Double Trouble: A Case Report of Hydralazine-Induced Vasculitis and Lupus
Malika Ibrahim, Thanda Aung, Sravani Penumarty

TL;DR
A 77-year-old woman developed severe drug-induced lupus and vasculitis after taking hydralazine, affecting multiple organs and requiring urgent medical attention.
Contribution
This case report highlights the rare but severe multi-organ complications of hydralazine-induced autoimmune syndrome.
Findings
The patient experienced hypoxic respiratory failure due to diffuse alveolar hemorrhage.
Acute kidney injury with crescentic glomerulonephritis and pancytopenia were observed.
Serologic tests confirmed a drug-induced autoimmune syndrome with positive ANA, dsDNA, anti-histone, and P-ANCA.
Abstract
We present a rare case of hydralazine-induced antineutrophil cytoplasmic antibody (ANCA) vasculitis and lupus, characterized by the simultaneous and severe involvement of multiple organ systems. Following outpatient hydralazine dose escalation, a 77-year-old woman developed hypoxic respiratory failure secondary to diffuse alveolar hemorrhage, acute kidney injury with crescentic glomerulonephritis, and pancytopenia. Serologic testing revealed positive antinuclear antibody (ANA), dsDNA, anti-histone antibody, and P-ANCA, supporting the diagnosis of drug-induced autoimmune syndrome. This case highlights the risk for severe multi-organ dysfunction in drug-induced lupus and vasculitis, emphasizing the need for vigilance in recognizing such complications.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
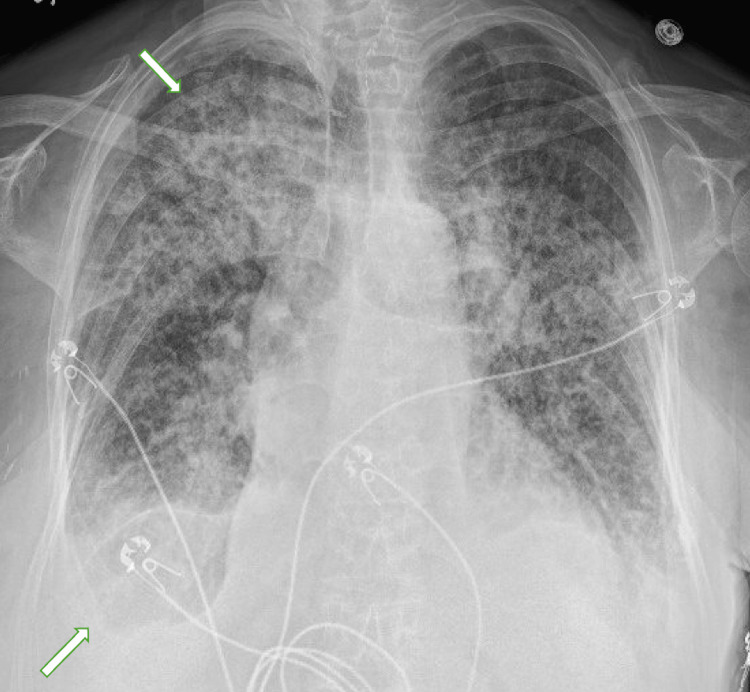 Figure 1
Figure 1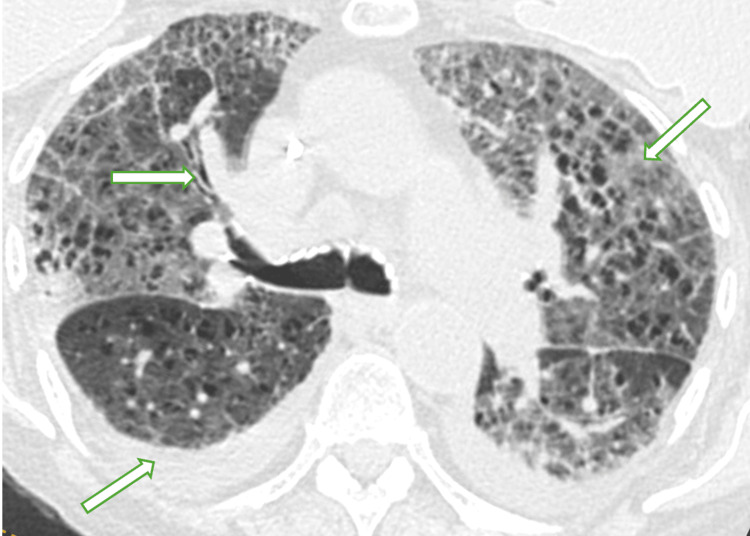 Figure 2
Figure 2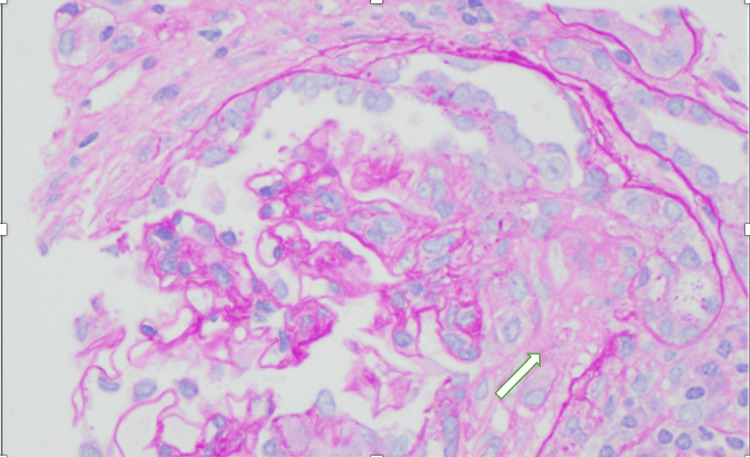 Figure 3
Figure 3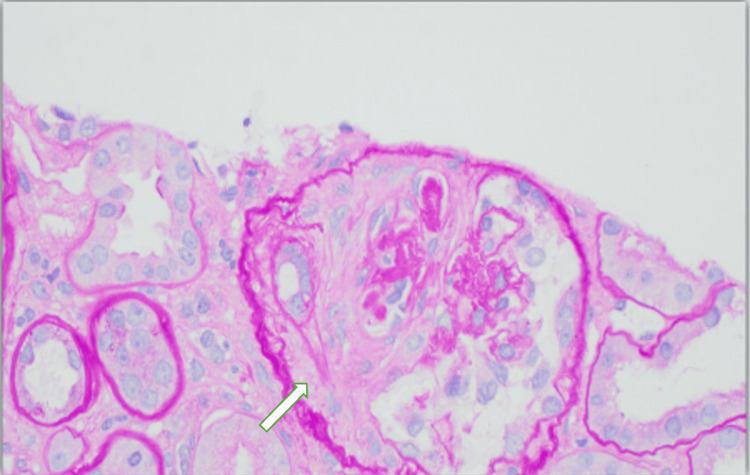 Figure 4
Figure 4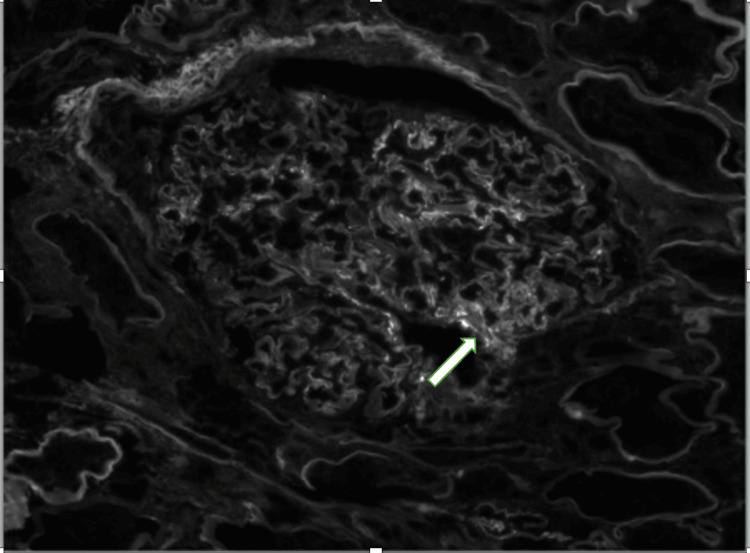 Figure 5
Figure 5 Figure 6
Figure 6| Laboratory Test | Patient Value | Reference Range & Units |
| White Blood Cell Count | 1.78 x10E3/uL | 4.16-9.95 x10E3/uL |
| Hemoglobin | 6.8 g/dl | 11.6-15.2 g/dl |
| Hematocrit | 22.1 % | 34.9-45.2 % |
| Mean Corpuscular Volume | 90.2 fL | 79.3-98.6 fL |
| Mean Corpuscular Hemoglobin | 29.4 pg | 26.4-33.4 pg |
| Platelets | 122 x10E3/uL | 143-398 x10E3/uL |
| Absolute Reticulocyte Count | 0.03 x10E3/uL | 0.02-0.26 x10E3/uL |
| Red Blood Cell Morphology | Normal | Normal |
| Schistocytes | Negative | Negative |
| Haptoglobin | 152 mg/dl | 21-210 mg/dl |
