Mismatch Repair-Deficient FIGO Stage IA Endometrial Adenocarcinoma With Negative Nodal Biopsy Presenting as Isolated Orbital Metastasis
Steven B Barker, Aditya Ghosh, Christie Taylor, Shravanti Macherla

TL;DR
A rare case of stage IA endometrial cancer with no lymph node involvement later developed an isolated orbital metastasis, highlighting the need for better risk assessment methods.
Contribution
Presents a rare clinical case of metastasis in a low-stage endometrial cancer patient with negative lymph node biopsy.
Findings
Endometrial cancer recurrence as isolated orbital metastasis is exceedingly rare after complete surgical resection with negative lymph nodes.
Current metastatic assessment methods may miss occult metastatic disease in some patients.
This case emphasizes the limitations of existing risk stratification and the need for improved early detection strategies.
Abstract
Endometrial cancer is the most common malignancy of the female genital tract in the United States and the fourth most common cancer among women worldwide. Recently, the pathological classification of endometrial cancer has expanded from a two-tiered system to a four-group system based on molecular profiling. Typically, metastatic endometrial cancer spreads via the lymphatic system, most frequently to the retroperitoneum. Hematogenous spread is rare but can occur. We present a case of an 82-year-old female with a history of FIGO (International Federation of Gynecology and Obstetrics) stage IA endometrial adenocarcinoma, status