Transcorneal electrical stimulation: impact on healthcare and future potential
Takeshi Morimoto

TL;DR
Transcorneal electrical stimulation (TES) is a noninvasive therapy that shows promise for treating retinal and neurological diseases by stimulating retinal cells and protecting them from degeneration.
Contribution
The paper highlights TES's neuroprotective effects and its potential application in both ophthalmology and neurology.
Findings
TES stimulates retinal ganglion cells without activating photoreceptors, enabling evaluation of inner retinal function.
TES has neuroprotective effects via upregulation of neurotrophic factors and reduction of inflammation.
Preliminary evidence suggests TES may benefit neurodegenerative diseases like Alzheimer’s and Parkinson’s.
Abstract
Transcorneal electrical stimulation (TES), a noninvasive therapeutic technique, has gained attention for its potential to treat retinal and optic nerve diseases. TES involves applying weak electrical currents via electrodes on the cornea to stimulate retinal ganglion cells (RGCs) without causing activation of photoreceptors, inducing phosphenes, and enabling the evaluation of inner retinal function. This is valuable for assessing residual retinal activity in patients with photoreceptor or RGC degeneration. Furthermore, TES has shown significant neuroprotective effects on RGCs and photoreceptors through mechanisms involving the upregulation of neurotrophic factors (e.g., insulin-like growth factor 1, brain-derived neurotrophic factor, and ciliary neurotrophic factor), reduction of inflammatory responses, and enhanced ocular blood flow. These findings are supported by extensive animal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
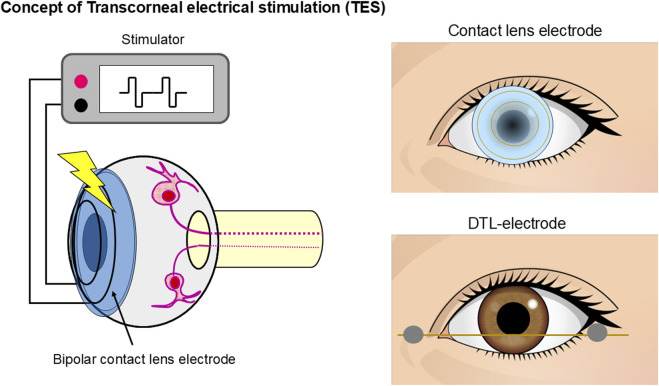 FIGURE 1
FIGURE 1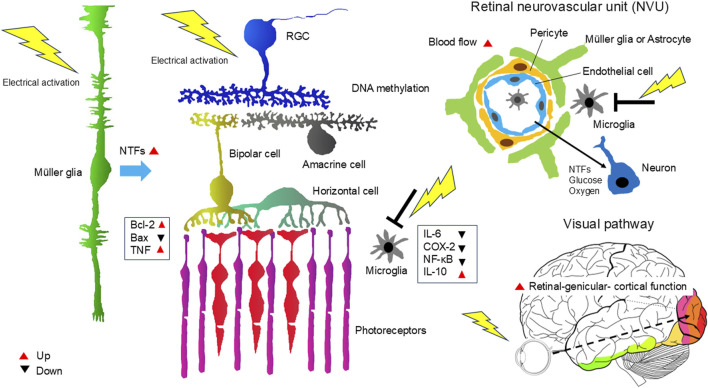 FIGURE 2
FIGURE 2| Study | Subject | Electrode | Parameters | Evaluation method |
|---|---|---|---|---|
|
| Healthy (n = 8) | Contact lens electrode | Monophasic 0.3–2.3 mA, 5.0–50 ms duration | EER |
|
| RP (n = 4) | Contact lens electrode | Monophasic 2.0 mA, 5.0 ms duration | EER |
|
| Healthy (n = 50) | Contact lens electrode | Monophasic, 0.1–2.0 mA, 5.0 ms duration, 1.98 Hz | EER |
|
| IRD (n = 5) | Contact lens electrode | Monophasic, 0.1–2.0 mA, 5.0 ms duration, 1.98 Hz | EER |
|
| CRAO (n = 8) | Contact lens electrode | Monophasic, 0.1–2.0 mA, 5.0 ms duration, 1.98 Hz | EER |
|
| Ocular trauma (n = 17), Healthy (n = 4) | Contact lens electrode | Monophasic, 2.0–20 mA, 1.0 ms duration, 1.0 Hz | EER |
|
| Healthy (n = 23), MH (n = 6), RAO (n = 3) | Contact lens electrode | Monophasic 0.3–2.0 mA 5 ms duration, 1.85 Hz | EER |
|
| IRD (n = 20), Healty (n = 8) | Contact lens electrode | Biphasic, 0.05–2.0 mA, 10 ms/phase, 20 Hz 1.0 s | Subjective phosphene and pupillary reflex |
|
| Healthy (n = 17), POAG (n = 9), RP (n = 14), Amblyopia (n = 3), Homonymous visual field loss (n = 4). | DTL electrode | Monophasic, 0–4.0 mA, 0.05–50.0 ms duration, 0.67 Hz, | Subjective phosphene |
|
| Healty (n = 6), RP (n = 2) | Monopolar scleral electrode | Biphasic, 1.0–1.5 mA, 1.0 ms/phase+interpulse 1.0 ms , 20 Hz, 20 pulses or 0.5–4.0 ms/phase+interpulse 1.0 ms, 50 Hz, 20 pulses | Subjective phosphene and pupillary reflex |
|
| RP (n = 17), Healthy (n = 15) | Contact lens electrode | Biphasic, 0.025–1.0 mA, 5, 7.5, 10 ms /phase, 20 Hz, 2 s | Subjective phosphene, OCT |
|
| Healthy (n = 20), RP (n = 30) ,STG(n = 14), RAO (n = 20), NAION (n = 16), POAG (n = 17) | DTL electrode | Biphasic, 0–10 mA, 1–100 Hz, 5 ms/phase | Subjective phosphene |
|
| RP (n = 40), Healthy(n = 40) | DTL electrode | Biphasic, 0–1.2 mA, 10 ms/phase, 20 Hz | Subjective phosphene and pupillary reflex |
|
| Healthy (n = 14) | DTL electrode | Sinusoidal, 0.01, 0.02,0.05 mA, 10 or 20 Hz, envelope frequency 1.2 Hz | Subjective phosphene and pupillary reflex |
| Study | Animal | Model | Electrode | Parameters | Effect | |
