Pre-exercise health screening in the UAE: A necessity or barrier to engage in physical activity?
Rifah Anwar Assadi, Afreen Abdul Rahim Sanaullah, Sathyapriya Nandagopal, Shahnaz Mohamed Wazil, Priya Pardasani, Meenadarsini Dhamothiran, And Ozyigit, Jagat Gopinath, Ans Ahmed Mahmood, Maryam Almarzooqi, Bibi Morsal Sayedy, Elham Riyaz, Jayakumary Muttappallymyalil

TL;DR
This study examines how often people in the UAE use pre-exercise health screenings and finds that only a small percentage do so, with factors like age and health conditions influencing the practice.
Contribution
The study identifies sociodemographic and health-related factors influencing pre-exercise screening adoption in the UAE.
Findings
Only 29.5% of participants underwent pre-exercise screening.
Older age, being male, higher education, and employment were associated with higher screening rates.
Most participants did not receive guidance from exercise professionals despite supporting mandatory screening.
Abstract
Sedentary lifestyles contribute to the rise of non-communicable diseases, making physical activity (PA) crucial for public health. Pre-exercise screening is an important tool for ensuring safety, but its utilization and the factors influencing its adoption need further exploration. This study assesses the utilization of pre-exercise screening among physical activity facility users in the UAE, identifying sociodemographic and health-related factors associated with screening practices. A cross-sectional study was conducted among adults aged 18 and above in the UAE. Data were collected through a self-administered questionnaire from 630 adults using PA facilities, covering socio-demographic characteristics, PA engagement, knowledge of PA benefits, and pre-exercise screening practices. Data analysis was performed using SPSS version 28 for descriptive and inferential statistics. Of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
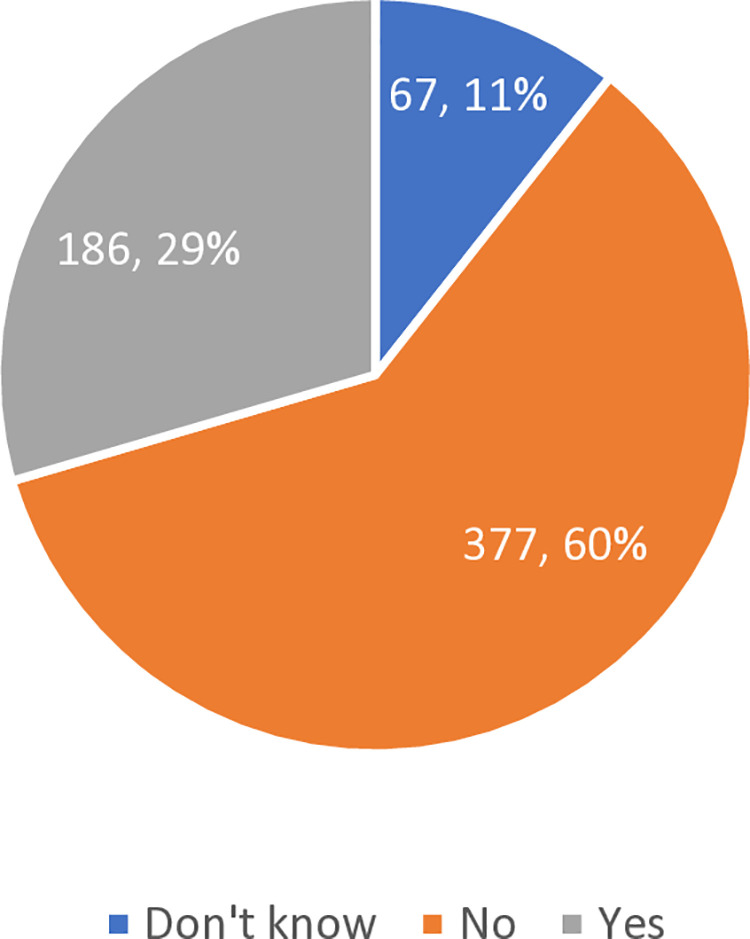 Fig 1