post total hysterectomy and bilateral salpingo-oophorectomy, with negative lymph node biopsy, who later presented with eye swelling and pain. Imaging revealed metastatic disease to the orbit with invasion of the orbital roof. She subsequently underwent surgical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
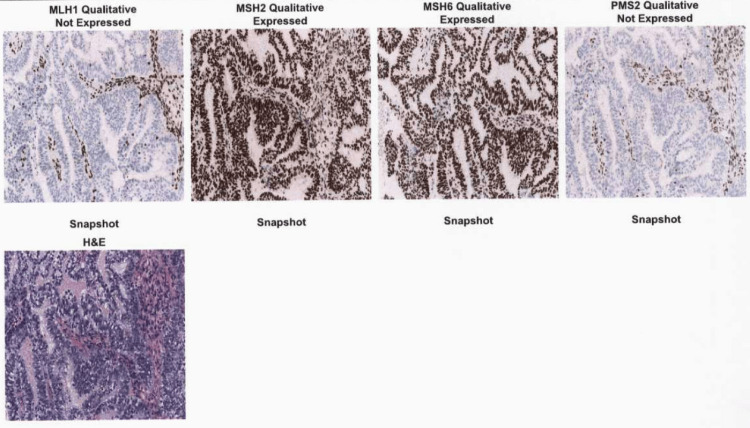 Figure 1
Figure 1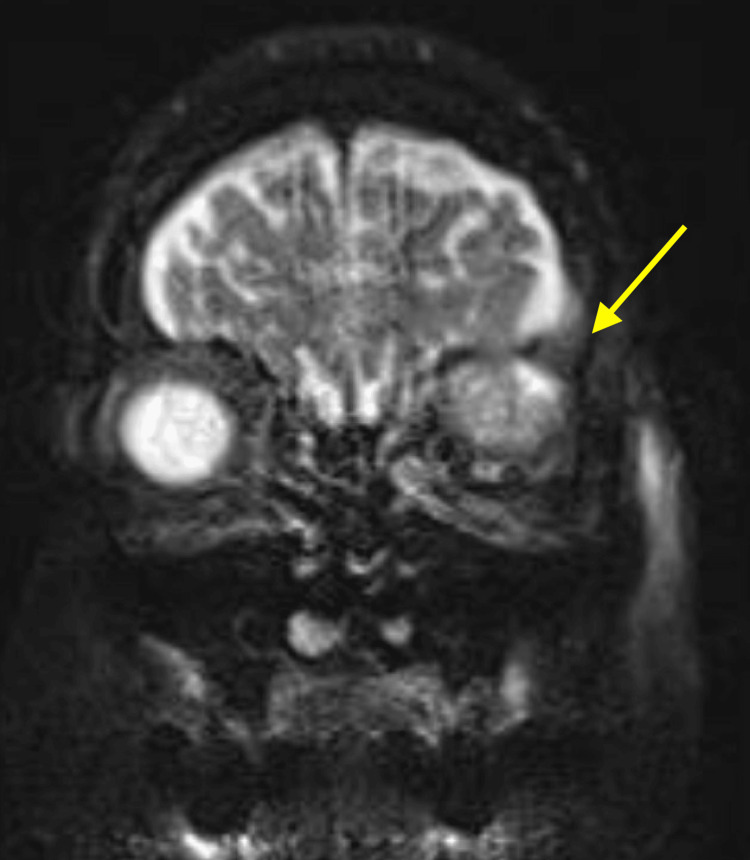 Figure 2
Figure 2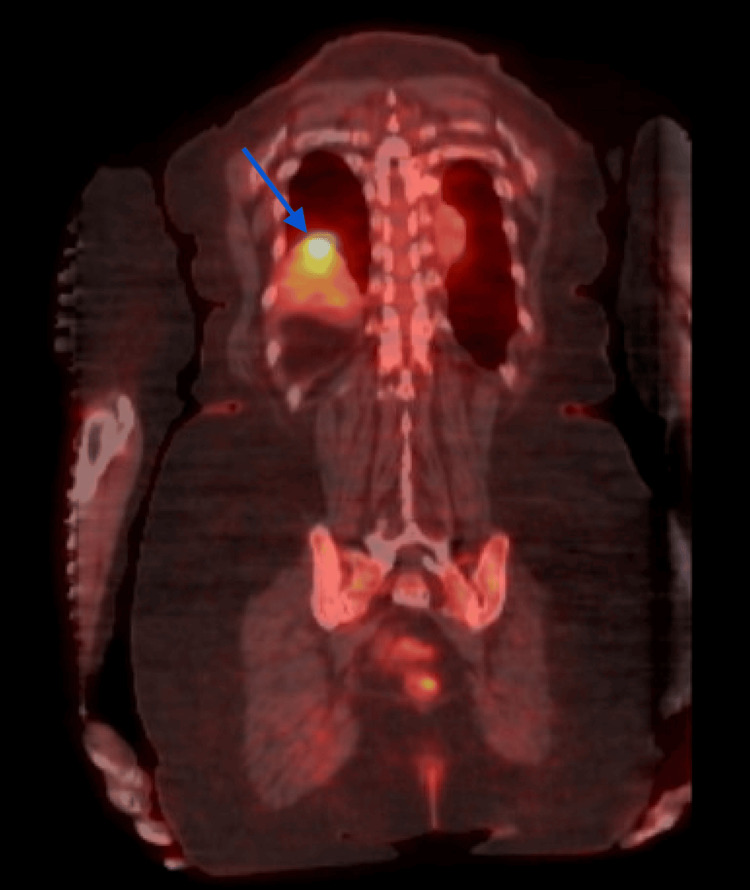 Figure 3
Figure 3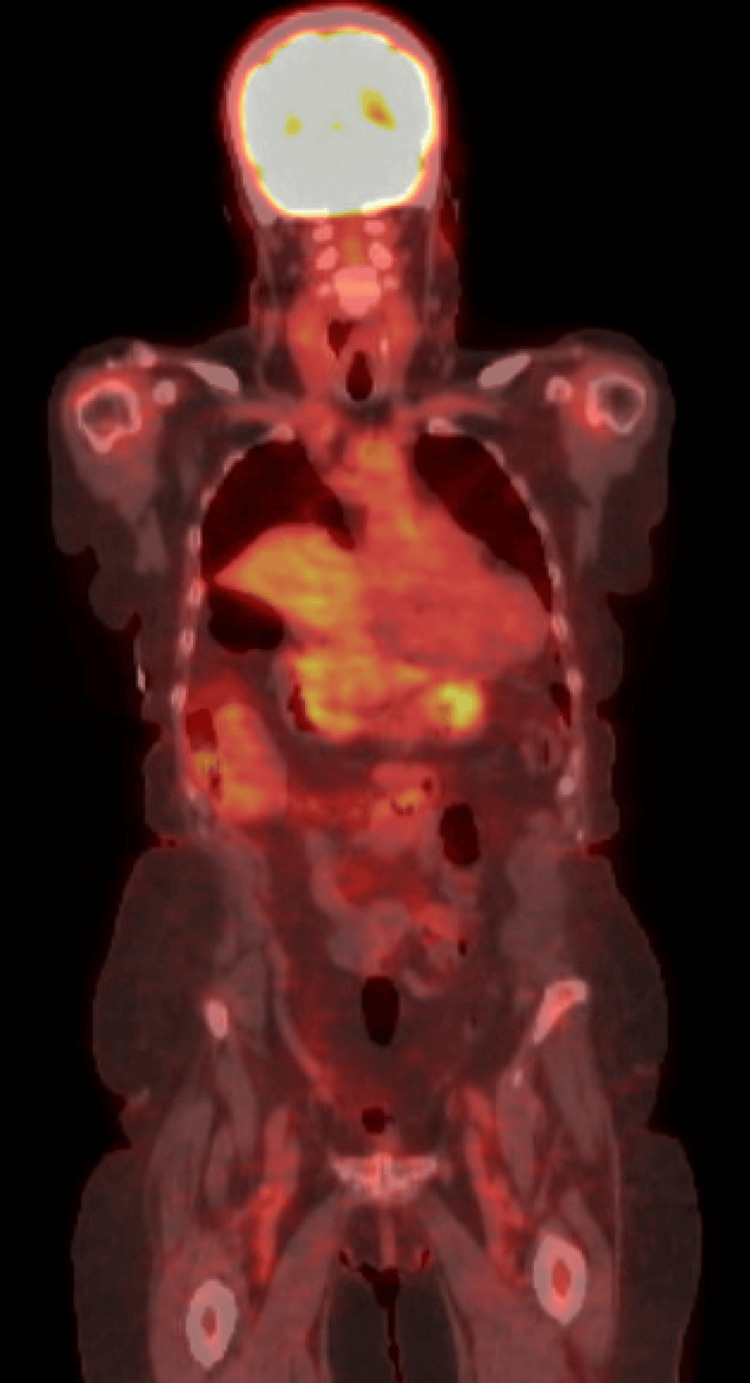 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Uterine Myomas and Treatments · Ovarian cancer diagnosis and treatment
Introduction
Endometrial cancer is the most common malignancy of the female genital tract in the United States and the fourth most common cancer among women worldwide [1,2]. Although the average age at diagnosis is 63 years, approximately 20-25% of cases occur in premenopausal women [3-6].
Historically, endometrial carcinoma has been classified into two types, Type I and Type II, based on histopathological characteristics [7-10]. However, the Cancer Genome Atlas (TCGA) has proposed a more refined molecular classification comprising four subgroups: POLE-ultramutated, microsatellite instability-high (MSI-H), copy-number high (usually associated with TP53 mutations), and copy-number low (no defining molecular alterations) [11]. This classification is increasingly used to guide prognosis and personalize treatment strategies.