|---|---|---|---|---|---|---|
|
| Wistar rats (ON transection) | TON | Optic nerve monopolar electrodes | Monophasic 0.02–0.07 mA, 0.05 ms duration, 20 Hz 2 h, once | RGC survival | |
|
| Wistar rats (ON transection) | TON | Contact lens electrode | Biphasic 0.1 mA, 0.5–3.0 ms/phase, 20 Hz, 1.0 h, once | RGC survival | |
|
| RCS rats | RP | Contact lens electrode | Biphasic 0.05–0.1 mA, 1.0 ms/phase, 20 Hz, 1 h, once a week for 2–6 wk | PR survival | |
|
| Wistar rats (ON crush) | TON | Contact lens electrode | Biphasic 0.5 mA, 0.05 ms/phase, 20 Hz, 6 h, once | RGC survival | |
|
| Wistar rats (ON transection) | TON | Optic nerve monopolar electrodes | Monophasic 0.05 mA, 0.05 ms duration, 10–50 Hz 10–120 min, once | RGC survival | |
|
| Wistar rats (ON crush) | TON | Contact lens electrode | Biphasic 0.1 mA, 1 ms/phase, 20 Hz, 1 h, 1,2,4,12 times for 12 d | Axonal regeneration of RGCs | |
|
| SD rats (light-induced) | RP | Contact lens electrode | Pre: biphasic 0.1–0.5 mA, 3 ms/phase, 20–100 Hz, 1 hr, once | PR survival | |
|
| Wistar rats (ON transection) | TON | Contact lens electrode | Biphasic 0.1 mA, 1 ms/phase, 20 Hz, 1 h, once | RGC survival | |
|
| SD rats(high IOP) | ION | Contact lens electrode | Biphasic 0.3 mA, 3 ms/phase, 20 Hz, 1 h, every 2 d for 2 wk | RGC survival | |
|
| P347L transgenic rabbits | RP | Contact lens electrode | Biphasic 0.7 mA, 10 ms/phase, 20 Hz, 1 h, once a week for 6 wk | PR survival | |
|
| P23H rats | RP | Sintered pellet electrodes, cornea & mouth | Sinusoidal, 4.7 mA, 5 Hz, 30 min, twice a week for 12 wks | PR function (ERG) | |
|
| C57/BL mice(MNU treated) | RP | Contact lens electrode | Biphasic 0.1–0.2 mA, 20 Hz, 1 h, three times for a week | PR survival | |
|
| DBA/2J (D2) mice | Glaucoma | Contact lens electrode | Biphasic 0.1 mA, 1 ms/phase, 20 Hz, 10 min, every 3 d for 8 wk | RGC survival | |
|
| rd10 mice | RP | Sclera electrode | Biphasic 0.05–0.1 mA, 2.5 ms/phase +interpulse 1 ms, 20 Hz, 1 hr, 3 or 5 times for 5 d | PR survival | |
|
| RCS rats | RP | Cornea ring electrode | Biphasic 0.2–0.1 mA, 10 ms/phase, 6 Hz, 2 hr, once a week, 6 times | PR survival | |
|
| rhodopsin knockout mice | RP | Skin electrodes (upper and lower eye lids) | Monophasic, rectangular (0.1 mA, 2–200 Hz, 40 s/cycle, 160 s) + ramp waveform (0.1 mA, 20 Hz, 160 s), 5 d x 2 times | Improvement in retinal function and visual behavior | |
| Study | Subject | Design | Type | Electrode | Parameters | Outcome |
|---|---|---|---|---|---|---|
|
| ION (n = 3), TON (n = 5) | Case series | TES | Contact lens electrode | Biphasic 0.3-2 mA, 10 ms/phase, 20 Hz, 30 min, once | Improvement in VA and VF |
|
| CRAO (n = 2), BRAO (n = 1) | Case series | TES | Contact lens electrode | Biphasic 1.1 mA, 10 ms/phase, 20 Hz, 30 min, once a month for 3 mo | Improvement in VA and VF |
|
| TON (n = 1) | Case report | rtACS | Skin electrode (upper eye lid) | Biphasic, current bursts, <0.6 mA, 10–30 Hz, 30–40-min for 10 d | Increase of detection ability and mean perimetric threshold |
|
| RP (n = 24) | Prospective, randomized, partially blinded study | TES | DTL electrode | Biphasic intensity 66% or 150% of EPT, 5 ms/phase, 20 Hz, 30 min, once a week for 6 wk | Improvement in VF at 150% of EPT |
|
| BRAO (n = 5) | Case series | TES | Contact lens electrode | Biphasic 0.5–0.9 mA, 10 ms/phase, 20 Hz, 0.5 hour, once | Improvement in visual function (mERG, HFA) |
|
| OND (n = 24), OND (placebo, n = 18) | Prospective, randomized, sham controlled study | rtACS | Skin electrode (upper eye lid) | Biphasic, current bursts, <1.0 mA, 5-20 Hz, 20-40 min daily for 10 d | Increase of detection ability |
|
| OND (n = 12), OND (placebo, n = 10) | Prospective, randomized, double-blind, placebo controlled study | rtACS | Skin electrode (upper eye lid) | Biphasic, current bursts, <1.0 mA, 5–20 Hz, 15 min daily for 10 d | Improvement of central visual field |
|