Fig 1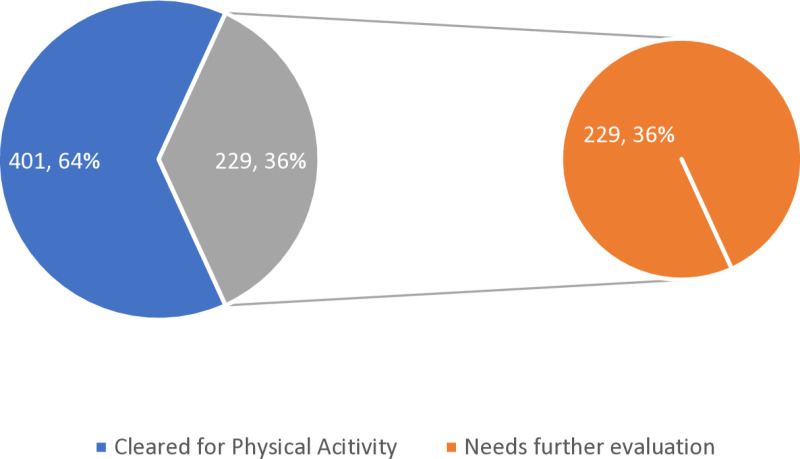 Fig 2
Fig 2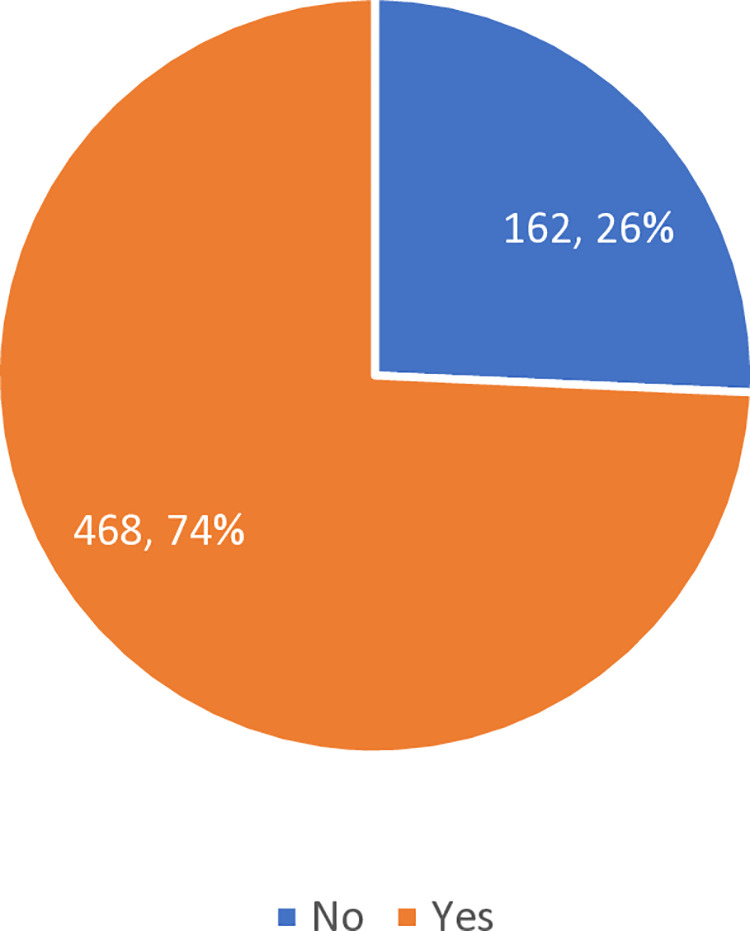 Fig 3
Fig 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhysical Activity and Health · Obesity, Physical Activity, Diet · Cardiovascular and exercise physiology
Introduction
According to World Health Organization, globally around 1.4 billion adults are physically inactive. Around one-fourth of men and one-third of women worldwide do not engage in sufficient physical activity to maintain their health. WHO describes physical activity “as any bodily movement produced by skeletal muscles that requires energy expenditure” [1]. Exercise influences cognitive functioning in the brain and well-being in regard to mental and physical health [2]. A minimum of between 150–300 minutes of moderate physical activity per week or 75–150 minutes of intense physical activity per week is recommended in order to avoid weight gain, increase weight loss and boost physical fitness [3]. Physical activities include walking, sports, cycling, running, weight-lighting, stretching exercises [1]. Lack of physical activity is known to be a modifiable risk factor for cardiovascular disease and chronic illnesses that includes obesity, cancer, diabetes, hypertension, depression, osteoarthritis and osteoporosis [4]. A study conducted among 76 countries between 2002 and 2004, found that around 21.4% are not physically active [5]. In 2016, 27.5% of adults worldwide were physically inactive [6]. In the MENA and Central Asia regions, 32.8% adults are physically inactive [7]. In Arab countries, the prevalence of physical exercise varied from 34.2 to 96.9% [8]. In the UAE adult population, around 58% are physically inactive [9]. From 2017–2021, 19% school children in UAE obtained the necessary level of moderate to vigorous physical activity [10]. According to DCD survey in Abu Dhabi, around 37.7% respondents met recommendations of WHO for physical activity [11].