| Lactate Dehydrogenase | 286 U/L | 125-256 U/L |
| Urea | 51 mg/dl | 7-22 mg/dl |
| Creatinine | 5.3 mg/dl | 0.6-1.3 mg/dl |
| eGFR | 9 mL/min/1.73m2 | >89 mL/min/1.73m2 |
| Immunoglobulin G | 1,181 mg/dl | 70-1600 mg/dl |
| Immunoglobulin A | 145 mg/dl | 76-426 mg/dl |
| Immunoglobulin M | 404 mg/dl | 40-230 mg/dl |
| Complement 3 | 48 mg/dl | 86-175 mg/dl |
| Complement 4 | 15 mg/dl | 10-40 mg/dl |
| C-reactive Protein (CRP) | 12.9 mg/dl | <0.8 mg/dl |
| Erythrocyte Sedimentation Rate (ESR) | 39 mm/hr | <=25 mm/hr |
| Thyroid-Stimulating hormone (TSH) | 11.9 mcIU/mL | 0.03-4 mcIU/mL |
| Streptolysin O Antibody (ASO) | <55 IU/mL | <=330 IU/mL |
| Antinuclear Antibody | <1:40 titer | <1:40 titer |
| Double-Stranded DNA Antibody EIA | 986 IU/mL | <=200 IU/mL |
| c-ANCA | 1:40 titer | < 1:20 titer |
| P-ANCA | >-1:12850 titer | < 1:20 titer |
| Myeloperoxidase Antibody | 128.4 CU | <20 CU |
| Proteinase-3 Antibody | 69.9 CU | <20 CU |
| Histone Ab | 5.3 Units | 0.0-0.9 Units |
| Centrome B Antibody | <1.0 AI | <1.0 AI (Antibody Index) |
| PM/Scl 100 Antibody IgG | Negative | Negative |
| SM Antibody | <20 Units | <20 Units |
| RNP Antibody | <20 Units | <20 Units |
| SSA Antibody | <20 Units | <20 Units |
| SSB Antibody | <20 Units | <20 Units |
| SSA-52 Antibody (Ro52) | 1 AU/mL | >=29 AU/mL |
| SSA-60 Antibody (Ro60) | 0 AU/mL | >=29 AU/mL |
| Scl-70 Antibody | 0 AU/mL | >=29 AU/mL |
| EJ Antibody | Negative | Negative |
| Ku Antibody | Negative | Negative |
| MDA5 Antibody | Negative | Negative |
| Mi-2 Antibody | Negative | Negative |
| NXP2 Antibody | Negative | Negative |
| OJ Antibody | Negative | Negative |
| PL-7 Antibody | Negative | Negative |
| PL-12 Antibody | Negative | Negative |
| P155/140 Antibody | Negative | Negative |
| SAE1 Antibody | Negative | Negative |
| SRP Antibody | Negative | Negative |
| TIF-1 Gamma Antibody | Negative | Negative |
| Jo-1 Antibody | Negative | Negative |
| HMGCR Antibody | <3 Units | 0-19 Units |
| Thyroid Peroxidase Antibody | 14 IU/mL | <=20 IU/mL |
| Thyroglobulin Antibody | <0.9 IU/mL | <=4 IU/mL |
| Cardiolipin Immunoglobulin A | <20 CU | <=20 CU |
| Cardiolipin Immunoglobulin G | <20 CU | <=20 CU |
| Cardiolipin Immunoglobulin M | 167 CU | <=20 CU |
| Cryocrit | Negative | Negative |
| Urine Analysis | ||
| Protein | 2+ | Negative |
| Blood | 3+ | Negative |
| Red Blood Cell per HPF | >210 cells/HPF | 0-2 cells/HPF |
| White Blood Cell per HPF | 4 cells/HPF | 0-4 cells/HPF |