| OND (n = 446) | Open-label, clinical observational study | rtACS | Skin electrode (upper eye lid) | Biphasic, current bursts, <1.0 mA, 5–20 Hz, 25–40 min daily for 10 d | Improvement in VF and VA |
|
| CRAO (n = 10, sham n = 2), BRAO (sham n = 1) | Prospective, randomized, sham-controlled study | TES | DTL electrode | Biphasic intensity 66% or 150% of EPT, 5.0 ms/phase, 20 Hz, 30 min, once a week for 6 wk | Improvement in ERG response (a-wave) at 150% of EPT |
|
| BVMD (n = 1) | Case report | TES | Contact lens electrode | Biphasic 0.17-0.25 mA, 10 ms/phase, 20 Hz, 30 min, 4 times | Improvement in VA |
|
| OND (n = 45), OND (sham, n = 37) | Multicenter, prospective, randomized, double-blind, sham-controlled study | rtACS | Skin electrode (upper eye lid) | Biphasic, current bursts, 125% of EPT, 8–25 Hz, 50 min 10 d within 2 weeks | Improvement in VF |
|
| RP (n = 32), RP (sham, n = 20) | Prospective, randomized, partially masked study | TES | DTL electrode | Biphasic intensity 150% or 200% of EPT, 5 ms/phase, 20 Hz, 30 min per week for 52 consecutive wk | Improvement of retinal function (scotopic b-wave) at 200% of EPT |
|
| RP (n = 7) | Prospective open-label observational study | TES | DTL electrode | Biphasic intensity 150% of EPT or 1.0 mA, 5 ms/phase, 20 Hz, 30 min, once a week for 6 mo, 24 sessions | No improvement in visual function compared to the control eyes |
|
| POAG (n = 3), NTG (n = 2) | Case series | TES | DTL electrode | Biphasic 0.3-0.5 mA, 10 ms/phase, 20 Hz, 30 min, every 3 mo for 11–68 mo | Improvement in VF (POAG) |
|
| RP (n = 7) | Prospective, randomized, controlled study | TES | DTL electrode | Biphasic 0.75 mA, 5 ms/phase, 20 Hz, 30 min, once a week for 6 wk | Prevention of slowly diminishing vision (ETDRS VA, GVF, qCSF) |
|
| RP (n = 10) | Prospective, non-randomized, open-label, uncontrolled study | TdES | Skin electrode (lower eye lid) | Biphasic 1.0 mA, 10 ms/phase, 20 Hz, 30 min, every 2 weeks for 6 sessions | Improvement of ETDRS BCVA and HFA VF |
|
| RP (n = 105) | Single-arm open label interventional safety study | TES | DTL electrode | Biphasic < 1.0 mA, 5 ms/phase, 20 Hz, 30 min, once a week for 6 mo | Transient dry eye symptoms, no serious adverse events, no improvement in visual function |
|
| RP (n = 15) | Prospective, randomized, controlled study | TES | DTL electrode | Biphasic 200% of EPT, 2 ms/phase, 20 Hz, 30 min, once a week for 12 wk | Improvement in BCVA, color vision, mERG(ring1) |
|
| RP (n = 101) | Prospective, randomized, controlled study | TES | DTL electrode | Biphasic 150% of EPT, 5 ms/phase, 20 Hz, 30 min, once a week for 8 wk | Improvement in VA or VF at 1 mo after TES |
|
| LHON (n = 10) | Prospective, non-randomized, open-label, uncontrolled study | TdES | Skin electrode(lower eye lid) | Biphasic 1.0 mA, 10 ms/phase, 20 Hz, 30 min, every 2 wk for 6 sessions | Improvement in VA |
|
| RP (n = 15) | Prospective, randomized, fellow-eye–controlled study | TES | DTL electrode | Biphasic 200% of EPT, 5 ms/phase, 20 Hz, 30 min, once a week for 6 mo | Stabilization of retinal function (mERG) |
|
| RP (n = 31), RP (sham, n = 20) | Prospective, randomized, partially masked study | TES | DTL electrode | Biphasic intensity 150% or 200% of EPT, 5 ms/phase, 20 Hz, 30 min, once a week for 1 yr | Reduction of loss of VF |
|
| ION (n = 5) | Prospective, non-randomized, open-label, uncontrolled study | TdES | Skin electrode (lower eye lid) | Biphasic 1.0 mA, 10 ms/phase, 20 Hz, 30 min, every 2 wk for 6 sessions | Improvement in VA or VF |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroscience and Neural Engineering · Planarian Biology and Electrostimulation · Photoreceptor and optogenetics research
1 Introduction
Electrical stimulation (ES) is a promising therapeutic tool for treating various neurological disorders. Multiple studies have demonstrated significant beneficial effects of ES with optimal safety and feasibility.
