Management of a unique hourglass-shaped abdominal aortic aneurysms: A case report
Javad Salimi, Pejman Pourazari, Afrooz Sadeghi, Amir Shokri

TL;DR
This case report describes the successful open surgery for a rare hourglass-shaped abdominal aortic aneurysm in a high-risk patient.
Contribution
The paper presents a unique case of hourglass-shaped AAA managed through open surgery due to unsuitability for endovascular repair.
Findings
Endovascular repair was not feasible due to inadequate proximal landing zones.
Open surgical intervention was necessary to safely repair the aneurysm.
Preoperative imaging was critical in guiding the treatment decision.
Abstract
Hourglass-shaped abdominal aortic aneurysms (AAAs) represent a complex variant of aneurysms, characterized by a distinctive constriction within the aorta, which are characteristically located in the abdominal or thoracic regions. Their unique morphology poses significant diagnostic and therapeutic challenges, particularly when considering the feasibility of endovascular repair versus open surgical intervention, demanding a specific approach to management. We present the case of a 68-year-old female patient admitted with abdominal pain complaints. Despite stable vital signs, her medical history, including diabetes mellitus and reduced ejection fraction (EF) of 40 %, indicated a heightened cardiovascular risk. Subsequent imaging studies, including Doppler ultrasonography and CT angiography, showed the presence of two adjacent abdominal aortic aneurysms forming an hourglass-shaped…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
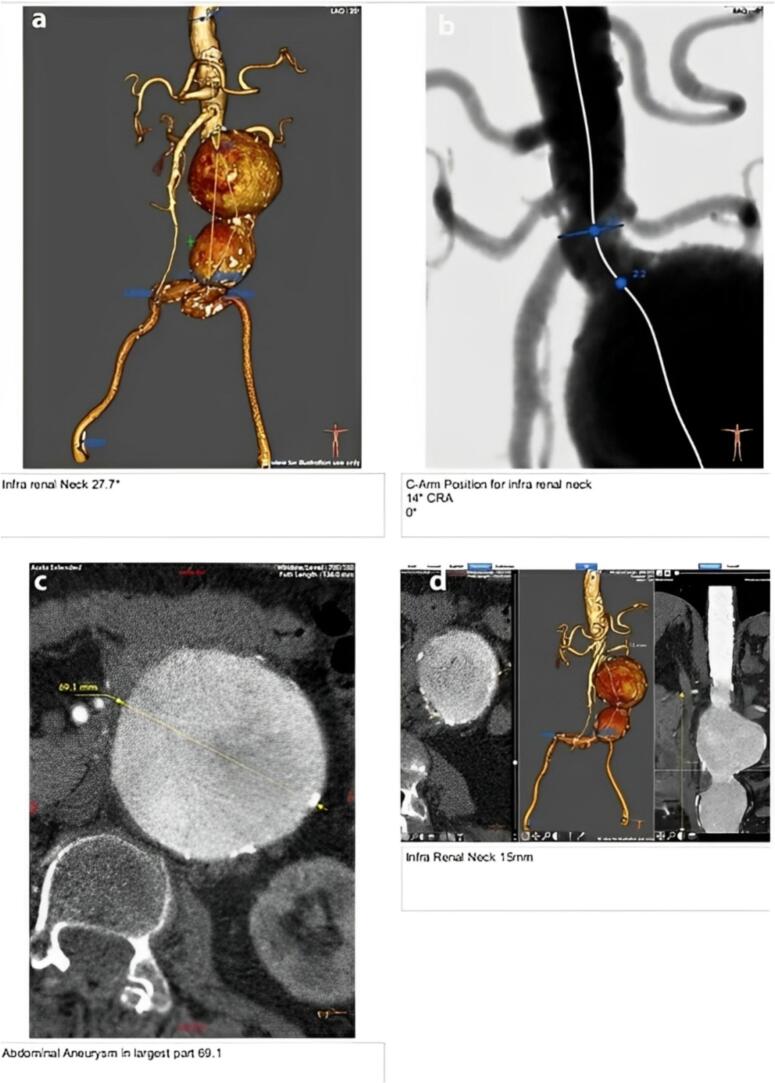 Figure 1
Figure 1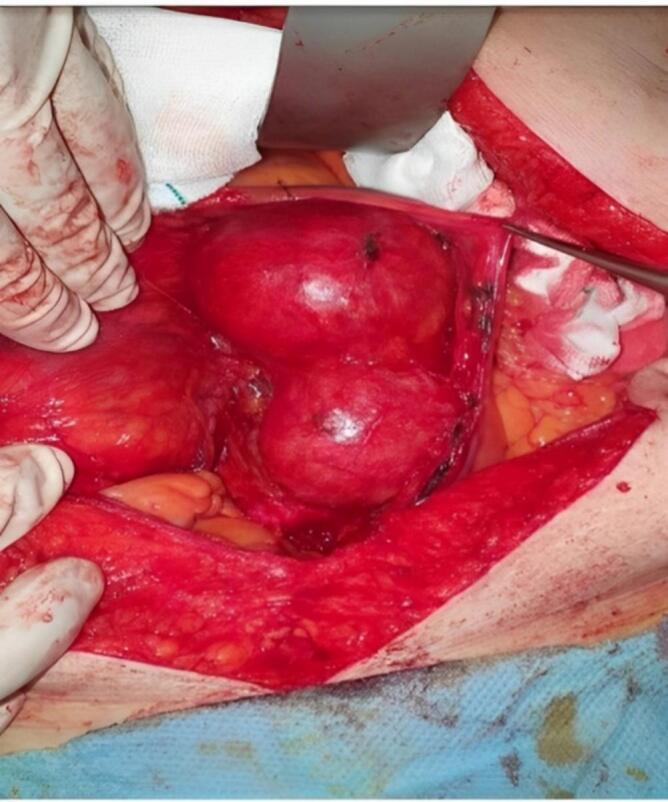 Figure 2
Figure 2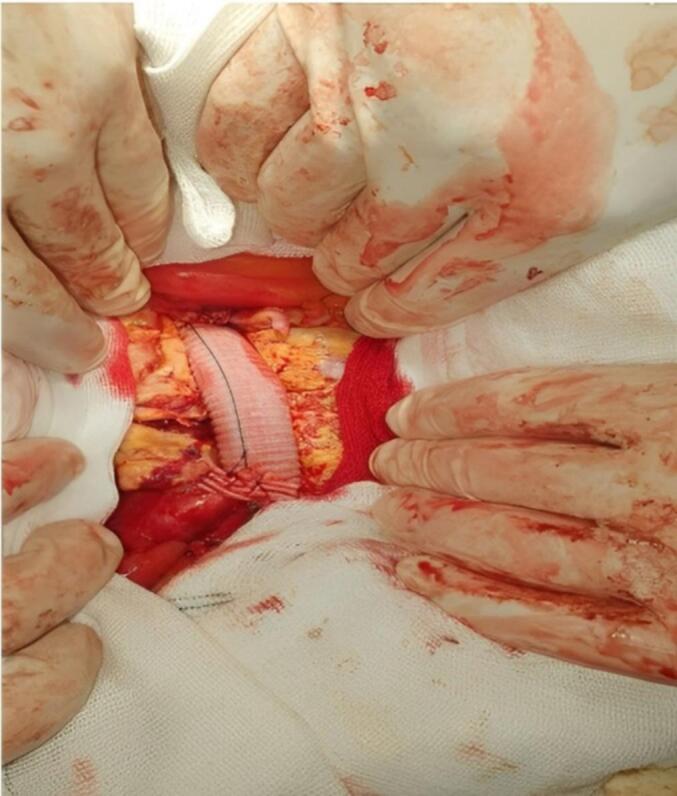 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic aneurysm repair treatments · Aortic Disease and Treatment Approaches · Cardiac, Anesthesia and Surgical Outcomes
List of abbreviations
AAAAbdominal Aortic AneurysmCTComputed TomographyCTAComputed Tomography AngiographyEFEjection FractionEVAREndovascular Aneurysm Repair
Background
1
