Video-assisted thoracoscopic surgery for adult benign idiopathic bronchoesophageal fistula: a report of two cases
Qihang Zhu, Jing Zhan, Xiaojing Yao, Haiping Xiao

TL;DR
Two adult cases of rare bronchoesophageal fistulas were successfully treated with video-assisted thoracoscopic surgery.
Contribution
Presents a novel surgical approach using thoracoscopic techniques for treating idiopathic bronchoesophageal fistulas.
Findings
Thoracoscopic surgery successfully resected the fistulas in two adult patients.
No postoperative complications were observed in either patient.
Videofluoroscopy was effective in identifying the abnormal tracts.
Abstract
We described two cases with idiopathic bronchoesophageal fistula presented recurrent postprandial coughing. Abnormal tracts connecting the oesophagus and bronchus were identified by videofluoroscopy. Thoracoscopic surgery was successfully performed, which involved the resection of the fistula and the interposition of a pedicle of viable parietal pleura between oesophageal and bronchial closures. Neither patient experienced symptoms of any subsequent complications. Adult bronchoesophageal fistula (BEF) is a rare condition that is typically secondary to various pathologies, including tumours, trauma and diverticula [1, 2].
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
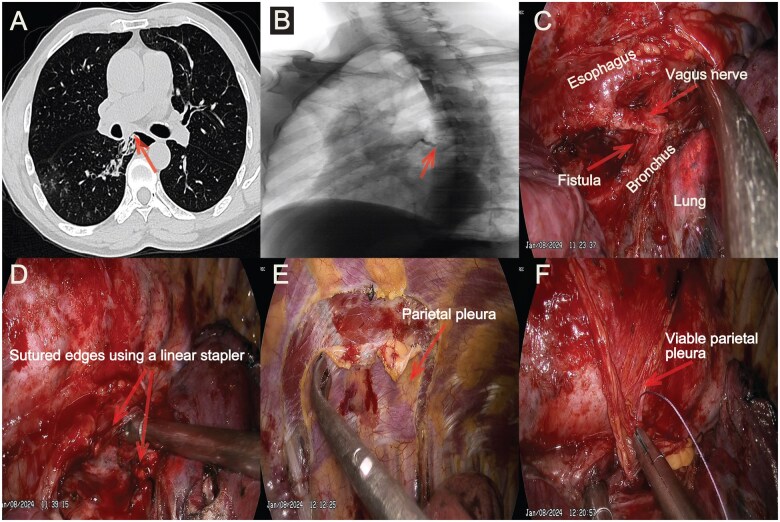 Figure 1
Figure 1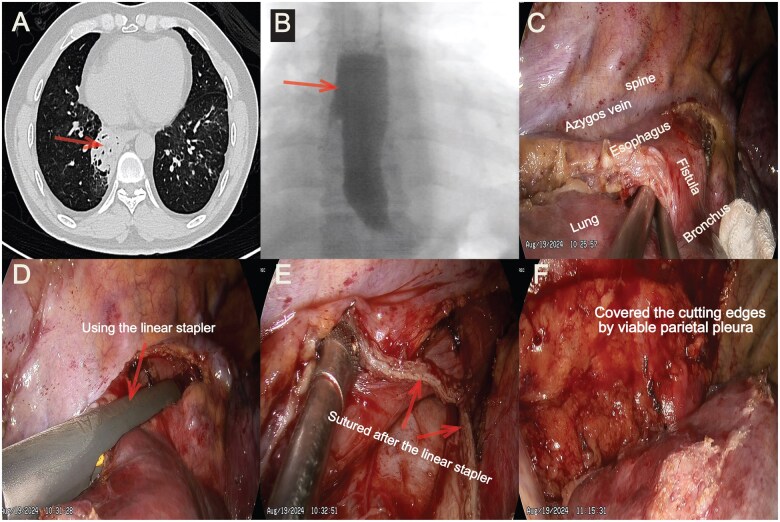 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Tracheal and airway disorders · Foreign Body Medical Cases
INTRODUCTION
Adult bronchoesophageal fistula (BEF) is a rare condition that is typically secondary to various pathologies, including tumours, trauma and diverticula [1, 2]. In certain patients diagnosed with idiopathic BEF based on symptoms and images, the exact aetiology remained undetermined despite a thorough evaluation. Traditionally, Surgical repair through thoracotomy has been the predominant surgical approach. With the advancement of thoracoscopic technology, numerous complex procedures can now be effectively performed using thoracoscopy. We reported two cases of idiopathic BEF repaired via thoracoscopic surgery.
CASES REPORT
Case 1
A 41-year-old man was admitted to our department on January 2nd, 2024 because of recurrent and worsening postprandial coughing for approximately 10 months. During this time, the patient underwent several treatments at local hospitals due to fever. However, each time was diagnosed with pneumonia based on chest X-ray. Computed tomography (CT) scan revealed chronic right lower pneumonia (Fig. 1A). Videofluoroscopy confirmed the abnormal tract connecting the oesophagus and the right middle bronchus(Fig. 1B). Bronchoscopy indicated a 0.2 cm fistula proximal to the right middle bronchus. Gastroscopy revealed a 0.3 cm fistula located 28 cm from the upper incisor. Blood tests and physical examinations did not reveal any abnormal findings.