The most prominent clinical features of endometrial carcinoma include abnormal uterine bleeding, intermenstrual bleeding, irregularly heavy bleeding, or any postmenopausal bleeding [6,9]. Regional extension of endometrial carcinoma may present as pelvic pain, pressure, or mass; cervical abnormalities; abdominal distension; and changes in bowel or bladder function [6,12]. Metastatic disease usually spreads lymphatically (most commonly to the retroperitoneal space), but it can rarely spread hematogenously (most commonly to the lungs). However, it is essential to note that pelvic examination and laboratory results are typically normal in patients with endometrial carcinoma [6,9,12].
The patient in this report presented with Type I endometrial cancer with microsatellite instability (MSI), indicating a defective mismatch repair system. Metastasis of endometrial adenocarcinoma is extremely rare, and the true incidence of orbital metastasis of endometrial adenocarcinoma is unknown. To date, orbital metastasis of endometrial adenocarcinoma has only been reported in case reports.
Case presentation
An 82-year-old woman (G4P4, menarche at age 15, menopause at age 52) with a history of FIGO (International Federation of Gynecology and Obstetrics) stage IA (cT1a, cN0, cM0) endometrial adenocarcinoma presented with progressive left eye pain, proptosis, and swelling approximately 19 months after her initial cancer diagnosis. Her family history was notable for ovarian cancer in her mother, thyroid cancer in her sister, and breast cancer in her daughter.