Vagus nerve stimulation (VNS) is clinically applied for the treatment of epilepsy, depression, cluster headache, and migraine (Cheng et al., 2022; Austelle et al., 2024). Deep brain stimulation has been applied in clinical practice for over 25 years and is well-established as an effective treatment for Parkinson’s disease (PD), dystonia, and Tourette syndrome (Ranjan et al., 2024).
Transcranial electrical stimulation (tES) has also been extensively investigated to alter brain function noninvasively by applying current to electrodes on the scalp. tES can induce changes in synaptic excitability and is promising for enhancing recovery in patients with stroke (Motolese et al., 2022). In addition, tES is clinically applied for the treatment of Alzheimer’s disease (AD) (Pilloni et al., 2022), Cerebral vasospasm and delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage are the leading causes of morbidity and mortality after aneurysmal subarachnoid hemorrhage (Budohoski et al., 2014). Several types of ES have been tested for the treatment of cerebral vasospasms and delayed cerebral ischemia, including trigeminal/vagus/facial nerve stimulation, sphenopalatine ganglion and spinal cord stimulation, tES, transcutaneous electrical neurostimulation, and electroacupuncture (Powell et al., 2022).
For the retina and optic nerve (ON), transcorneal ES (TES) modulates retinal neurons to evoke light sensations, commonly referred to as “phosphene.” This phenomenon has been utilized to evaluate the residual retinal function in individuals with visual impairments. Furthermore, owing to the neuroprotective effects of TES on injured retinal ganglion cells (RGCs) in vivo (Morimoto et al., 2005), basic and clinical research on TES and related ES methods have significantly progressed over the past two decades. These advancements have established ES as a promising treatment approach for ON and retinal diseases (Morimoto, 2012; Pardue et al., 2014; Tao et al., 2016; Liu et al., 2021; Li et al., 2024).
This review explores the fundamental and clinical studies conducted on TES to date and its potential future applications.
2 History of transcorneal electrical stimulation
ES of the eye can induce a light sensation known as “phosphine,” a phenomenon that later led to the development of retinal prostheses aimed at restoring vision in blind patients with advanced retinitis pigmentosa (RP).
TES is used to stimulate the retina and evoke phosphenes. The procedure involves placing a bipolar contact lens electrode with an inner and outer ring in the form of a contact lens, such as an electroretinogram (ERG) electrode, or DTL-electrode on the patient’s cornea (Figure 1). To stimulate the retina, a weak electric current is then applied through the electrodes. Numerous studies have investigated ES-induced phosphenes. Early research on electrically induced phosphenes primarily focused on psychophysical studies (Motokawa et al., 1951; Brindley, 1960).
Schematic representation of TES. A bipolar contact lens electrode with an inner and outer ring in the form of a contact lens or DTL-electrode was placed on the participant’s cornea. Electric current pulses activate the retinal neurons.
Subsequently, Jarvik and Kopp (1967) developed a more convenient and less invasive method known as TES. TES was then employed in electrophysiological studies to investigate the relationship between ES and phosphene perception. Potts et al. (1968) were the first to report an “electrically evoked potentials (EER)” induced by TES. They found that the latency of EER was shorter than that of the visually evoked potentials, indicating that TES can evoke visual perception even without photoreceptor involvement (Potts et al., 1968; Potts and Inoue, 1969; 1970). Shimazu et al. (1996) and Shimazu et al. (1999) also reported similar findings using experiments with cats.
