Cardiac tamponade due to influenza B infection in a young immunocompetent female: A case report and review of literature
Sreethish Sasi, Fatma Ben Abid, Mohammed Altayeb Alamin, Javed Iqbal, Muna Al-Maslamani

TL;DR
A young, healthy woman developed heart complications from influenza B, highlighting the need for early diagnosis and treatment.
Contribution
This case report adds to the limited literature on influenza B-induced cardiac tamponade in immunocompetent individuals.
Findings
A 22-year-old immunocompetent female developed cardiac tamponade due to influenza B infection.
The patient recovered after treatment with pericardiocentesis, oseltamivir, and anti-inflammatory drugs.
The case emphasizes the importance of considering influenza as a cause of acute cardiac complications.
Abstract
Influenza infections are recognized globally for their respiratory manifestations, but are less commonly associated with severe cardiovascular complications such as cardiac tamponade. The relationship between influenza infections, particularly influenza B, and cardiac complications such as myocarditis, pericarditis, and cardiac tamponade remains underexplored, particularly in immunocompetent individuals. We report the case of a 22-year-old immunocompetent female who presented to the emergency department with acute shortness of breath, fatigue, and dizziness due to symptoms suggestive of an influenza-like illness. Laboratory and imaging findings revealed a large circumferential pericardial effusion suggestive of cardiac tamponade. Subsequent investigations confirmed influenza B infection. The patient was managed with pericardiocentesis, oseltamivir, nonsteroidal anti-inflammatory drugs,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
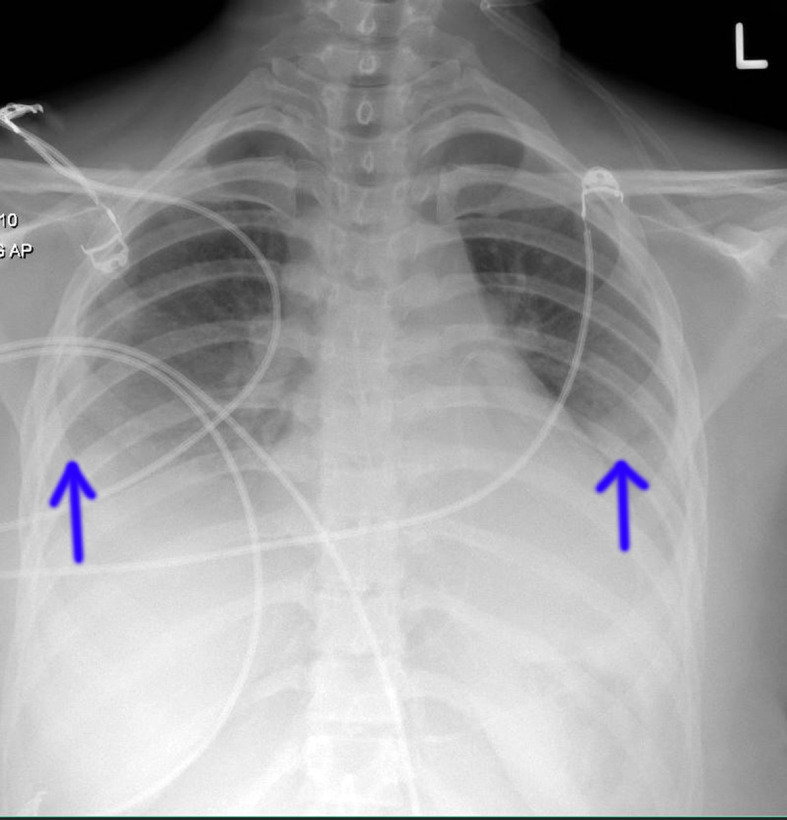 Figure 1
Figure 1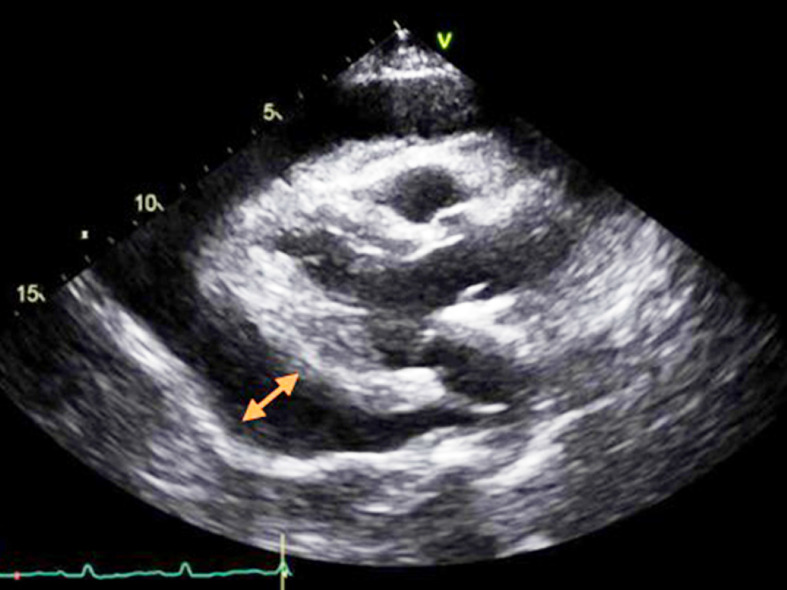 Figure 2
Figure 2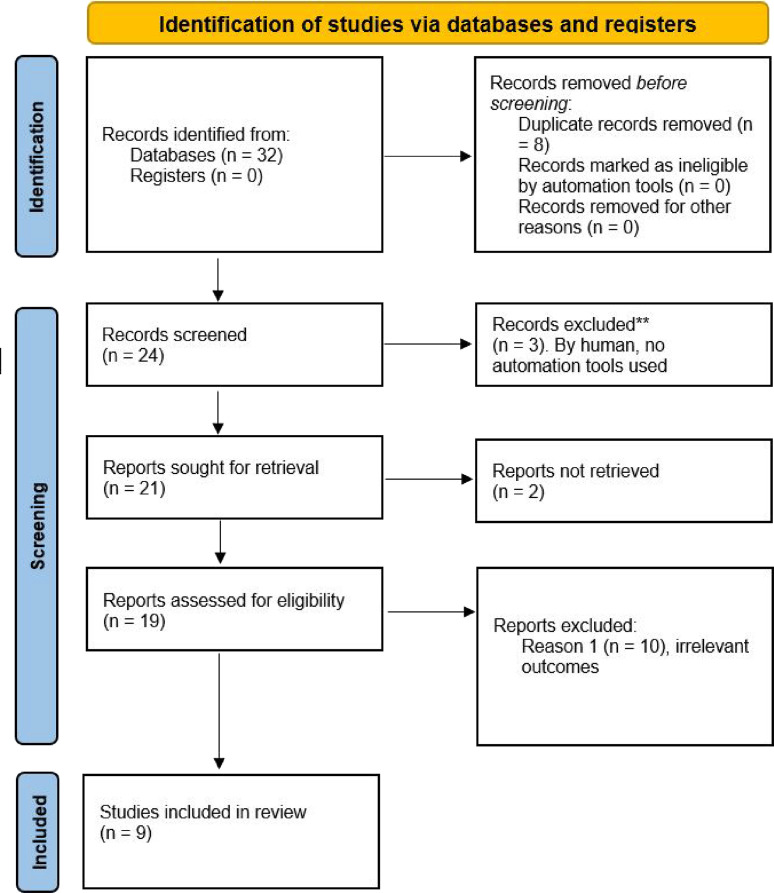 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Viral Infections and Immunology Research · Cardiovascular Effects of Exercise
Introduction