Initially, at age 80, she presented to her primary care physician with abnormal uterine bleeding. She was referred to a gynecologist and underwent hysteroscopy with dilation and curettage. Two polyps and a mass-like structure were identified and biopsied. Pathology revealed endometrioid adenocarcinoma with absent or low expression of mismatch repair (MMR) proteins MLH1 and PMS2, while MSH2 and MSH6 expression was retained (Figure 1).
Mismatch repair enzyme staining following dilation and curettage (D&C). Images viewed at 100× magnification.
Genomic testing demonstrated MLH1 promoter hypermethylation (53.5%), and microsatellite instability testing confirmed MSI-high status. The patient subsequently underwent total hysterectomy and bilateral salpingo-oophorectomy with pelvic washings. Cytological analysis and lymphadenectomy of eight right pelvic lymph nodes and seven left pelvic lymph nodes revealed no malignancy. Final pathology confirmed FIGO stage IA endometrioid adenocarcinoma (Müllerian primary) without myometrial invasion or angiolymphatic involvement of the fallopian tubes or ovaries. Given the absence of lymphatic spread, adjuvant radiation or chemotherapy was not recommended.
Nineteen months later, the patient developed left upper eyelid swelling and visual disturbances. A PET/CT was scheduled, but the patient presented to the emergency department shortly thereafter with worsening proptosis and vision loss. She was started on oral corticosteroids and empiric antibiotics, and urgent ophthalmology and neurosurgery consultations were obtained. An MRI of the orbit revealed a 4.0 × 3.2 × 3.1 cm mass in the left orbit with associated proptosis and inferior displacement of the left globe (Figure 2). The patient subsequently underwent a multidisciplinary surgical procedure, including a left orbitozygomatic craniotomy with stereotactic volumetric tumor resection, complex orbital roof and rim reconstruction, and exploratory orbitotomy with biopsy and mass resection.
Orbital MRI with and without intravenous contrast showing a large, avidly enhancing, solid and cystic mass in the left superior orbit with intracranial extension through the left orbital roof. There is direct dural involvement and mass effect on the left inferior frontal lobe.The yellow arrow denotes the left orbital mass, which displaces the globe and invades the left orbital roof.
Postoperative histopathology confirmed metastatic adenocarcinoma consistent with a Müllerian primary, with loss of MLH1 and PMS2 expression identical to the patient’s original tumor profile. She received postoperative adjuvant orbital radiation therapy. An orbitotomy with cytologic washings and biopsy was performed. Flow cytometry of the washings was negative for definitive malignancy; however, biopsy demonstrated poorly differentiated carcinoma with both acute and chronic inflammation. "Immunohistochemical staining was positive for Super K, cytokeratin 7 (CK7), progesterone receptor (PR), and estrogen receptor (ER), suggestive of metastatic Müllerian carcinoma.
A whole-body PET/CT scan revealed a 1.9 cm pulmonary nodule in the posterior aspect of the right lower lobe (Figures 3, 4). A CT-guided biopsy of the right lower lobe pulmonary nodule confirmed metastatic, poorly differentiated adenocarcinoma. Approximately 1.5 months after discharge, she began radiation therapy. She remained on oral corticosteroids to manage periorbital and intracranial edema. Pembrolizumab 200 mg every three weeks was initiated two months post-discharge, and she continues to receive Pembrolizumab every three weeks since diagnosis.
Whole-body PET/CT revealing a metastatic lung nodule.The blue arrow indicates metastatic lung nodule.
Whole-body PET/CT revealing no residual or metastatic disease in the abdomen or pelvis.
Discussion
Endometrial carcinoma is primarily a histopathologic diagnosis. In this case, the tumor was classified as FIGO stage IA, indicating superficial or no myometrial invasion. First-line management for stage IA disease typically involves surgical resection, total hysterectomy with bilateral salpingo-oophorectomy, without adjuvant therapy, as recurrence is uncommon. The risk of pelvic lymph node involvement in stage IA endometrial cancer is estimated at ≤3%, and the five-year progression-free survival rate ranges from 95% to 98% [6-11]. However, identifying the small subset of patients at higher risk for recurrence or distant metastasis remains a clinical challenge.
