ARR is of significant potential high morbidity and mortality^[20]^. Interestingly, we showed a higher incidence of morbidity and mortality in reoperative cases, especially after previous surgery for aortic dissection. Additionally, in our study, one of the most dominant postoperative complications was the increased postoperative permanent pacemaker implantation rate, which as described in the literature in an independent long-term mortality risk factor^[21]^. Patel P.M. et al.^[1]^ reported an acceptable mid-term outcome of ARR with the FS conduit. In our study, despite the small number of patients, we could confirm this finding too.
Over time, the ARR with application of xenografts is gaining ground over the traditional ARR with mechanical conduits and is a proven exceptional solution in cases with different AR pathologies, including IE complicated with ARA and a destructed root. Bioroots offer comparable benefits to aortic allografts, as they enable the reconstruction of the AR following extensive debridement of infected tissues. Multiple reports indicate that bioroots exhibit remarkable durability, achieving a 94% rate of freedom from structural valve disease over a span of 14 years^[1^,^22^-^24]^. In our study, we observed favorable results in terms of clinical outcomes, with no notable occurrences of structural valve dysfunction or other significant conduit-related complications noted during the follow-up period. Interestingly, in our study, although the BI group had a higher operative risk of mortality, according to the Society of Thoracic Surgeons and the European System for Cardiac Operative Risk Evaluation II scores, we did not prove any significant statistical difference between the survival in the two bioconduit subgroups (P-value 0.889).
Based on the bibliography, operative mortality of ARR is reported with a range of 1% to 5% when performed in the setting of primary cardiac surgery^[25^-^28]^, and 2% to 18% in the case of reoperative AR surgery^[9^,^29]^. Esaki et al.^[20]^ showed a five-year survival after reoperative ARR of 74.0%, while previous ARR, prior to proximal aortic surgery, and concomitant arch replacement proved to be no risk factors for operative mortality. LeMaire et al.^[24]^ showed in a report of 132 patients with ARR using stentless xenografts, a survival of 85.6% ± 3.1% at one year and 77.8% ± 4.8% at five years. This approximates our findings, as we showed that the four-year survival was 57.7%. Comparing the two bioconduits, we proved significantly longer CPB times in the FS group, but no notable differences by terms of clinical outcome, survival, and graft functional performance as shown in Table 5. This is consistent with other studies showing no significant differences, but shorter CPB due to the simplified implantation technique of BI conduit^[22]^. Puehler et al.^[30]^ reported a 33-patient cohort who underwent Bentall procedure with BI conduit and showed 30-day mortality of 33%, mainly due to multiorgan failure, 3% graft reinfection with ARA, but a stable survival of patients after hospital discharge. We could not prove a significant difference in the survival correlated to the presence of ARA in the infective cases. This may be due to the small cohort volume.
Limitations
The study has certain limitations due to its retrospective and non-randomized nature. Additionally, the selection of graft-conduit was based on the surgeon’s preference, experience, and surgery type. When comparing the two groups, significant disparities were observed in their risk profile and baseline characteristics since they were not entirely homogeneous. This study encompassed diverse clinical settings and patients who had previously undergone cardiac or aortic surgeries. This study includes urgent and emergency cases and should not be generalized in elective ARR cases.
CONCLUSION
ARR presents a formidable surgical challenge due to the severity of its pathology. The choice between utilizing the BI or FS conduit does not appear to significantly impact ultimate outcomes in terms of operative mortality, survival, and follow-up valvular hemodynamics. Nonetheless, it is noteworthy that age, comorbidities, and concomitant surgery remain crucial factors that directly influence long-term survival and clinical outcomes. It should be emphasized that this study was conducted at a single center and thus its findings cannot be generalized or applied universally. The individualized assessment of patients requiring an ARR remains essential for achieving the best outcomes. Consequently, additional research with larger cohorts is warranted to attain a more comprehensive understanding of this complex entity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patel PM Callahan M Dong A Wei J Binongo J Leshnower B Clinical outcomes using freestyle valve-valsalva graft composite conduit for aortic root replacement Ann Thorac Surg 2022114364364910.1016/j.athoracsur.2021.12.022.35031292 · doi ↗ · pubmed ↗
- 2Kouchoukos NT Marshall WG Jr, Wedige-Stecher TA. Eleven-year experience with composite graft replacement of the ascending aorta and aortic valve J Thorac Cardiovasc Surg 19869246917053531730 · pubmed ↗
- 3Bentall H De Bono A. A technique for complete replacement of the ascending aorta Thorax 196823433833910.1136/thx.23.4.338.5664694 PMC 471799 · doi ↗ · pubmed ↗
- 4Baumgartner H Falk V Bax JJ De Bonis M Hamm C Holm PJ 2017 ESC/EACTS guidelines for the management of valvular heart disease Eur Heart J 201738362739279110.1093/eurheartj/ehx 391.28886619 · doi ↗ · pubmed ↗
- 5Blehm A Schurr P Sorokin VA Zianikal I Kamiya H Albert A Comparison of different surgical techniques in 112 consecutive patients with aortic root operations: when should the valve be spared?J Heart Valve Dis 201423191624779323 · pubmed ↗
- 6Lim E Ali A Theodorou P Sousa I Ashrafian H Chamageorgakis T Longitudinal study of the profile and predictors of left ventricular mass regression after stentless aortic valve replacement Ann Thorac Surg 20088562026202910.1016/j.athoracsur.2008.02.023.18498814 · doi ↗ · pubmed ↗
- 7Lehr EJ Wang PZ Oreopoulos A Kanji H Norris C Macarthur R. Midterm outcomes and quality of life of aortic root replacement: mechanical vs biological conduits Can J Cardiol 2011272262.e 152010.1016/j.cjca.2010.12.034.21459276 · doi ↗ · pubmed ↗
- 8Etz CD Homann TM Rane N Bodian CA Di Luozzo G Plestis KA Aortic root reconstruction with a bioprosthetic valved conduit: a consecutive series of 275 procedures J Thorac Cardiovasc Surg 200713361455146310.1016/j.jtcvs.2007.01.058.17532939 · doi ↗ · pubmed ↗