Hourglass-shaped abdominal aortic aneurysms (AAAs) constitute a rare and interesting variant of aortic pathology, which accounts for around 1.3 % of all deaths among men aged 65 to 85 years in developed countries, characterized by a distinct narrowing of the aorta that complicates traditional management approaches. An aortic aneurysm is essentially an abnormal aorta dilation resembling a hernia, which may occur in either the abdominal or thoracic regions (1,2). An aneurysm occurs when the aorta's diameter is more than 1.5 times its normal size (3). These vascular anomalies pose significant risks, including rupture and thrombosis, which can lead to life-threatening situations. Effectively managing AAAs involves thorough evaluation and customized intervention strategies that determine the specific shape of the aneurysm and the patient's overall health. Most individuals with aortic aneurysms remain asymptomatic until a rupture occurs, at which point they may experience severe abdominal and lower back pain, with some severe drop in their blood pressure (4,5).
Early diagnosis and intervention are crucial, as the weakened aorta wall can rupture, leading to catastrophic hemorrhage from this major artery (6). The mortality rate associated with abdominal aortic dissection is reported to be as high as 81 %, with 32 % of patients dying before reaching medical facilities (7).
While abdominal aortic aneurysms are more common than their thoracic counterparts, diagnosing them may appear challenging (1). Although abdominal ultrasound is often used as an initial screening tool, CT angiography remains the gold standard for confirming the diagnosis and plays a crucial role in the detailed evaluation of aneurysm morphology guiding the treatment strategy. These imaging modalities are essential in determining whether a patient should undergo open surgery or an endovascular aneurysm repair (8,9).
In this case report, we present an instance of two adjacent abdominal aortic aneurysms manifested in an hourglass shape. This unique presentation not only posed diagnostic challenges but also required careful consideration in our treatment decisions. The current report gave details of the management of this rare position, which emphasized the diagnosis, treatment strategies, and the complications involved in the results obtained by us. By sharing our findings, we aim to enrich the existing literature on abdominal aortic aneurysms and refine relevant management protocols for this complex condition, ultimately enhancing patient care and outcomes.
Case presentation
2