Influenza infections represent a significant global health concern, causing a variety of symptoms ranging from mild, self-limiting infections to severe respiratory failure and death.^ 1 ^ The causes of these complications are poorly understood, with both host- and virus-specific factors being involved.^ 1–3 ^ Severe pneumonia and respiratory failure often occur after influenza infections.^ 1,2 ^ The ability of influenza viruses to spread to distant organs and cause tissue damage outside the lungs is also not fully understood.^ 1,2 ^ Cardiac involvement in influenza infections is rare, with influenza myocarditis typically presenting as a mild, self-limiting disease.^ 2 ^ Fulminant shock is rarely reported, and there are only a few case reports of cardiac complications due to influenza B infections in adults.^ 1–6 ^ Influenza viruses affect the upper and lower respiratory tracts, leading to increased morbidity and mortality. Although cardiovascular complications are rare, studies suggest an association between influenza and increased cardiovascular mortality, particularly during the flu season.^ 3,4,7 ^ Primary cardiac pathologies such as myocarditis, pericarditis, pericardial effusion, and cardiac tamponade caused by influenza B are not well defined.^ 8 ^ Understanding the clinical characteristics, diagnostic approaches, treatment strategies, complications, and outcomes of patients with influenza-related myopericarditis or isolated pericarditis is crucial due to the annual public health burden of influenza. Cardiac tamponade, a life-threatening condition, can occur as a complication of influenza B infection,^ 1–9 ^ highlighting the need for comprehensive data on demographic and clinical characteristics as well as management strategies to reduce mortality in high-risk patients. Hamad Medical Corporation (HMC) is the primary healthcare provider for secondary and tertiary care for almost 3 million people in the State of Qatar (10). It has 14 general and specialty hospitals with a bed capacity of nearly 2,500, multiple specialized outpatient services, and national electronic medical records (10). The publication of this case report was approved by the IRB (Institutional Review Board), Medical Research Centre (MRC) of HMC (approval no. MRC-04-24-160). Written and informed consent was obtained from the patient for the publication of her case information and images.
Case Presentation