Subsequently, several human experiments have evaluated the characteristics of EERs in healthy participants (Miyake et al., 1980a; Dorfman et al., 1987; Takei et al., 1993) and patients with various retinal and ON diseases (Miyake et al., 1980b; Miyake et al., 1980c; Dorfman et al., 1987). Studies have reported that the EERs remained nearly normal in patients with functional disorders of the rod or cone visual pathways (Miyake et al., 1980b), whereas they were reduced in patients with central retinal artery occlusion or ON diseases (Miyake et al., 1980c). Despite these findings, basic research on TES made no significant progress, nor did it lead to clinical applications, and studies on TES came to a standstill for some time.
3 TES to assess inner retinal function
The advancement in retinal prostheses and regenerative medicine renders it possible to restore the vision of patients with blindness and retinal degenerative diseases such as RP. For the successful restoration of vision through such treatment, the function of the inner retinal neurons must remain intact.
As the prospect of clinical applications transitions into reality, robust and sophisticated methodologies are increasingly needed to assess residual inner retinal function in patients with blindness (Table 1), particularly those being considered candidates for these transformative treatments.
In particular, patients eligible for treatment often suffer from degeneration-induced photoreceptor loss, which makes it impossible to evaluate inner retinal function using conventional ophthalmic tests such as visual acuity (VA) tests, visual field (VF) tests, ERG, or VEP. The structural evaluation of the inner retinal layers using optical coherence tomography (OCT) is currently the sole method for assessing the inner retinal layers (Chader et al., 2009).
TES is considered an effective method for evaluating inner retinal functions because it can stimulate RGCs without activating photoreceptors (Potts and Inoue, 1970; Miyake et al., 1980b; Shimazu et al., 1999). This has brought TES back into the spotlight, leading to a resurgence of its research starting in the 2000s. A method combining TES-induced phosphenes and pupil responses to evaluate inner retinal function subjectively and objectively in healthy individuals and patients with inherited retinal degeneration has been reported (Morimoto et al., 2006; Kelbsch et al., 2017; Kelbsch et al., 2018).
Methods have been developed to evaluate the function of the inner retinal layers by analyzing the characteristics of ES-induced phosphenes, such as their position, size, shape, brightness, and color (Gekeler et al., 2006; Fujikado et al., 2007; Naycheva et al., 2012). Furthermore, a combined approach integrating OCT for retinal structural assessment with the evaluation of phosphenes was also proposed (Huang et al., 2009).
Given the rapidity, safety, and reliability of phosphene-based evaluation of inner retinal function using TES, this method shows great potential for assessing inner retinal layer function in patients with blindness and inherited retinal degeneration and could become a standard diagnostic test.
In the future, with the wide adoption of regenerative medicine, retinal prostheses, and optogenetic therapies, TES is expected to play an increasingly crucial role in assessing the functionality of the inner retinal layers in patients who have lost photoreceptors.
4 Neuroprotective effects of TES on the retinal neurons
ES can dose-dependently modulate the survival rates of isolated central nervous system (CNS) neurons in vitro (Kaplan et al., 1988). Many studies have investigated the neuroprotective effects of ES on injured neurons in vivo. Within the auditory system, the survival of spiral ganglion cells (SGCs) is a key factor that influences the performance of cochlear implants. Enhancing SGC survival is anticipated to improve sensitivity and enhance auditory discrimination. Chronic ES supported SGC survival that would otherwise degenerate following exposure to ototoxic drugs in vivo (Lousteau, 1987; Hartshorn et al., 1991).
Similarly, in the visual system, brief ES using monophasic pulses on the transected ON increased RGC survival in rats, demonstrating the neuroprotective effect of ES on the ON (Morimoto et al., 2002). Furthermore, the extent of this survival-promoting effect was dependent on the ES parameters (Okazaki et al., 2008).
Direct ES of the ON has demonstrated a neuroprotective effect; however, its highly invasive nature makes its clinical application challenging. Therefore, this study focused on TES, a less invasive and safer stimulation method than ON stimulation, which is also used to evaluate the function of inner retinal layers. This study revealed that TES exerts a neuroprotective effect on RGCs, similar to that of direct ON stimulation. TES increased RGC survival after ON transection in rats by upregulating endogenous IGF-1 (Morimoto et al., 2005). The survival-promoting effect of TES was dependent on ES parameters (Morimoto et al., 2010). TES was also neuroprotective for axons in crushed ONs (Miyake et al., 2007) and enhanced the axonal regeneration of RGCs through the activation of the IGF-1 pathway in the rat ON crush model (Tagami et al., 2009).
Moreover, TES exerts neuroprotective effects on photoreceptors. In animals with inherited photoreceptor degeneration, TES enhanced photoreceptor survival in Royal College of Surgeons rats (Morimoto et al., 2007; Gonzalez Calle et al., 2023), P347L transgenic rabbits (Morimoto et al., 2012), P23H rats (Rahmani et al., 2013), N-methyl-N-nitrosourea-administered mice (Tao et al., 2016), rd 10 mice (Liu et al., 2022), and phototoxic rats (Ni et al., 2009), rhodopsin knockout mice (Enayati et al., 2024). TES also exerted neuroprotective effects on ischemic damaged retinas in vivo (Wang et al., 2011). TES provided RGC axon protection and led to a reduction in inflammatory cells in a mouse glaucoma model (Jassim et al., 2021).