Regular physical exercise reduces the risk of cardiovascular diseases for both women and men [12], but it’s also known for exercise related deaths in asymptomatic individuals from the rupture of atherosclerotic plaque in a coronary artery, leading to acute thrombosis [13,14]. In sports related to male marathon runners, mostly cardiac arrest is often linked to atherosclerotic coronary artery disease or hypertrophic cardiomyopathy [15]. Muscle injuries are the most prevalent type of injury in sports, accounting for 10–55% of all the injuries [16]. Improved fitness levels can help slow down the progression toward hypertension [17]. For certain individuals, engaging in higher-intensity exercise may yield additional health benefits, whereas others might experience greater advantages from lower-intensity activities performed over a longer duration [18]. According to ACSM (American College of Sports Medicine) guidelines for exercise testing and prescription, exercise related event risk like sudden cardiac death or Acute Myocardial infarction is higher in individuals with factors of vigorous intensity PA, and/ or unaccustomed PA [19]. The American College of Sports Medicine recommends incorporating resistance training as a supplementary component to an aerobic-based exercise program to help reduce blood pressure [20]. To ensure clarity for patients, minimize the risk of injury and maintain the effectiveness of exercise. The healthcare providers should approach exercise as a carefully prescribed intervention, as related to medications.
Pre-exercise screening is carried out to identify individuals who may have conditions that increase their risk of experiencing a negative outcome during physical exercise or activity. It is a safety net that helps to assess if the potential benefits of exercise outweigh the hazards for an individual [21]. In 2010, three national organizations- ESSA (Exercise and Sports Science Australia), SMA (Sports Medicine Australia) and FA (Fitness Australia) collaborated to standardize pre-exercise screening in the Australian health and fitness industry. Many fitness industries have used several screening tools which are adopted from international organizations like the Canadian PAR-Q or the American College of Sports Medicine’s risk stratification system. In 2011, three Australian organizations created the Adult Pre-Exercise Screening System (APSS) and its basic equipment, the Tool (APSS Toll) [22]. The ACSM recommendations have replaced the risk factor evaluation with an algorithm that stratifies first by present physical activity level, then by chronic illness presence and/or symptoms and then finally by desired exercise intensity [23]. Despite its importance, there are significant gaps in the implementation and awareness of effective screening protocols worldwide. This disparity is evident in various regions, particularly in developing countries, where financial constraints and lack of knowledge hinder the adoption of standardized practices.
Methods
The research aims to explore the utilization of pre-screening among physical activity facilities users in Ajman, UAE, through a cross-sectional study design. It targets adult users of such facilities, focusing on those who are registered, over 18 years old, of any gender or nationality, and excludes those unwilling to participate. A sample size of 426 participants is calculated based on existing literature [24], factoring in a nonresponse rate and utilizing convenience sampling for recruitment.
The study employed a self-administered questionnaire to gather data on socio-demographic characteristics, literacy on physical activity, and practice details including type, frequency, and duration of physical activity, as well as use of pre-exercise screening from 17 June 2023–19 February 2024. This instrument underwent face and content validation by experts, followed by a pilot test.
Ethical considerations for the study included obtaining approval from the Gulf Medical University Institutional Review Board (IRB-COM-STD-103-May-2023), ensuring participant consent, maintaining anonymity, and upholding voluntary participation, with no risk to participants. The study proceeded with IRB approval, obtained permissions from relevant facilities, and data collection was carried out using an online Google questionnaire form. This method was chosen for its feasibility, considering the short response time required, lack of harm to participants. Consent was obtained digitally through participants’ explicit selection of “Yes” or “No” to indicate their agreement to participate in the online questionnaire. The consent process was witnessed by the data collection team to ensure transparency and compliance.