A 22-year-old Qatari woman presented to the emergency department of Hamad General Hospital, Doha, Qatar, in November 2023 with acute shortness of breath, fatigue, and dizziness after suffering from fever, vomiting, and watery diarrhea for three days. She had no relevant medical, surgical, family, or psychosocial history. She was found to have respiratory distress, with a respiratory rate of 28 breaths per minute, room air oxygen saturation of 92%, a heart rate of 110 beats per minute, and a blood pressure of 100/70 mmHg. Laboratory investigations revealed an elevated white blood cell count of 13 × 10^ 9 ^ per liter, a C-reactive protein level of 2.7 milligrams per liter, and a procalcitonin level within normal limits. A chest X-ray revealed bilateral obliteration of costophrenic angles, more pronounced on the right side, and haziness in both lower lung fields (Figure 1). Transthoracic echocardiography (TTE) showed a large collection anterior to the right ventricular free wall, a variation in transmitral valve flow of more than 25%, a non-collapsing inferior vena cava (right atrial pressure between 5 and 10 mmHg), a systolic collapse of the right atrium, and right ventricular early diastolic collapse suggestive of cardiac tamponade (Figure 2). The left ventricular ejection fraction was 49%. Pericardiocentesis was performed and 400 milliliters of pericardial fluid was aspirated. It was a straw-colored fluid with a clear appearance. The white blood cell count in the fluid was increased to 211 cells per microliter, predominantly consisting of monocytes (90%) and a small percentage of lymphocytes (8%). Viral panel analysis of the pericardial fluid revealed negative results, and autoimmune workup, including serological tests, was unremarkable. A nasopharyngeal and throat swab was positive for influenza B, while all other respiratory pathogen polymerase chain reaction (PCR) tests were negative. The patient was promptly started on oseltamivir, nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, and supportive care. Her condition improved, and she was discharged after a week of hospitalization. Viral myocarditis was considered as part of the differential diagnosis, but given the clinical improvement after pericardiocentesis and medical therapy, further evaluation with cardiac MRI was not pursued. Serial testing of cardiac troponin was performed and was within normal limits. A clinical follow-up was performed one week after hospital discharge, during which the patient was asymptomatic and a TTE showed an EF (Ejection Fraction) of 55% without pericardial effusion.
