Innovative Application of a Rigidizing Overtube in Endoscopic Ultrasound–Guided Biopsy for Sampling of a Cecal Submucosal Lesion
Anas Zaher, Nicholas G. Brown

TL;DR
A new technique using a rigidizing overtube improves endoscopic biopsy accuracy for hard-to-reach gut lesions.
Contribution
Demonstrates a novel use of rigidizing overtube technology in endoscopic ultrasound-guided biopsy for cecal submucosal lesions.
Findings
A rigidizing overtube stabilized the colonoscope during endoscopic ultrasound-guided biopsy of a cecal lesion.
The procedure provided a benign diagnosis without requiring surgery.
The method shows potential for safer and more accurate sampling in challenging anatomical locations.
Abstract
Subepithelial lesions in the gastrointestinal tract present diagnostic challenges, particularly in difficult-to-access regions like the cecum. This case report describes a 71-year-old woman with a submucosal lesion adjacent to the appendix, where a rigidizing overtube was used to stabilize the colonoscope for an endoscopic ultrasound–guided fine-needle biopsy. The procedure was successful, obtaining a benign diagnosis without the need for surgery. This case highlights the utility of rigidizing overtube technology in enhancing the accuracy and safety of endoscopic interventions for subepithelial lesions, particularly in anatomically challenging locations like the cecum.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
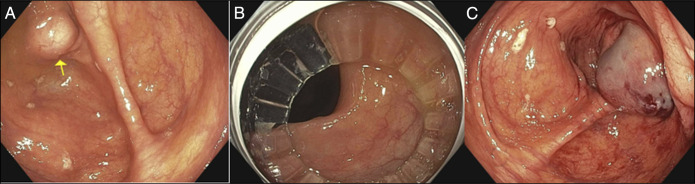 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastric Cancer Management and Outcomes · Gastrointestinal disorders and treatments
INTRODUCTION
Subepithelial lesions (SEL) of the gastrointestinal (GI) tract are often detected incidentally and present unique diagnostic challenges due to their submucosal location.^1^ Endoscopic ultrasound (EUS) has become an essential tool in the assessment and biopsy of these lesions, offering precise visualization and tissue acquisition. Traditionally, in challenging locations such as the cecum, the limited accessibility and stability required for accurate biopsy often necessitated partial surgical resection of the colon. We present a 71-year-old woman who was found to have a submucosal lesion adjacent to the appendix. Using the rigidizing overtube, we successfully performed an EUS-guided fine-needle biopsy (FNB) without the need for surgery. This case demonstrates the potential of rigidizing overtube technology to enable minimally invasive management of complex colonic lesions.
CASE REPORT
A 71-year-old woman with a medical history of hypertension presented to the gastroenterology clinic with persistent abdominal discomfort. For the past 2 years, she had experienced an intermittent, shock-like sensation in the right upper quadrant, occasionally extending to the left upper quadrant. This sensation did not vary with changes in bowel habits or food intake. Her social history was notable for being a nonsmoker and occasional alcohol consumption. She denied any family history of GI malignancy.
Her abdominal exam was unremarkable. Initial workup included a urea breath test for Helicobacter pylori, which returned positive; the patient was subsequently started on appropriate therapy. Further evaluation with colonoscopy revealed a submucosal lesion near the appendix. Tunneled biopsy was performed with cold forceps. However, the histology results showed no malignancy. To better characterize this finding, a computed tomography scan of the abdomen and pelvis with contrast was obtained, which confirmed the presence of a 1.1-cm submucosal lesion adjacent to the appendix orifice.
A multidisciplinary team reviewed the case and recommended further assessment using a through-the-scope probe. Although surgical resection vs endoscopic resection was discussed, the patient expressed a preference to avoid invasive management for the time being.
During colonoscopy, the entire colon was examined and appeared otherwise normal. To facilitate precise imaging and biopsy, a rigidizing overtube was deployed onto the colonoscope and advanced to the cecum, where it was left in place while the colonoscope was exchanged for a linear echoendoscope (Figure 1). The EUS portion of the examination confirmed the presence of a round, intramural (subepithelial) lesion in the cecum, adjacent to the appendix. The lesion appeared hypoechoic, with its origin located within the deep mucosa. It measured approximately 11 mm × 9 mm, with well-defined endosonographic borders.
Endoscopic imaging and procedural views: (A) endoscopic view of the subepithelial lesion in the cecum. (B) Colonoscope inserted through the rigidizing overtube. (C) Post–fine-needle aspiration image showing the biopsy site after a single-pass FNB with a 22-gauge needle.