Data will be securely stored for three years and analyzed using SPSS for descriptive and inferential statistics, with significance set at a p-value ≤ 0.05.
Results
A total of 630 responses were collected from adults using physical activity facilities in the UAE. Table 1 presents the demographic characteristics of the participants. Among them, 496 (78.7%) were unemployed, and 134 (21.3%) were employed. The gender distribution was relatively balanced, with 329 (52.2%) females and 301 (47.8%) males. The majority of participants were aged 30 years or older (527; 83.7%), and most were single (522; 82.9%). Regarding education, 409 participants (64.9%) had education beyond high school, 210 (33.3%) had a high school education, and only 11 (1.7%) had education below high school level.
Table 1: Distribution of sociodemographic variables.
Fig 1 illustrates the self-reported utilization of pre-exercise screening among participants. Of the 630 respondents, 377 (60%) reported not utilizing pre-exercise screening, 186 (30%) indicated they utilized it, and 67 (11%) were unsure of their use of pre-exercise screening.
Distribution of participants according to self-reported pre-exercise screening utilization.
Table 2 summarizes the association between pre-exercise screening utilization and participants’ sociodemographic characteristics. Significant associations were found for employment status (P < 0.01), gender (P < 0.05), age category (P < 0.01), and educational level (P < 0.05), while marital status showed no significant relationship.
Table 2: Association between pre-exercise screening utilization and Sociodemographic characteristics.
Employed participants were more likely to have undergone screening (40.3%) compared to unemployed participants (26.6%). Males reported higher screening rates (33.9%) than females (25.5%). Participants over 30 years old had notably higher utilization (44.9%) than those aged 30 or younger (26.7%). Screening rates also increased with higher educational attainment, with those above high school reporting the highest utilization (33.5%).
These findings highlight the influence of sociodemographic factors on engagement with pre-exercise health screenings and point to the need for targeted awareness efforts among lower-participating groups.
S1 Table shows participants’ responses to the General Health Questions of the Physical Activity Readiness Questionnaire (PAR-Q+). Among participants, the most commonly reported health issues were dizziness or loss of balance (18.4%), musculoskeletal problems (15.9%), chest pain (15.6%), heart conditions or high blood pressure (13.3%), other chronic conditions (11.7%), use of prescribed medications (10.8%), and advice to engage only in medically supervised physical activity (8.9%).
Table 3 displays the association between participants’ responses to the PAR-Q+ general health questions and their utilization of pre-exercise screening. Across all seven health-related questions, statistically significant associations were observed (all P < 0.001).
Table 3: Association between pre-exercise screening utilization and PARQ+ General health questions.
Participants who reported health conditions—including heart conditions or high blood pressure (52.4%), chest pain (48.0%), dizziness or loss of consciousness (50.9%), other chronic conditions (54.1%), prescribed medications (52.9%), musculoskeletal issues (43.0%), and recommendations for medically supervised activity (66.1%)—were significantly more likely to have undergone pre-exercise screening than those who did not report these conditions.
These findings suggest that individuals with existing or perceived health risks are more inclined to participate in pre-exercise screening, underscoring the role of perceived medical vulnerability in health behavior decisions.
Fig 2 depicts the results of the General Health Assessment based on the PAR-Q+ responses. Of the 630 participants, 401 (64%) were cleared for physical activity, while 229 (36%) requiring further evaluation due to medical conditions or health concerns.
Results of General Health Assessment based on Physical Activity Readiness Questionnaire for everyone (PAR-Q+).
S2 Table shows that the most common follow-up health issues were arthritis, osteoporosis, or back problems (11.4%), followed by mental health or learning difficulties (6.8%), metabolic conditions (6.1%), other or multiple conditions (7.7%), respiratory diseases (5.2%), spinal cord injuries (4.2%), and stroke (3.4%).
Table 4 shows the association between pre-exercise screening utilization and participants’ responses to the follow-up health questions of the PAR-Q + . Significant associations (P < 0.05 or lower) were observed for all listed conditions.
