Stimulant-Related Emergencies in Older Adults
Jonathan S. Zipursky, Rachela Smith, Ania Sarnocinska, Jagadish Rangrej, Inas Riyaz Mohammed, Saad Rais, Kamil Malikov, Michael P. Hillmer, Nathan M. Stall

TL;DR
This study looks at how often older adults visit the emergency room due to stimulant-related issues each year.
Contribution
The study provides annual data on stimulant-related emergency visits specifically among older adults.
Findings
Rates of stimulant-related emergency department visits were analyzed annually.
Older adults showed notable patterns in stimulant-related emergency visits.
Abstract
This cohort study examines annual rates of stimulant-related emergency department visits among older adults.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristics | Visits, No. (%) (N = 1247) |
|---|---|
| Age, median (IQR), y | 69 (67-73) |
| Age group, y | |
| 66-74 | 1031 (82.7) |
| 75-84 | 166 (13.3) |
| ≥85 | 50 (4.0) |
| Sex | |
| Female | 313 (25.1) |
| Male | 934 (74.9) |
| Location of residence | |
| Rural | 102 (8.2) |
| Urban | 1093 (87.7) |
| Neighborhood income, quintile | |
| 1st (lowest) | 579 (46.4) |
| 2nd | 247 (19.8) |
| 3rd | 196 (15.7) |
| 4th | 87 (7.0) |
| 5th (highest) | 86 (6.9) |
| Prescription for psychostimulant | 20 (1.6) |
| Narcolepsy | 0 |
| Parkinson disease | 23 (1.8) |
| ADHD | 8 (0.6) |
| Dementia | 34 (2.7) |
| Mental health | |
| Psychotic disorder | 216 (17.3) |
| Substance use disorder | 687 (55.1) |
| Mood disorder | 415 (33.3) |
| Anxiety disorder | 662 (53.1) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAttention Deficit Hyperactivity Disorder · Pharmaceutical Practices and Patient Outcomes · Medication Adherence and Compliance
Introduction
Most data on substance use in older adults have focused on alcohol, opioids, and cannabis, yet there is a growing concern about stimulant use.^1^ The majority of people born between 1946 and 1964 (commonly referred to as “Baby Boomers”) are now over the age of 65 years, and this generation has historically used substances at higher rates than previous generations. While stimulant-related health care visits have increased among all adults over the last 2 decades,^2,3^ there are limited population-based data on stimulant-related emergency department visits specific to older adults.
Methods
We conducted a population-based retrospective cohort study examining annual stimulant-related emergency department (ED) visits in older adults (aged 66 years or more) between January 2010 and December 2023 in Canada’s most populous province, Ontario (16 million residents). We used linked administrative data from the Ontario Ministry of Health; the primary outcome was the annual rate (per 100 000 population) of ED visits in older adults for stimulant related emergencies. We identified ED visits where International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes corresponding to mental and behavioral disorders or poisoning from cocaine and/or stimulants were listed as the main or contributing reason for the ED visit (eAppendix in Supplement 1). We allowed participants to contribute multiple ED visits to the analysis. We also examined sex, age, medical comorbidities commonly associated with prescription stimulant use, and dispensations for stimulant prescriptions. Data on race and ethnicity were unavailable. All statistical analyses were conducted using SAS version 9.4 (SAS Institute). The study was approved by the Sunnybrook Health Sciences Research Ethics Board and was exempt from informed consent requirements because data were deidentified. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies (eAppendix in Supplement 1).
Results
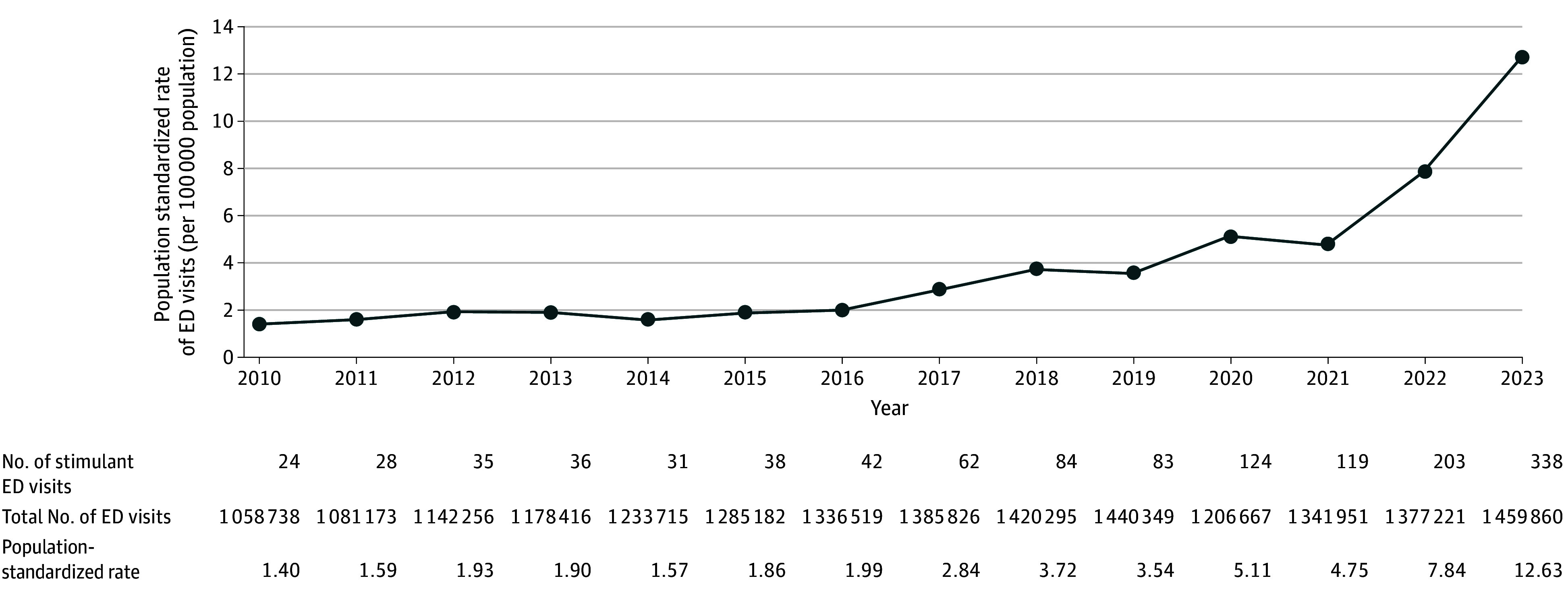