A fine-needle biopsy was performed using a 22-gauge biopsy needle via a transcolonic approach, yielding a core tissue sample. Cytological examination of the specimen confirmed benign pathology. The procedure was successful, and the patient tolerated it well, leaving without complications.
DISCUSSION
The diagnostic approach to SEL in the GI tract has evolved significantly with advancements in endoscopic tools and techniques. Historically, lesions in difficult-to-access regions, such as the cecum, often required invasive surgical procedures for definitive diagnosis due to limited maneuverability and stability within the colon. The introduction of devices like the rigidizing overtube has revolutionized this field, enabling safer and more effective endoscopic interventions even in anatomically challenging areas.^2^
For submucosal lesions, the American Gastroenterological Association recommends using EUS with fine needle aspiration or fine needle biopsy (FNB) to obtain tissue samples and determine the nature of the lesions. However, assessing SEL in the right colon, including the cecum, poses unique challenges due to anatomical positioning and potential loop formation, making precise needle placement difficult.^2^ The rigidizing overtube (Figure 2) has traditionally been applied in procedures where loop formation is a significant issue, including colonoscopy, enteroscopy, and endoscopic retrograde cholangiopancreatography in patients with altered anatomy. Initially flexible for navigating GI tract bends, the rigidizing overtube stiffens upon vacuum application, creating a stable conduit that maintains the endoscope's position without looping ^3^. This mechanism improves procedural efficiency and safety by reducing repeated scope passes and mitigating procedural fatigue from prolonged manipulation.^4–6^
Rigidizing overtube, single-use flexible overtube.
The safety of the rigidizing overtube has been demonstrated in clinical use. Jawaid et al.^7^ described its application in 97 patients without any device-related adverse events, supporting its role as safe adjunct in complex endoscopic procedures.
According to our knowledge, this is the first reported case in the literature utilizing a rigidizing overtube for FNB of a cecal lesion with EUS guidance. In this case, the use of the rigidizing overtube device facilitated a successful, single-pass FNB with optimal tissue acquisition, allowing for a definitive benign diagnosis. Such advancements underscore the potential of modern endoscopic tools in expanding access to regions of the GI tract previously deemed surgically challenging, offering patients an effective and less invasive pathway to accurate diagnosis and management.
The study's strength lies in its novel use of the rigidizing overtube for EUS-guided FNB of a cecal lesion. However, as a single case report, its findings lack generalizability. Larger studies are needed to confirm its benefits.
DISCLOSURES
Author contributions: A. Zaher: manuscript drafting, chart review and data abstraction, manuscript revision, guarantor of manuscript. NG Brown: manuscript revision. Anas Zaher is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Menon L Buscaglia JM. Endoscopic approach to subepithelial lesions. Therap Adv Gastroenterol. 2014;7(3):123–30.10.1177/1756283 X 13513538 PMC 396881624790643 · doi ↗ · pubmed ↗
- 2Yung E. Use of overtubes in diagnostic and therapeutic endoscopy. Curr Gastroenterol Rep. 2021;23(5):142–8.
- 3Sharzehi K Sethi A Savides T. AGA clinical practice update on management of subepithelial lesions encountered during routine endoscopy: Expert review. Clin Gastroenterol Hepatol. 2022;20(11):2435–43.e 4.35842117 10.1016/j.cgh.2022.05.054 · doi ↗ · pubmed ↗
- 4Wei MT Hwang JH Watson RR Park W Friedland S. Novel rigidizing overtube for colonoscope stabilization and loop prevention (with video). Gastrointest Endosc. 2021;93(3):740–9.32739483 10.1016/j.gie.2020.07.054 · doi ↗ · pubmed ↗
- 5Kim H. Rigidizing overtube in gastrointestinal endoscopy: Expanding capabilities in complex cases. Dig Endosc. 2022;34(2):208–15.
- 6Cheng S Brunaldi VO Silva GLR . Endoscopic-ultrasound evaluation and fine needle aspiration with a linear echoendoscope in the cecum: It is possible. Endoscopy. 2019;51(9):e 270-e 271.31083753 10.1055/a-0896-2086 · doi ↗ · pubmed ↗
- 7Jawaid S Aboelezz AF Daba G . Prospective feasibility study of a novel rigidizing stabilizing overtube in the resection of complex gastrointestinal polyps. Endoscopy. 2025;57(1):68–73.38991535 10.1055/a-2350-4059 · doi ↗ · pubmed ↗