The results of numerous animal experiments have demonstrated the neuroprotective effects of TES in the eyes of patients with retinal degenerative diseases and ON disorders (Table 2).
5 Mechanism of the neuroprotective effects of TES on the retina and ON
The mechanism underlying the neuroprotective effects of ES has been extensively studied over time. As regards the neuroprotective and axonal outgrowth-promoting effects of ES, ES-induced depolarization via the activation of voltage-dependent Ca^2+^ channels is crucial.
Brief periods of ES applied to cultured Xenopus spinal neurons significantly increased intracellular Ca^2+^ and cAMP levels, which, in turn, play a crucial role in promoting the extension of growth cones (Ming et al., 2001). Various neurotrophic factors are reportedly induced by ES applied to RGCs and/or Müller cells, exerting neuroprotective effects in vitro.
RGC stimulation by ES from a silicon chip enhanced their survival and axonal growth in response to brain-derived neurotrophic factor (BDNF) in vitro (Goldberg et al., 2002).
Brief ES of cultured Müller cells increased the gene expression of IGF-1, BDNF, basic fibroblast growth factor (bFGF) (Sato et al., 2008a; Sato et al., 2008b; Sato et al., 2008c), and ciliary neurotrophic factor (CNTF) (Enyati et al., 2020) by activating L-type voltage-dependent Ca^2+^channels.
The neuroprotective effects of TES are considered to involve various neurotrophic and neuroprotective factors that are expressed within the retina in response to TES in vivo. TES enhanced retinal neuron survival by increasing endogenous neurotrophic factors, namely, IGF-1 (Morimoto et al., 2005), BDNF and CNTF (Ni et al., 2009; Tao et al., 2016), and bFGF (Yu et al., 2020). These neurotrophic factors increased significantly in Müller cells, which play a significant role in TES-induced neuroprotection.
Other neuroprotective factors were reported to be related to the neuroprotective effects of TES. Bcl-2 was upregulated, whereas Bax was downregulated (Ni et al., 2009; Tao et al., 2016), and the tumor necrosis factor superfamily was upregulated in the retina after TES (Willmann et al., 2011). DNA methylation changes with therapeutic effects were also induced by TES (Tew et al., 2024).
TES also affects the immune system. TES decreased the number of Iba-1-positive microglial cells, reduced interleukin-6 (IL-6) and COX-2 expression and NF-κB phosphorylation, and increased IL-10 levels (Fu et al., 2018). Microglial inhibition by TES was observed in genetic secondary glaucoma mouse model (Jassim et al., 2021).
Other effects of TES are thought to be associated with increased ocular blood flow. Numerous studies have investigated the potential relationship between TES and retinal blood flow, and growing evidence indicates a significant link. For instance, measurements of TES-induced retinal intrinsic reflective changes in cat eyes have revealed vascular changes caused by the activation of retinal neurons (Mihashi et al., 2011; Morimoto et al., 2014). Similarly, studies assessing blood flow in human eyes have demonstrated that TES increases chorioretinal blood flow in both healthy individuals (Kurimoto et al., 2010) and patients with RP (Bittner et al., 2018a). Furthermore, the TES-induced increase in retinal blood flow involves neurovascular coupling (NVC) (Su et al., 2020).
NVC is a phenomenon in which neurons, glial cells, and blood vessels in the CNS work together. When neurons become active, the blood flow in the corresponding region increases to meet the energy demands of the active neurons by delivering oxygen and glucose. NVC is essential for supporting RGC metabolism and survival (Haider et al., 2022). Many patients with glaucoma suffer from vascular deficits, including reduced blood flow, impaired autoregulation, NVC dysfunction, and breakdown of the blood–retina and blood–brain barriers (Alarcon-Martinez et al., 2023).
Based on the above findings, increased blood flow is inferred to exert a neuroprotective effect on the retina. The TES-induced increase in ocular and retinal blood flow may contribute to this neuroprotective effect.
TES also affects neuronal activity in the visual pathway and ameliorates retinal-genicular- cortical function in diseases involving the visual system (Castoldi et al., 2025).
In summary, TES is thought to exert neuroprotective effects on RGCs and photoreceptors through various mechanisms. These include the production of neurotrophic factors via Müller cells, DNA methylation, modulation of the immune system (e.g., suppression of macrophage activity), and an increase in ocular and retinal blood flow, and amelioration of retinal-genicular- cortical function in ocular diseases involving the visual system (Figure 2).
Mechanism of the neuroprotective effects of TES on the retina and ON. TES triggers various responses that act together to promote neuronal survival and improve neuronal function. These include the production of neurotrophic factors via Müller cells, DNA methylation, modulation of the immune system (e.g., suppression of macrophage activity), and an increase in ocular and retinal blood flow, and amelioration of retinal-genicular- cortical function in ocular diseases involving the visual system. NTFs, neurotrophic factors.