Table 4: Association between pre-exercise screening utilization and PARQ+ follow-up health questions.
Participants reporting specific medical conditions—such as spinal cord injury (72.7%), stroke or TIA (73.7%), cancer (72.7%), high blood pressure (60.0%), heart or cardiovascular disease (62.5%), and respiratory conditions (55.2%)—had substantially higher rates of pre-exercise screening utilization compared to those without these conditions. Elevated screening rates were also noted among individuals with metabolic conditions (52.9%), mental health problems or learning difficulties (50.0%), arthritis or back problems (40.6%), and those with multiple or unlisted medical conditions (48.8%).
These findings indicate that individuals with more serious or multiple health conditions are significantly more likely to undergo pre-exercise screening, reflecting greater awareness or healthcare referral among higher-risk groups.
Fig 3 highlights the participants’ opinions on mandatory pre-exercise screening. A significant majority, 468 (74%), were in favor of making pre-exercise screening mandatory, while 162 (26%) were opposed.
Participants’ stance on making pre-exercise screening mandatory.
These findings emphasize the need for increased awareness of pre-exercise screening practices and suggest that mandatory screening could potentially improve safety and health outcomes for individuals engaging in physical activity.
Table 5 presents the association between participants’ stance on making pre-exercise screening mandatory and their actual utilization of such screenings. A statistically significant association was found (P < 0.05). Participants who supported mandatory screening were more likely to have undergone pre-exercise screening (32.7%) compared to those who opposed it (20.4%), while those who opposed the mandate also reported the highest rate of non-utilization (68.5%). These results suggest that positive attitudes toward policy-level screening requirements may be linked to greater personal engagement in screening behavior.
Table 5: Association between pre-exercise screening utilization and Participants’ Stance on Making Pre-Exercise Screening Mandatory.
Discussion
Demographic factors play a significant role in shaping health practices. Abd-Allatif conducted a comparative study on physical activity among UAE migrants, which revealed trends similar to those found in our study. However, their findings highlighted key differences, particularly in terms of employment status and health risks. Our, UAE participant facility users had high unemployment rates (see Table 1), while the migrant study participants were all employed, with many working in either physically demanding or sedentary jobs [25]. While high unemployment may limit access to fitness resources among UAE participant facility users, migrant workers face health risks tied to the physical demands of their jobs. Notably, employed participants in our study (40.3%) were more likely to undergo pre-exercise screening compared to unemployed participants (26.6%) (P < 0.01) (see Table 2). Thus, socioeconomic factors influence both groups, but in opposite ways: one group faces economic obstacles, while the other faces occupational health hazards.
Beyond socioeconomic factors, age emerged as another significant influence on physical activity behaviors, with notable differences observed between the younger and older participants. Our study, participant facility users were predominantly young, with 84.4% under 30 (Table 1), while over age 30 (44.9%) showed significantly higher pre-exercise screening utilization (P < 0.01) (Table 2). Young age group is typically more open to physical activity, which contrasts with other study done in UAE among the older migrant cohort [25]. In our study, female consists of 52.2%, while male 47.8% in contrasts with migrant study where participants averaged 34 years for males and 33.6 years for females. Despite their youth, the migrant group faced barriers, such as long working hours and limited leisure time, which hindered their ability to engage in regular exercise [25]. Additionally, Males (33.9%) utilized pre-exercise screening more than females (25.5%) (P < 0.05) (Table 2).
Marital status also had implications for exercise habits. Among participant facility users, 82.9% were single, indicating fewer family responsibilities and more time for exercise. This pattern aligns with the migrant study, which found that single individuals living in shared accommodations tended to engage more in physical activity [25]. Such findings highlight how family obligations and cultural expectations can influence fitness priorities. This is particularly true for women across diverse global settings. In the UAE, cultural expectations often dictate family roles and responsibilities, which can limit opportunities for women to engage in physical activity due to pressure to prioritize family over personal health.
Educational attainment revealed 64.9% of UAE participant facility users had post-secondary education (Table1), while it’s noted that higher education levels in migrant UAE study correlated with physical inactivity levels [25]. Although Higher education was associated with greater screening utilization, with participants above high school (33.5%) more likely to use screening than those with lower education levels (P < 0.05) (Table 2). This demonstrates that, despite education, financial and social factors may be stronger determinants of health behaviour.