Discussion
The case presented highlights the importance of considering influenza infections as a potential cause of acute cardiac complications, particularly in young adults with respiratory symptoms. Influenza viruses are well known for their respiratory manifestations. However, their association with cardiac complications, although rare, can significantly impact patient outcomes and requires prompt recognition and management.
Pericardial effusion and cardiac tamponade, as observed in this case, are rare complications of influenza infections, especially in the absence of underlying cardiovascular disease. A literature review was conducted using a systematic approach, focusing on studies of cardiac tamponade associated with influenza B infection. We searched PubMed, Scopus, and Google Scholar for articles published between 2000 and the present, using keywords such as “Influenza B”, “cardiac tamponade”, and “viral myocarditis”. We included peer-reviewed case reports and reviews that specifically addressed cardiac complications associated with influenza B in immunocompetent individuals. Articles were screened for relevance, and data on patient demographics, clinical presentation, diagnosis, treatment, and outcomes were extracted and analyzed. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for the literature search is shown in Figure 3. The findings were synthesized to identify patterns and inform the discussion in the manuscript. While the exact mechanism of influenza-induced cardiac involvement remains unclear, several hypotheses have been proposed.^ 2–10 ^ Direct viral invasion of cardiac tissue leading to myocarditis, systemic inflammation triggered by the viral infection, and immune-mediated responses have been identified as potential pathways leading to pericardial effusion and tamponade.^ 3,8,9 ^ TTE played a pivotal role in the diagnosis and management of the patient by revealing a large circumferential pericardial effusion with signs of cardiac tamponade. Prompt pericardiocentesis, taking into account echocardiographic findings, was crucial for relieving cardiac compression and preventing further hemodynamic compromise. Detection of influenza B virus in respiratory samples highlights the importance of considering viral etiologies in patients with acute respiratory symptoms, especially during the influenza season. Timely initiation of antiviral therapy with oseltamivir likely contributed to the patient's favorable outcome by reducing viral replication and limiting disease progression. Although pericardial fluid analysis did not reveal viral presence, negative results do not rule out influenza-induced pericarditis because viral shedding in the pericardial fluid may occur intermittently or at low levels. Additionally, the absence of autoimmune markers suggests that the pericardial effusion was likely a consequence of the viral infection rather than an autoimmune-mediated process. A comparative analysis of our case with existing cases of influenza related cardiac tamponade in the literature is summarized in Table 1. A statistical analysis of the cases presented shows an unequal distribution between influenza A and influenza B infections (95:39). The outcomes vary, with a higher recovery rate of 75% compared to a fatality rate of 25%. Pericardiocentesis was performed in all cases, indicating its widespread use as a therapeutic intervention. The most commonly administered medical treatment was oseltamivir, which was used in all cases. Broad-spectrum antibiotics were also used frequently,^ 1,5,6 ^ while other treatments such as NSAIDs, corticosteroids, and colchicine^ 1,2,8 ^ were used less frequently. This analysis underscores the importance of tailored medical interventions in managing influenza-related complications, highlighting the variability in treatment approaches across different cases. Prospective studies investigating the long-term cardiovascular sequelae of influenza infections are needed to better understand the implications of influenza on cardiac health beyond the acute phase of the illness.