| Hyaline Casts | >20/LPF | 0-2/LPF |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Urticaria and Related Conditions · Coagulation, Bradykinin, Polyphosphates, and Angioedema
Introduction
Antineutrophil cytoplasmic antibody (ANCA) vasculitis is a small vessel disease in which ANCAs, typically against myeloperoxidase or proteinase 3, activate neutrophils and cause rapidly progressive glomerulonephritis, pulmonary hemorrhage, and systemic inflammation [1]. Drug-induced lupus (DIL), often associated with hydralazine, is a reversible autoimmune syndrome marked by anti-nuclear and anti-histone antibodies and immune-complex deposition, producing lupus-like manifestations that resolve upon drug withdrawal [2]. Hydralazine-induced ANCA vasculitis and lupus represent a potentially life-threatening adverse drug reaction that requires prompt recognition and management. With an incidence of 5-10% in patients receiving hydralazine, particularly among slow acetylators, women, and those on higher doses or prolonged therapy [3,4], this condition involves drug-induced DNA demethylation leading to autoantibody formation against neutrophil components [5]. Unlike classic DIL, which typically presents with milder constitutional symptoms and arthralgias, hydralazine-induced ANCA vasculitis often manifests with severe multi-organ involvement including glomerulonephritis, alveolar hemorrhage, and systemic vasculitis [6,7]. Diagnosis relies on establishing a temporal relationship between drug exposure and symptom onset, positive serologic markers (ANA, anti-histone antibodies, ANCA), and exclusion of alternative etiologies [8]. This report highlights the case of a 77-year-old woman who developed acute kidney injury with crescentic glomerulonephritis, pancytopenia, and diffuse alveolar hemorrhage following hydralazine dose escalation in the outpatient setting during the months preceding hospitalization, emphasizing the need for heightened clinical vigilance for this severe complication in patients receiving hydralazine therapy.
Case presentation
A 77-year-old woman with a significant medical history of thyroid cancer status post-thyroidectomy and breast cancer status post-mastectomy presented with acute renal failure and pancytopenia. A few weeks before her admission, she was experiencing severe fatigue, chills, poor appetite, and intermittent diarrhea. Her thyroid replacement therapy was uptitrated on an outpatient basis to alleviate some of her symptoms, but the adjustment proved unsuccessful.