The findings underscore significant challenges impacting both pre-exercise screening and physical activity participation. Addressing these issues requires tailored interventions that account for socio-economic, occupational, and cultural factors. Comparative analysis between the two groups can further inform the development of targeted, stratified interventions to effectively meet their distinct needs.
While demographic factors provide context for physical activity habits, the issue of pre-exercise screening is equally critical. The data presented in Fig 1 highlights a concerning 60% non-utilization rate for pre-exercise screenings, with 30% of participants reported the use and 10% unaware of its existence. This finding reveals significant gaps in both health awareness and institutional support in the UAE. These findings align with Herbert, reported only 18% using preparticipation screening in U.S. university fitness facilities [26] while our study indicates an even higher level of disengagement. Furthermore, the 10% of participants unaware of screening highlights a global challenge in effectively communicating health protocols. In Australia, a nationwide self-reported survey of fitness professionals on use of Adult pre exercise screening system (APSS) found that only 20% used the screening extremely frequently, while 45% used it infrequently [27]. Institutional readiness appears to be a key differentiator. While the UAE’s 30% utilization rate demonstrates relatively higher individual compliance, it also highlights systemic shortcomings. Moving forward, transitioning the responsibility from individuals to institutions—by making screenings mandatory and integrated into the membership process for all members—could significantly improve overall health outcomes.
Key health issues that influence physical activity preparedness are highlighted in S1 Table, which displays the PAR-Q+ data. These included dizziness (18.4%), joint problems (15.9%), chest pain (15.6%), cardiac ailments or hypertension (13.3%), chronic diseases (11.7%), and medication use (10.8%). In our study about 18.4% reported dizziness, while such conditions are known to effect adults 15% to 20% yearly with prevalence increasing with age [28]. Randomized controlled trial of 6 month concluded Supervision of Physical therapy guided intervention such as supervised Vestibular rehabilitation therapy (VRT) is highly effective for subjective dizziness with chronic peripheral vestibular disorders [29]. Remarkably, 15.6% of participants reported experiencing chest pain, which is a crucial sign that these people could require adapted exercise regimens, including low-impact exercises, to reduce joint and heart strain. The significance of pre-exercise screenings in identifying high-risk individuals who might need medical examinations or customised exercise regimens to safely participate in physical activity is highlighted by these findings. Globally, similar barriers to physical activity have been reported. For instance, Alsaleh and Baniyasin found that 56.7% of coronary heart disease (CHD) patients in neighbouring Jordan had low physical activity due to discomfort, reflecting the joint issues and chronic conditions observed in our study [30]. In our study 13.3% reported with cardiac ailments or hypertension following 11.7% with chronic diseases. Similarly, a study by Bytyci Katanolli in Kosovo found that individuals with diabetes and hypertension often avoid physical activity due to fear of worsening their health [31]. Fitness professionals and facilities should prioritize strategies like promoting isometric exercise training (IET) as it’s known as antihypertensive alternative [32] with high adherence & 11.2–12.9 mmHg reductions in office systolic BP of healthy adults [33] and expanding healthcare access. These approaches can foster inclusive, evidence-based programs that enhance physical activity readiness and adherence, even in resource-constrained settings.
While our study noted significant association for utilization of pre-exercise screening (see Table 3) with a history of heart conditions or high blood pressure (52.4%) (P < 0.001), participants reporting chest pain (48%), balance issues (50.9%), or other chronic medical conditions (54.1%) (P < 0.001). Also, Use of prescribed medications (52.9%) and musculoskeletal issues (43%) significantly correlated with increased pre-exercise screening utilization (P < 0.001).