6 Clinical application of TES for various retinal and ON diseases
Numerous clinical studies have examined TES and similar ES therapies for various retinal and ON diseases (Table 3). Initial TES was performed for nonarteritic anterior ischemic optic neuropathy and traumatic optic neuropathy, and some patients reported improvements in VA and VFs (Fujikado et al., 2006). Since then, TES has been applied to diseases, including retinal artery occlusion (Inomata et al., 2007; Oono et al., 2011; Naycheva et al., 2013), Best vitelliform macular dystrophy (Ozeki et al., 2013), ON atrophy (Gall et al., 2010), and glaucoma (Ota et al., 2018). Despite the modest therapeutic effects, positive outcomes were observed, leading to the application of this treatment approach to various ocular diseases.
Clinical studies on the neuroprotective effects of ES, involving many patients, have been conducted for both RP and optic neuropathies. Among these, Schatz et al. (2011) conducted the first randomized controlled trial (RCT) of TES in patients with RP. The study reported the safety of TES in RP patients. and enhancements in the VF area (VFA) and scotopic b-wave amplitude. A continuation of this study revealed a trend toward improved safety and function (specifically scotopic b-wave amplitude) with 1 year of continued treatment (Schatz et al., 2017). Furthermore, regular and dose-dependent use of TES significantly reduced the loss of VFA (V4e) in treated eyes compared with untreated eyes in patients with RP (Stett et al., 2023).
Since then, more RCTs on TES for patients with RP have been conducted. Wagner et al. (2017) demonstrated that TES was safe and well-tolerated in patients with RP. However, visual function measurements at 6 months were not significantly different between the control and treated eyes.
With TES, some patients experienced a significant improvement in VA and VF (Bittner and Seger, 2018b). A single-arm open-label interventional trial involving 105 patients with RP reported an excellent safety profile for TES; however, it did not observe significant improvements in visual function (Jolly et al., 2020). Another single-arm open-label interventional trial with 101 patients with RP found that the mean BCVA and VF test scores improved significantly 1 month after TES initiation. However, these improvements were transient and disappeared after the treatment was discontinued (Sinim Kahraman and Oner, 2020). In addition, single-arm open-label interventional trials have suggested that TES may slow deterioration in multifocal electroretinography (Demir et al., 2022; Dizdar Yigit et al., 2022). Furthermore, RCTs investigating transdermal ES (TdES), a technique similar to TES, in patients with RP demonstrated both safety and significant improvements in VA and VF for up to 3 months (Miura et al., 2019).
In clinical applications of TES and TdES for RP, some patients demonstrate notable improvements in visual function, whereas others do not exhibit significant changes. Such heterogeneity in outcomes is likely attributable to multiple factors, including disease stage and severity, inter-individual anatomical and physiological differences, and variations in stimulation parameters (e.g., current intensity, frequency, duration, and interval of treatment sessions).”
TES has shown potential in improving VA and VF in patients with RP. However, as the underlying disease continues to progress, these improvements may be temporary, eventually giving way to further deterioration in visual acuity and visual field. Therefore, a critical challenge in clinical practice is to develop strategies that can sustain the therapeutic effects of TES and help slow the progression of retinal degeneration over time.
TES has been widely performed for patients with various optic neuropathies. An RCT of repetitive transorbital alternating current stimulation (rtACS), which is similar to TES, for patients with ON damage, such as traumatic optic neuropathy, revealed that rtACS facilitated vision restoration in VA and VF size (Sabel et al., 2011; Gall et al., 2011; Fedorov et al., 2011; Gall et al., 2016).
Preliminary studies have investigated the potential of TdES as a treatment option for optic neuropathies. In a study on Leber hereditary optic neuropathy, 10 patients received TdES over 10 weeks. Significant improvements in VA were observed at all follow-up points, with half of the patients demonstrating notable enhancements in VF sensitivity (Kurimoto et al., 2020). Another study evaluated TdES for nonarteritic anterior ischemic optic neuropathy in five patients treated over 12 weeks. Some cases showed improvements in VA and VF sensitivity without adverse events (Miura et al., 2023).
Despite the relatively few treatment reports on the effects of TES on optic neuropathies (Fujikado et al., 2006), results of previous animal experiments and clinical trials of rtACS suggest the significant potential efficacy of TES for these conditions. Therefore, RCTs are needed to further investigate the therapeutic effects of TES on optic neuropathies.
Finally, regarding the safety of TES treatment, numerous studies to date have reported no serious complications, with only transient dry eye symptoms and punctate superficial keratitis being observed (Jolly et al., 2020; Sinim Kahraman and Oner, 2020). TES induces corneal epithelial damage in mice by disrupting mucin homeostasis (Yang et al., 2022). However, these were mild and all resolved without sequelae (Jolly et al., 2020; Sinim Kahraman and Oner, 2020).
Although potential side effects of TdES treatment—such as keratitis, dermatitis, facial or trigeminal nerve disorders, and nasal abnormalities—were anticipated due to the use of skin electrodes, none of these adverse events were observed during treatment. The skin sensory irritation and discomfort caused by the electrical stimulation were well tolerated by the patients (Kurimoto et al., 2020; Miura et al., 2023).