A 68-year-old woman was admitted to the emergency department with complaints of persistent abdominal pain over several days. Her vital signs were stable upon her arrival, indicating no immediate hemodynamic instability. A fully physical examination ordered the doctor to Doppler ultrasonography, due to which AAA was diagnosed. To collect more detailed information about the form, size, and location of the aneurysm, a CT angiogram was also done (Fig. 1). This case was reported in line with the SCARE criteria (10).Fig. 1. Various Viewpoints of the Aneurysm, including (a) a 3D CT angiographic reconstruction showing an infrarenal abdominal aortic aneurysm with a neck length of 27.7 mm; (b) a fluoroscopic image with optimal C-arm positioning (14° cranial angulation, 0° rotation) for assessment oh = f the infrarenal neck during endovascular planning; (c) an axial CT image demonstrating the maximal transverse diameter of the aneurysmal sac; and (d) #d post-processing and coronal CT images showing an infrarenal neck length of 15 mm, providing crucial information for EVAR feasibility and endograft selection.Fig. 1
The patient's medical history included diabetic mellitus, hypertension, and a history of cigarette smoking, introducing several risk factors that complicated her clinical management. Given her underlying diabetes and a low ejection fraction of 40 %, the medical team was initially chosen for an endovascular approach to the management of aneurysms, often preferred for high-risk patients due to its minimally aggressive nature and rapid recovery time. However, on further evaluation, it became clear that the proximal landing zone for endovascular repair was insufficient, which inspired us to reevaluate the treatment plan. Eventually, it was decided to proceed with open surgical intervention (Fig. 2, Fig. 3).Fig. 2. Intraoperative view of an hourglass-shaped abdominal aortic aneurysm with two distinct aneurysmal sacs connected by a narrowed segment.Fig. 2. Fig. 3Post-resection view showing successful graft placement following excision of the abdominal aortic aneurysm.Fig. 3
The procedure was performed under general anesthesia with laparotomy. Approximately three minutes after the administration of heparin (5000 units IV), distal control was first obtained, followed by proximal control, with total clamp time estimated to be 12–14 min. The aneurysmal segment, including both aneurysms, was excised. A straight Dacron tube graft (approximately 20 mm in diameter) was anastomosed end-to-end using Prolene 3–0 continuous sutures. Hemostasis was confirmed, and pulses were palpable distally. The intraoperative blood loss was minimal (estimated 50–130 mL).