Fig 2 that shows 64% of participants were cleared for physical activity, while 36% required further evaluation. But according to UAE National Health Survey 2017–2018 reported that 67.9% of adults aged 18–69 years were overweight (BMI ≥ 25 kg/m2) [34]. While a study among US adults aged 40 years had a notable over 90% recommendation for physician consult by using American Heart Association/American College of Sports Medicine’s Preparticipation Questionnaire (AAPQ) in addition to similar results using Physical activity readiness questionnaire (PAR-Q) [35]. These figures suggest that more attention needs to be paid to the underlying health issues that may prevent full participation in exercise. Following on responses to PARQ+ questions to 36% that were not cleared for PA at initial screening (See S2 Table), 64 (11.4%) of participants reported having Arthritis, Osteoporosis, or Back Problems. Approximately 1.71 billion people worldwide live with musculoskeletal conditions [36]. According to evidence stated by College of Family Physicians of Canada Physical activity series – with a favourable risk to benefit ratio for patients with these conditions, also stating adverse events risk is somewhat higher in specific category of patients thereby emphasis individualized approach [37].
In our study, 38 (6.8%) participants reported having mental health problems or learning difficulties. One study found the prevalence of UAE adults suffering from at least one mental health disorder to be 57.2%, with Anxiety and depression being the most common conditions [38]. A systematic review and network meta-analysis including 218 different studies found that physical activity was an effective treatment for depression, with walking or jogging, yoga, and strength training more effective than other exercises [39].
Merely 34 (6.1%) of the individuals indicated that they had metabolic problems, such as type 1 or type 2 diabetes. A cross-sectional study found the overall prevalence of metabolic syndrome in the UAE to be 37.4% [40], While 16.4% is reported as age adjusted diabetes prevalence in adults (20–79 years) by Diabetes Atlas (International Diabetes Federation- IDF) [41]. The American Diabetes Association has concluded in its position statement that exercise and physical activity should be advised and incorporated into the care plan for all individuals with diabetes to help manage blood sugar levels and promote overall health. Additionally, it lists various groups with specific exercise type, intensity and structuring in accordance with conditions [42].
With our study, second most common heath issue reported condition other than the listed or to having two or more conditions of about 7.7%. Apart from the listed were respiratory disease (5.2%), Cardiovascular conditions (coronary artery disease, heart failure or Rhythm abnormality) (4.3%), spinal cord injury (4.2%), Cancer of any kind (3.9%), stroke (which included Transient Ischemic Attack (TIA) or Cerebrovascular Accident (3.4%). In Physical activity practice guideline for Americans, disability or chronic health conditions individuals are recommended as per their ability and avoid inactivity, and highlighted to be under care of healthcare provider, additional consult for guidance on amount and type of activity [43]. As seen the participants in our study in Table 4, showing higher screening rate with cancer (72.7%), high blood pressure (60%), or cardiovascular conditions (62.5%) (P < 0.001), while those with mental health problems (50%), strokes (73.7%), respiratory diseases (55.2%), and spinal cord injuries (72.7%) were more likely to undergo pre-exercise screening (P < 0.01 to P < 0.001).
Notably, about 74% were in favour of making pre- screening mandatory with about 32.7% (of 468) utilizing the screening service and 20.4% (of 162) of opposed not in favour also utilizing if made mandatory (see Table 5). But recent guidelines, such as those from the American College of Sports Medicine (ACSM), have moved towards a more liberal approach as seen in review conducted for community lifestyle intervention program [44]. ACSM states sedentary individuals can commence light to moderate intensity exercise program, and that all individuals should participate in preparticipation screening for exercise. For general population, use of an exercise professional via an algorithm before initiating a moderate to vigorous program by using Physical Activity Readiness Questionnaire Plus (PAR-Q+) [45]. The goal of these revised guidelines is to lower obstacles to exercise engagement while considering the patient’s medical history, intended exercise intensity, current level of physical activity, and the existence of CVD signs and symptoms [45].
Conclusions
Overall, the study reveals that only one-third of participants (186 out of 630) utilized pre-exercise screening before engaging in physical activity. Despite the underutilization, the findings highlight that several factors—such as sociodemographic characteristics, chronic health conditions, and attitudes toward mandatory screening—play a critical role in the adoption of pre-exercise screening. Notably, while all participants were exposed to screening, approximately two-thirds (401 out of 630) were cleared for physical activity, with the remaining one-third (229 out of 630) requiring further evaluation due to health concerns. Addressing knowledge gaps, implementing policies that support mandatory screening, and shifting public attitudes could enhance the uptake of this preventive measure, ultimately improving health safety during physical activity. Additionally, the study finds a significant association between participants’ stance on making pre-exercise screening mandatory and its actual utilization, emphasizing the influence of personal attitudes on screening practices.