On admission, she was afebrile with a blood pressure of 165/85 mmHg, a respiratory rate of 18, and was saturating 99% on room air. On examination, she had 4+ bilateral lower extremity edema extending to the knees. She had increased work of breathing but a normal cardiac exam.
She had a long history of severe hypertension, managed with several antihypertensive medications, including bumetanide 1 mg daily, hydralazine 100 mg three times daily, and valsartan 160 mg daily. Upon evaluation, the patient was found to have an acute kidney injury. Her urinalysis showed proteinuria and hematuria in the sub-nephrotic range. Her admission labs also revealed pancytopenia and elevation in both her sedimentation rate and C-reactive protein (CRP).
In addition to her renal issues, she developed progressive anemia that remained unstable despite blood transfusions. On hospital day 3, she developed hypoxia requiring supplemental oxygen via a high-flow nasal cannula at 60L/min and 60% FiO2. A chest X-ray, shown in Figure 1, revealed diffuse airspace opacities, suggesting pulmonary edema or alveolar hemorrhage. The following day, her condition further deteriorated with the onset of frank hemoptysis and an increased need for oxygen, leading to her transfer to the intensive care unit (ICU). Due to her unstable vitals, bronchoscopy was deferred. A computed tomography (CT) scan of her chest, shown in Figure 2 completed five days into her ICU stay, displayed ground glass changes and pleural effusions with possible overlying atelectasis and or pneumonia.
Chest X-ray showing a bilateral upper lobe greater than lower lobe airspace infiltrates and bilateral small pleural effusions
Follow-up CT chest without contrast showing interlobular septal thickening with patchy ground glass in the upper lobes, with a small right more than left pleural effusions with overlying atelectasis/pneumoniaCT, Computed Tomography
A series of autoimmune tests were ordered, detailed in Table 1, revealing low C3, low-normal C4, positive high-titer dsDNA and positive P-ANCA with titer elevation, raising concern for lupus nephritis versus ANCA-induced vasculitis. The differential diagnosis also included thrombotic thrombocytopenic purpura (TTP), hemolytic uremic syndrome (HUS), membranoproliferative glomerulonephritis, multiple myeloma, and cryoglobulinemia.