7 Clinical potential of TES for treating brain disorders
As mentioned earlier, TES stimulates the retina, resulting in phosphene generation in the visual cortex of the brain. Thus, ES of the eye affects the CNS. Because the eyes are an extension of the brain, examining ocular symptoms is gradually becoming a common practice in diagnosing brain pathologies.
Ophthalmological evaluations have revealed that neurodegenerative and neurological diseases, such as AD, PD, and multiple sclerosis, manifest retinal symptoms (Majeed et al., 2021; Chang et al., 2022; Bostan et al., 2023).
To treat these diseases, interest is growing in leveraging the connection between the eyes and the brain for therapeutic interventions. Most forms of ES of the brain are invasive, such as deep brain stimulation and motor cortex stimulation, and often involve postoperative complications. Conversely, noninvasive forms, such as tES and VNS, exhibit significant variability in response to the stimulation (Reed and Cohen Kadosh, 2018).
TES is considered a novel approach for noninvasively stimulating the eye to modulate brain networks in neurodegenerative diseases. TES to the retina modulates the brain coherence and connectivity of the visual and nonvisual cortices, and the observed alterations are largely maintained. TES holds a strong potential to modulate higher cortical functions, including cognition, awareness, emotion, and memory (Agadagba et al., 2022).
In rat models of retinal degeneration and chronic unpredictable stress, TES has shown promising effects, such as promoting antidepressant-like actions and recovering cognitive impairments (Yu et al., 2021; Yu et al., 2022a; Yu et al., 2022b). Despite the lack of basic or clinical research on the therapeutic effects of TES on AD or PD, noninvasive TES shows potential as a tool for modulating brain function in the treatment of brain diseases. This approach offers hope for the future treatment of patients with neurodegenerative diseases.
8 Concluding remarks and future directions
This review summarizes the results of studies on the role of TES as an assessment method of inner retinal layer function in patients with photoreceptor degeneration and as a neuroprotective treatment for retinal and ON diseases. Furthermore, it explores foundational research investigating the potential of TES as a neuroprotective therapy for brain disorders. TES not only influences retinal function by promoting neurotrophic factor production and immunosuppression and increasing blood flow but also affects other brain regions, including the visual cortex and hippocampus. With further clinical advancements, TES shows promise as a therapeutic approach for degenerative conditions of the retina and ON and neurological disorders.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agadagba S. K.Eldaly A. B. M.Chan L. L. H. (2022). Transcorneal electrical stimulation induces long-lasting enhancement of brain functional and directional connectivity in retinal degeneration mice. Front. Cell. Neurosci. 16, 785199. 10.3389/fncel.2022.785199 35197826 PMC 8860236 · doi ↗ · pubmed ↗
- 2Alarcon-Martinez L.Shiga Y.Villafranca-Baughman D.Cueva Vargas J. L.Vidal Paredes I. A.Quintero H. (2023). Neurovascular dysfunction in glaucoma. Prog. Retin Eye Res. 97, 101217. 10.1016/j.preteyeres.2023.101217 37778617 · doi ↗ · pubmed ↗
- 3Austelle C. W.Cox S. S.Wills K. E.Badran B. W. (2024). Vagus nerve stimulation (VNS): recent advances and future directions. Clin. Auton. Res. 34, 529–547. 10.1007/s 10286-024-01065-w 39363044 PMC 11543756 · doi ↗ · pubmed ↗
- 4Bittner A. K.Seger K. (2018 b). Longevity of visual improvements following transcorneal electrical stimulation and efficacy of retreatment in three individuals with retinitis pigmentosa. Graefes. Arch. Clin. Exp. Ophthalmol. 256, 299–306. 10.1007/s 00417-017-3858-8 29222719 PMC 6039224 · doi ↗ · pubmed ↗
- 5Bittner A. K.Seger K.Salveson R.Kayser S.Morrison N.Vargas P. (2018 a). Randomized controlled trial of electro-stimulation therapies to modulate retinal blood flow and visual function in retinitis pigmentosa. Acta. Ophthalmol. 96, e 366–e 376. 10.1111/aos.13581 29130647 PMC 5920686 · doi ↗ · pubmed ↗
- 6Bostan M.Pîrvulescu R.Tiu C.Bujor I.Popa-Cherecheanu A. (2023). OCT and OCT-A biomarkers in multiple sclerosis - review. Rom. J. Ophthalmol. 67, 107–110. 10.22336/rjo.2023.20 37522023 PMC 10385714 · doi ↗ · pubmed ↗
- 7Brindley G. S. (1960). Physiology of the retina and visual pathway. Edward Arnold, 155–160.
- 8Budohoski K. P.Guilfoyle M.Helmy A.Huuskonen T.Czosnyka M.Kirollos R. (2014). The pathophysiology and treatment of delayed cerebral ischaemia following subarachnoid haemorrhage. J. Neurol. Neurosurg. Psychiatry. 85, 1343–1353. 10.1136/jnnp-2014-307711 24847164 · doi ↗ · pubmed ↗