Physical activity is a cornerstone of overall health and well-being, offering a myriad of benefits that extend far beyond physical fitness. Regular exercise can lead to significant improvements in cardiovascular health, diabetes management, cancer prevention, and mental health [46]. For optimal results, exercise prescriptions should be personalized, considering factors such as the specific chronic condition, current fitness level, and individual goals. These findings emphasize the need for greater awareness and implementation of pre-exercise screening, as many individuals may have underlying conditions that could affect their ability to safely participate in physical activity in terms of intensity, frequency, duration and mode.
Various forms of exercise and physical activity include such as resistance training for muscle strength and bone density, yoga for flexibility and mental well-being, and aerobic activities for cardiovascular health enabling physical therapists’ role. Collaboration between primary care providers, physical therapists, and fitness professionals is essential for developing safe and effective exercise programs for individuals with chronic conditions in order to keep up with the standards of ACSM. However, there is currently a gap in integration between healthcare and fitness systems. Only 17% of general practitioners participate in formal alliances for stimulating physical activity [47]. This interdisciplinary approach ensures that patients receive appropriate guidance, support, and tailored exercise prescriptions to manage their conditions effectively and improve their overall quality of life.
Limitations
One of the key limitations of this study is not fully represent the broader population’s attitudes or behaviours toward pre-exercise health assessments. Additionally, the study relied on self-reported data, which could introduce biases, as participants might have overestimated or underestimated their engagement in physical activity or health conditions. The cross-sectional design limits the ability to establish causal relationships. Finally, the study was conducted within a specific geographic region (the UAE), which may limit the generalizability of the findings to other regions or populations with different cultural, healthcare, and physical activity contexts. Further research with larger, more diverse samples and longitudinal designs is needed to build a more comprehensive understanding of pre-exercise screening practices.
Supporting information
S1 TableParticipants responses to PARQ+ General health questions.(DOCX)
S2 TableParticipants responses to PAR-Q+ follow-up health questions.(DOCX)
S1 FileExcel Data of the participants.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Physical activity 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/physical-activity
- 2Mandolesi L, Polverino A, Montuori S, Foti F, Ferraioli G, Sorrentino P, et al. Effects of physical exercise on cognitive functioning and wellbeing: biological and psychological benefits. Front Psychol. 2018;9:509. doi: 10.3389/fpsyg.2018.00509 29755380 PMC 5934999 · doi ↗ · pubmed ↗
- 3Niemiro GM, Rewane A, Algotar AM. Exercise and fitness effect on obesity. Treasure Island (FL): Stat Pearls; 2024.30969715 · pubmed ↗
- 4Warburton DER, Nicol CW, Bredin SSD. Health benefits of physical activity: the evidence. CMAJ. 2006;174(6):801–9. doi: 10.1503/cmaj.051351 16534088 PMC 1402378 · doi ↗ · pubmed ↗
- 5Dumith SC, Hallal PC, Reis RS, Kohl HW 3rd. Worldwide prevalence of physical inactivity and its association with human development index in 76 countries. Prev Med. 2011;53(1–2):24–8. doi: 10.1016/j.ypmed.2011.02.017 21371494 · doi ↗ · pubmed ↗
- 6Katzmarzyk PT. Expanding our understanding of the global impact of physical inactivity. Lancet Glob Health. 2023;11(1):e 2–3. doi: 10.1016/S 2214-109X(22)00482-X 36480932 · doi ↗ · pubmed ↗
- 7Chaabane S, Chaabna K, Abraham A, Mamtani R, Cheema S. Physical activity and sedentary behaviour in the Middle East and North Africa: An overview of systematic reviews and meta-analysis. Sci Rep. 2020;10(1):9363. doi: 10.1038/s 41598-020-66163-x 32518254 PMC 7283267 · doi ↗ · pubmed ↗
- 8Murtagh E, Shalash A, Martin R, Abu Rmeileh N. Measurement and prevalence of adult physical activity levels in Arab countries. Public Health. 2021;198:129–40. doi: 10.1016/j.puhe.2021.07.010 34418764 · doi ↗ · pubmed ↗