The patient had an uneventful recovery. She was extubated in the operating room, monitored in the ICU for one day, and then transferred to the general ward. She was discharged on postoperative day 4 in stable condition with palpable distal pulses and no signs of ischemia.
Follow-up imaging with Doppler ultrasonography was performed one month post-operation, revealing a patent graft with no residual flow into the excluded aneurysmal sacs. The aneurysms had been completely bypassed, and there were no signs of complications such as thrombosis or pseudoaneurysm formation. The patient remained asymptomatic, and clinical examination confirmed bilaterally normal peripheral pulses.
Discussion
3
The management of AAAs involves a choice between open surgery and endovascular approaches, each with its own indications and risks. While the majority of aortic aneurysms present as singular, well-defined dilations, rare cases of dual aneurysms forming an hourglass-shaped configuration have been reported, predominantly in the thoracic aorta (11,12). This case report presents an unusual instance of an hourglass-shaped aortic aneurysm located in the abdominal section of the aorta. Remarkably, this case involves two adjacent abdominal aortic aneurysms that were nearly connected, a presentation scarcely encountered in clinical evidence.
The differential diagnoses considered included a variety of conditions with similar clinical presentations. The patient first presented with chronic abdominal pain, which can be suggestive of a variety of conditions like acute mesenteric ischemia, perforated viscus, and renal colic. The initial ultrasound, followed by CT angiography, helped narrow down the diagnosis to an abdominal aortic aneurysm. While mesenteric ischemia and renal stones were considered due to the patient's risk factors, the imaging findings provided critical evidence in favor of an aneurysm diagnosis. The CT angiogram confirmed the presence of the aneurysm and highlighted its atypical hourglass shape, distinguishing it from other possible causes of abdominal pain.
Double abdominal aortic aneurysms raise important considerations for each condition, its treatment, and surgical approach. Morphologically different hourglass AAAs pose difficulties in decision-making due to the anatomic configuration affecting whether endovascular repair is possible. Although endovascular aneurysm repair is often preferred for high-risk patients due to its minimally invasive nature and shorter recovery times (13), in this present case, the insufficient proximal landing zone rendered EVAR unsuitable, necessitating open surgical intervention. This highlights a critical limitation of endovascular approaches in cases with complex vascular anatomy.
The result of this case effectively illustrates several key points. First, adequate preoperative imaging is paramount to aneurysm morphology description and treatment planning. CT angiography remains the gold standard in assessing aneurysm dimensions, thrombus formation, and the feasibility of stent graft placement. Doppler ultrasonography was initially used for detection, followed by a CT angiogram to assess the full extent and suitability for surgical intervention. Importantly, approximately three minutes after the administration of heparin, distal control was first obtained, followed by proximal control. These critical steps were essential for ensuring hemodynamic stability and maintaining surgical precision. Second, patient-specific factors, such as cardiovascular comorbidities and anatomical constraints, should guide the selection of intervention type. In this instance, despite the patient's comorbid conditions, open repair was deemed the safest and most durable option.