The role of lymph node assessment continues to be an area of active debate. While some surgeons perform systematic lymphadenectomy for staging purposes, others favor a more conservative approach, especially in low-risk disease. Sentinel lymph node (SLN) biopsy has emerged as a viable alternative, offering adequate staging with lower surgical morbidity. Advocates for limited surgery argue that the likelihood of nodal metastasis in early-stage disease is low and that lymphadenectomy provides no therapeutic benefit in the absence of nodal involvement. Additionally, omitting lymphadenectomy reduces operative time, lowers complication rates, and shortens recovery. However, this approach may lead to underdiagnosis of occult metastatic disease, delayed initiation of systemic therapy, and worse outcomes in select patients [6].
Several risk factors have been proposed to guide decision-making around lymph node dissection, including patient age, tumor grade, depth of myometrial invasion, lymphovascular space invasion (LVSI), and histologic subtype [13,14]. Biomarkers such as CA-125 have also been investigated for their potential to predict extrauterine spread [15,16]. Molecular profiling is increasingly used to stratify risk and guide treatment decisions, particularly in ambiguous or high-risk cases.
The TCGA molecular classification provides additional insight into tumor biology. In particular, MMR-D or MSI-H tumors, as seen in this patient, are associated with unique therapeutic implications. Notably, MSI-H tumors tend to respond poorly to conventional chemotherapy but demonstrate improved outcomes with immunotherapy, particularly immune checkpoint inhibitors such as pembrolizumab [17,18]. Despite promising data, standardized treatment protocols based on molecular classification have yet to be universally adopted.
This case highlights the importance of integrating molecular profiling into routine diagnostic and treatment workflows. Although the patient had low-stage, node-negative disease, her MSI-H profile and eventual hematogenous spread underscore the limitations of conventional staging and the need for personalized treatment strategies. Early identification of high-risk molecular subtypes may help guide the use of adjuvant therapies and prompt closer surveillance in patients with otherwise low-risk histology.
Conclusions
Although FIGO stage IA endometrial adenocarcinoma is generally associated with a favorable prognosis, this case illustrates how mismatch repair deficiency can significantly alter the disease trajectory. The unexpected development of distant metastasis in a patient with negative lymph node biopsies underscores the limitations of traditional staging and highlights the need for molecular profiling in early disease. A tailored approach to surveillance and treatment, particularly in patients with MSI-H tumors, may improve long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Surveillance, Epidemiology, and End Results (SEER) program. Cancer of the endometrium - cancer stat facts 7 2023 https://seer.cancer.gov/statfacts/html/corp.html
- 2Endometrial cancer Lancet Morice P Leary A Creutzberg C Abu-Rustum N Darai E 109411083872016 https://read.qxmd.com/read/269778312635452310.1016/S 0140-6736(15)00130-0 · doi ↗ · pubmed ↗
- 3Endometrial carcinoma: epidemiology, risk factors, and prevention Up To Date 7 2023 Chen LM Berek JS Waltham, MA Up To Date 2023 https://www.uptodate.com/contents/endometrial-carcinoma-epidemiology-risk-factors-and-prevention
- 4Endometrial cancer in the elderly: does age influence surgical treatments, outcomes, and prognosis?Menopause Koual M Ngo C Girault A Lécuru F Bats AS 9689762520182976219810.1097/GME.0000000000001119 · doi ↗ · pubmed ↗
- 5Endometrial cancer Stat Pearls [Internet] Mahdy H Vadakekut ES Crotzer D Treasure Island, FL Stat Pearls Publishing 2023 https://pubmed.ncbi.nlm.nih.gov/30252237/30252237 · pubmed ↗
- 6Principles and Practice of Gynecologic Oncology Chi DS Berchuck A Dizon DS Yashar CM Philadelphia, PA Lippincott Williams & Wilkins 2017 https://oncology.lwwhealthlibrary.com/book.aspx?bookid=2054
- 7Type I and II endometrial cancers: have they different risk factors?J Clin Oncol Setiawan VW Yang HP Pike MC 260726183120132373377110.1200/JCO.2012.48.2596 PMC 3699726 · doi ↗ · pubmed ↗
- 8Endometrial carcinoma: serous and clear cell histologies 7 2023 Schwartz PE 202352023 https://www.uptodate.com/contents/endometrial-carcinoma-serous-and-clear-cell-histologies