Between 2010 and 2023 there were 1247 stimulant-related ED visits in older adults; median (IQR) age was 69 years (67-73 years), 934 (74.9%) were male, and 579 (46.4%) were in the lowest income quintile (Table). Of the stimulant-related visits, 806 (64.6%) were related to cocaine, 412 (33.0%) to other stimulants, and 29 (2.3%) to both. Rates of stimulant-related ED visits in older individuals increased from 1.4 to 12.6 per 100 000 from 2010 to 2023 (Figure). Among stimulant-related ED visits, 20 (1.6%) were preceded by a prescription fill for a psychostimulant drug within 90 days. In addition, 23 visits (1.8%) occurred in patients with Parkinson disease, 8 (0.6%) with attention deficit hyperactivity disorder, and 34 (2.7%) in people living with dementia. Moreover, 216 visits (17.3%) occurred in patients with a history of psychosis, 687 (55.1%) with substance use disorder, 415 (33.3%) with mood disorders, and 662 (53.1%) with anxiety disorders.
Stimulant-Related Emergency Department (ED) Visits in Older Adults in Ontario, Canada From 2010 to 2023
Discussion
We observed a 9-fold increase in annual stimulant-related ED visits among Ontario older adults between 2010 and 2023. Few patients experiencing stimulant-related ED visits filled prescriptions for psychostimulants or had conditions that are commonly treated with stimulants, and more than two-thirds of ED visits were related to cocaine use. The observed trends may be attributable to increases in recreational stimulant use among older adults (eg, cocaine, amphetamines, ecstasy), the rising prevalence of high potency stimulants in the unregulated drug supply, misappropriation of prescribed stimulants, and growing social acceptance of psychoactive substances. Older adults may be at high risk of adverse drug events from stimulants due to age-related physiological changes, polypharmacy, and multimorbidity.^4^
Study limitations include restricting data to ED visits, which may underestimate the number of stimulant-related poisonings and mental and behavioral disorders.^5^ Some older adults using stimulants may have avoided hospital care or sought care in other settings. Finally, reasons for stimulant use were unavailable.
While the absolute number of ED visits attributable to stimulant toxicity remained low, our study highlights an increasing trend of stimulant-related harms among older adults, especially in lower income men and those with mental health and addictions disorders. Prescription and nonprescription stimulant use have been linked to an increased risk of adverse health outcomes in older adults including hypertension, stroke, myocardial infarction, and arrhythmia.^6^ Overall there is a need for increased stimulant use screening among older adults and enhanced clinical engagement to minimize stimulant-related harms.^4^
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stall NM, Shi S, Malikov K, . Edible cannabis legalization and cannabis poisonings in older adults. JAMA Intern Med. 2024;184(7):840-842. doi:10.1001/jamainternmed.2024.133138767898 PMC 11106709 · doi ↗ · pubmed ↗
- 2Martins D, Greaves S, Tadrous M, . Landscape of Prescription Stimulant Use: Patterns, Trends and Geographic Variation in Ontario, Canada. Ontario Drug Policy Research Network. September 25, 2018. Accessed January 16, 2025. https://odprn.ca/wp-content/uploads/2018/09/ODPRN-Landscape-of-Prescription-Stimulant-Use.pdf
- 3Crispo JAG, Liu L, Bach P, . Amphetamine-related emergency department visits in Ontario, Canada, 2003-2020. Can J Psychiatry. 2023;68(11):838-849. doi:10.1177/0706743723115893336891572 PMC 10590093 · doi ↗ · pubmed ↗
- 4Jones KF, Beiting KJ, Ari M, . Age-friendly care for older adults with substance use disorder. Lancet Healthy Longev. 2023;4(10):e 531-e 532. doi:10.1016/S 2666-7568(23)00174-537804842 PMC 12718471 · doi ↗ · pubmed ↗
- 5Rowe CL, Santos GM, Kornbluh W, Bhardwaj S, Faul M, Coffin PO. Using ICD-10-CM codes to detect illicit substance use: a comparison with retrospective self-report. Drug Alcohol Depend. 2021;221:108537. doi:10.1016/j.drugalcdep.2021.10853733621806 PMC 11008535 · doi ↗ · pubmed ↗
- 6Tadrous M, Shakeri A, Chu C, . Assessment of stimulant use and cardiovascular event risks among older adults. JAMA Netw Open. 2021;4(10):e 2130795. doi:10.1001/jamanetworkopen.2021.3079534694389 PMC 8546494 · doi ↗ · pubmed ↗