Finally, this case highlights the value of individualized surgical planning in the context of aneurysmal disease complexity. While EVAR has revolutionized the treatment of routine AAAs, open repair is still the mainstay for patients with complex anatomical presentations. The patient's good postoperative result supports the fact that despite its invasiveness, open surgery remains a viable and often necessary approach in select cases.
Conclusions
4
In conclusion, hourglass-shaped AAAs represent a rare but clinically significant entity requiring careful diagnostic and therapeutic consideration. The present case contributes to the limited existing literature and reinforces the necessity of personalized management strategies to optimize outcomes in complex aortic aneurysms. Future studies should focus on refining classification criteria for such aneurysms and developing advanced endovascular techniques to expand treatment options for patients with challenging vascular anatomy.
Informed consent
Written informed consent was obtained from the patient guardian for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Consent
Informed written consent was obtained from the patient for publication of this Case report along with any accompanying images. On request, a copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethical approval
Ethical approval for this study (IR.TUMS.SINAHOSPITAL.REC.1403.160) was provided by the Ethics Committee of Tehran University of Medical Sciences, Tehran, IRAN.
Ethics approval
The study was carried out by the Declaration of Helsinki and was registered by the ethics committee of the Department of Cardiology.
Funding
No funding.
Author contribution
JS, PP, and AS were responsible for the surgical management of the patient and data acquisition. AS and AF contributed to drafting the manuscript. JS and PP critically reviewed and revised the manuscript for intellectual content. All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Guarantor
Amir Shokri
Research Registration Number
Not applicable.
Conflict of interest statement
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mathur A.Mohan V.Ameta D.Gaurav B.Haranahalli P.Aortic aneurysm Journal of translational internal medicine.41201635412819151610.1515/jtim-2016-0008 PMC 5290913 · doi ↗ · pubmed ↗
- 2Dansey K.D.Varkevisser R.R.B.Swerdlow N.J.Li C.de Guerre L.E.V.M.Liang P.Epidemiology of endovascular and open repair for abdominal aortic aneurysms in the United States from 2004 to 2015 and implications for screening J. Vasc. Surg.74220214144243359229310.1016/j.jvs.2021.01.044PMC 8316377 · doi ↗ · pubmed ↗
- 3Vaitėnas G.Mosenko V.RačytėA.Medelis K.Skrebūnas A.Baltrūnas T.Abdominal aortic aneurysm diameter versus volume: a systematic review Biomedicines 11320239413697992010.3390/biomedicines 11030941 PMC 10046268 · doi ↗ · pubmed ↗
- 4Upchurch G.R.Jr.Schaub T.A.Abdominal aortic aneurysm Am. Fam. Physician 73720061198120416623206 · pubmed ↗
- 5Garrity B.M.Sugarman E.Pulley S.Abdominal aortic aneurysm rupture presenting with focal weakness and altered mental status: a case report Int. J. Emerg. Med.1512022283573309010.1186/s 12245-022-00433-5PMC 9214986 · doi ↗ · pubmed ↗
- 6Nienaber C.A.Clough R.E.Sakalihasan N.Suzuki T.Gibbs R.Mussa F.Aortic dissection Nat. Rev. Dis. Primers 21201611810.1038/nrdp.2016.7127560366 · doi ↗ · pubmed ↗
- 7Reimerink J.J.van der Laan M.J.Koelemay M.J.Balm R.Legemate D.A.Systematic review and meta-analysis of population-based mortality from ruptured abdominal aortic aneurysm Br. J. Surg.100112013140514132403755810.1002/bjs.9235 · doi ↗ · pubmed ↗
- 8Vu K.N.Kaitoukov Y.Morin-Roy F.Kauffmann C.Giroux M.F.Thérasse E.Rupture signs on computed tomography, treatment, and outcome of abdominal aortic aneurysms Insights Imaging 5320142812932478906810.1007/s 13244-014-0327-3PMC 4035490 · doi ↗ · pubmed ↗