The case highlights the importance of TTE in diagnosing large circumferential pericardial effusion with signs of cardiac tamponade, as recommended by the European Society of Cardiology (ESC) guidelines.^ 11,12 ^ TTE is the first-line imaging modality for diagnosing pericardial effusion and cardiac tamponade, and the guidelines recommend immediate management with pericardiocentesis to relieve pressure from cardiac tamponade.^ 11,12 ^ Management of pericarditis, including antiviral therapy with oseltamivir, NSAIDs, and colchicine, is in accordance with the ESC guidelines for the treatment of viral pericardial disease. The manuscript's approach to providing supportive care and detailed follow-up, demonstrating improvement and resolution of pericardial effusion, is consistent with comprehensive care strategies recommended by the ESC, particularly in the acute phase of the disease.^ 11,12 ^
Conclusion
This case report highlights the importance of considering influenza B as a potential cause of severe cardiac complications, even in young and otherwise healthy individuals. The successful management of cardiac tamponade in this patient highlights the critical role of timely diagnosis and intervention, particularly the use of TTE and pericardiocentesis. The patient's complete recovery following antiviral therapy, NSAIDs, and colchicine further emphasizes the effectiveness of early and appropriate treatment strategies. As influenza can lead to life-threatening cardiac conditions, healthcare providers should maintain a high index of suspicion during the influenza season. This case adds to the growing body of literature on influenza-induced cardiac complications and serves as a reminder that vigilance and prompt treatment are required in such cases.
List of abbreviations
Competing interests
The authors have no conflicts of interest to declare.
Authors' contributions
SS conceptualized the study, drafted and revised the manuscript, and gave final approval. FBA, MAA, and JI conducted literature reviews and analyses, critically revised the manuscript, and approved the final version. MAM reviewed and interpreted imaging and laboratory findings, contributed to drafting and revising the manuscript, and gave final approval for publication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roto D Malnoske ML Winters S Georas SNA fatal case of influenza B myocarditis with cardiac tamponade Case Rep Crit Care 2018 Aug 3020188026314 doi: 10.1155/2018/802631430245893 PMC 6136560 · doi ↗ · pubmed ↗
- 2Dumitrescu C Mehta K Singh V When the heart has the flu: influenza B resulting in cardiac tamponade Chest 2019 Oct 156(4)A 803doi: 10.1016/j.chest.2019.08.771 · doi ↗
- 3Pandey Y Hasan R Joshi KP Habash FJ Jagana R Acute influenza infection presenting with cardiac tamponade: a case report and review of literature Perm J 20192318–104doi: 10.7812/tpp/18-104PMC 632655730624200 · doi ↗ · pubmed ↗
- 4Arfaras-Melainis A Cordero H Goyal A Benes L Salgunan R Acute influenza B infection presenting as cardiac tamponade: a case report Cureus 2020 Nov 3012(11)e 11799 doi: 10.7759/cureus.1179933409044 PMC 7779153 · doi ↗ · pubmed ↗
- 5Mir J Mumtaz S Akram A Aamir M Islam MI, Lund J Flu kills: acute influenza B presenting with cardiac tamponade Chest 2021 Oct 160(4)A 398doi: 10.1016/j.chest.2021.07.397 · doi ↗
- 6Schroff P Hovey JR Jagadeesan CT Nagalapuram V Chaucer B Cardiac tamponade secondary to influenza B infection Cureus 2021 May 713(5)e 14888 doi: 10.7759/cureus.1488834109077 PMC 8180197 · doi ↗ · pubmed ↗
- 7Desai R Raina JS Itare V Jain A Singh S Bhuva R Pericardial tamponade in patients with influenza infection: A systematic review of published cases Circulation 2020 Nov 12142(Suppl_3)15587 doi: 10.1161/circ.142.suppl_3.15587 · doi ↗
- 8Radovanovic M Petrovic M Barsoum MK Nordstrom CW Calvin AD Dumic I Influenza myopericarditis and pericarditis: a literature review J Clin Med 2022 Jul 1511(14)4123 doi: 10.3390/jcm 1114412335887887 PMC 9316162 · doi ↗ · pubmed ↗