(A) Computed tomography revealed chronic right lower pneumonia and the abnormal tract (arrow). (B) Videofluoroscopy confirmed the fistula connecting the oesophagus and the right middle bronchus (arrow). (C) Identification and exposure of the anomalous fistula. (D) After being incised and sutured using a linear stapler. (E) Plan the pleural area based on the scope. (F) Using a piece of viable parietal pleura to interpose between oesophageal and bronchial closures
The surgery was performed on January 8th, 2024. The patient was positioned in the lateral decubitus position and underwent double-lumen endotracheal intubation under general anesthesia. A skin incision of approximately 30 mm was made at the junction of the midaxillary line and the fifth intercostal space. Posterior mediastinal pleura was dissected to isolate and expose the abnormal tract connecting the oesophagus and bronchus (Fig. 1C) according to the videofluoroscopy. Then, another 10 mm incision was made at the seventh intercostal space. Linear stapler (Ethicon) was inserted to cut the tract and suture the edges on both sides (Fig. 1D). After that, absorbable suture was used to reinforce both sides. A pedicle of viable parietal pleura was dissected and interposed between oesophageal and bronchial closures to reduce the probability of recurrence (Figure 1E and F). The operation lasted 175 minutes with blood loss of about 50 mL.
Case 2
Another 52-year-old man was admitted with recurrent postprandial coughing for approximately 24 months on August 13th, 2024. CT revealed chronic right lower pneumonia, which is more consolidation than Case 1 (Figure 2A). Videofluoroscopy confirmed the fistula (Figure 2B). The invasive examinations, such as gastroscopy and bronchoscopy, were omitted. The same procedure lasted 160 minutes with blood loss of about 70 mL was performed (Figure 2C–F) on August 19th.
(A) Computed tomography revealed chronic right lower pneumonia (arrow). (B) Videofluoroscopy confirmed the abnormal tract connecting the oesophagus and the right middle bronchus (arrow). (C) Identification and exposure of the anomalous fistula. (D) Using a linear stapler to clip fistula. (E) After being incised and sutured. (F) After interpose the viable parietal pleura between oesophageal and bronchial closures
Postoperative management
Both patients were fasted for 5 days postoperatively along with gastrointestinal decompression. Parenteral nutrition, acid inhibitors and short-term antibiotics were used during the period. No short-term complications occurred. Chest drainage tubes were removed on the postoperative third day. There were no abnormalities in the videofluoroscopy on 5th postoperative day. The gastric tubes were removed and the patients resumed a liquid diet. The patients were discharged on postoperative 7th day and instructed to gradually return to a normal diet. Up to January 2025, subsequent follow-up showed good life quality. No oesophageal stenosis or recurrence of fistula was observed.
DISCUSSION
Neither patient had a history of endotracheal, oesophageal intubation, malignancy, infection or foreign bodies. The diagnosis and treatment of idiopathic BEF present considerable challenges. No standardized guidelines have been established due to the low incidence. Recurrent postprandial coughing and localized pneumonia at the same site indicate the possibility of idiopathic BEF. The most critical examination to confirm BEF is upper gastrointestinal videofluoroscopy. Gastroscopy and bronchoscopy would be beneficial, yet not essential [1].
There are very few cases concerning idiopathic BEF. Oesophageal diverticulum may be the primary potential cause of idiopathic BEF. Surgical repair is an effective approach for addressing BEF. The most widely adopted approach was thoracotomy, which often involved the interposition of vascularized muscle flaps [1, 2]. Thoracoscopic surgery has been widely used in thoracic diseases. Isolated cases have been reported and confirmed the use of thoracoscopic surgery in BEF [3, 4]. Muscle flaps are hard to obtain via thoracoscopy, whereas the pleura can be readily obtained. The viable parietal pleura, preserved by maintaining the pleural blood supply on the spinal side, serves as an appropriate tissue to be inserted between oesophageal and bronchial closures, thereby isolating tissues and reducing the risk of recurrence [5]. The whole operation process is minimally invasive and effective. Nevertheless, pre/intraoperative evaluation of the available tissue is important. Open surgery and muscle flap should be considered as alternative approaches.
There are limitations in our article. First, it is not feasible to conduct a comparative study, such as between open and thoracoscopic surgery, or between muscle and pleura, due to the limited number of cases. Second, follow-up time is limited. Long-term complications, including oesophageal stenosis, warrant continued observation. However, according to the current results, thoracoscopic surgery combined with pleural implantation demonstrates advantages and is worthy of further application and promotion in BEF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sun Y , Hao S, Yang Y et al Surgical management of acquired tracheo/bronchoesophageal fistula associated with esophageal diverticulum. J Thorac Dis 2017;9:3684–92.29268375 10.21037/jtd.2017.09.81PMC 5723829 · doi ↗ · pubmed ↗
- 2Zhang X , Jiao H, Liu X. Bronchoesophageal fistula secondary to esophageal diverticulum in an adult: a case report and literature review. J Int Med Res 2021;49:300060521992234.33596687 10.1177/0300060521992234 PMC 7897816 · doi ↗ · pubmed ↗
- 3Braghetto I , Cardemil G, Schwartz E et al Videothoracoscopic management of middle esophageal diverticulum with secondary bronchoesophageal fistula: report of a case. Surg Today 2008;38:1124–8.19039640 10.1007/s 00595-008-3797-4 · doi ↗ · pubmed ↗
- 4Kang DK , Kang MK, Heo W, Hwang YH. Successful repair of bronchoesophageal fistula through uniportal video-assisted thoracoscopic surgery. J Investig Med High Impact Case Rep 2021;9:23247096211028385.10.1177/23247096211028385 PMC 823676934176303 · doi ↗ · pubmed ↗
- 5Zhang BS , Zhou NK, Yu CH. Congenital bronchoesophageal fistula in adults. World J Gastroenterol 2011;17:1358–61.21455337 10.3748/wjg.v 17.i 10.1358 PMC 3068273 · doi ↗ · pubmed ↗