Further inquiry revealed that the patient had recently increased her hydralazine dosage to 100 mg three times daily approximately 1.5 months before this admission. This raised suspicion for hydralazine-induced lupus or a related vasculitis, further supported by a positive anti-histone antibody.
On day 3 of hospitalization, she was treated with tranexamic acid for hemoptysis, high-dose steroids, a five-day course of plasmapheresis (PLEX), and a rituximab infusion as part of her ANCA-associated vasculitis vs DIL management. A hemodialysis catheter was inserted, and she underwent dialysis while being monitored for renal recovery. With the above treatment, the patient started showing clinical improvement.
A kidney biopsy, shown in Figures 3-6 with the corresponding pathology slides, was performed on hospital day 15 after the patient had stabilized. The findings were consistent with predominantly chronic crescentic glomerulonephritis. The biopsy revealed low-grade IgG/C3 deposits and mild tubulointerstitial scarring (25% involvement). Of the 18 glomeruli sampled, seven showed crescents (six fibrous, one fibrocellular). The low-grade deposits were mostly in mesangial regions but did not exhibit the characteristic "full house" pattern seen in lupus nephritis. These findings were compatible with a pauci-immune (ANCA-associated) process, which could be related to the noted hydralazine use.
Kidney biopsy slide under light microscopy showing inflammatory cells and presence of fibrocellular crescents
Kidney biopsy under light microscopy showing fibrous crescents
Kidney biopsy using immunofluorescence staining and microscopy showing segmental IgG deposition in the mesangial region
Kidney biopsy using immunofluorescence staining showing trace C3 deposition
At the time of discharge, she was weaned off oxygen and scheduled for outpatient follow-up, including interval repeat imaging, pulmonary function tests, ongoing monitoring of renal improvement on dialysis, and rheumatology follow-up for immunosuppression management including steroid taper and rituximab infusions.
Discussion
This case illustrates the diagnostic and therapeutic challenges encountered in patients with multisystem involvement suggestive of an autoimmune process, particularly in the context of long-term medication use. The patient’s presentation, with acute kidney injury, pancytopenia, pulmonary hemorrhage, and elevated systemic inflammatory markers, prompted a broad differential that included lupus nephritis, ANCA-associated vasculitis, and other microangiopathic processes such as TTP or HUS.
A critical aspect of this case was the history of hydralazine use, especially the recent up-titration to 100 mg three times daily. Hydralazine is a well-recognized trigger for DIL as well as for ANCA-associated vasculitis [9]. Factors leading to this spectrum of hydralazine-induced autoimmunity are not fully understood, but the current hypothesis includes that hydralazine alters neutrophil and lymphocyte function to promote the exposure of sequestered antigens and decrease central tolerance. This, in turn, leads to ANCAs and/or anti-nuclear antibodies (ANA), which may lead to overt systemic autoimmunity [10]. Notably, hydralazine-associated organ damage can be extensive, and in cases of hydralazine-induced ANCA vasculitis, the kidneys are frequently affected, manifesting as rapidly progressive glomerulonephritis with crescent formation, as seen in our patient. Such renal involvement can lead to irreversible kidney injury if not promptly identified and managed [6]. Additionally, though rare, pulmonary involvement evidenced by diffuse alveolar hemorrhage and interstitial changes on imaging in our case can occur leading to life-threatening respiratory compromise [11,12]. Lionaki et al. described an increased risk for developing hydralazine-induced ANCA-associated vasculitis with a longer duration and higher doses of hydralazine therapy especially in slow acetylators, female patients, and patients with a history of thyroid disease, a phenotype relevant to our case who suffered from hypothyroidism with futile up-titration of thyroid replacement therapy in the period leading to hospitalization [13].
Previous case reports reveal that most patients with drug-induced ANCA-associated vasculitis have MPO-ANCA, frequently in very high titers, as found in our patient [5]. However, the complete serologic profile of this patient further confounded the diagnostic picture. Although hydralazine-induced lupus is classically characterized by positive anti-histone antibodies with an absence of anti-dsDNA antibodies [14], our patient demonstrated elevated dsDNA titers. The coexistence of anti-dsDNA, typically seen in idiopathic SLE, with high-titer anti-histone antibodies, low C3 levels, pancytopenia, and constitutional symptoms complicates the clinical assessment, suggesting an overlap syndrome and underscoring the continuum between DIL and ANCA-associated vasculitis [6]. In experimental evidence, data demonstrated that patients treated with hydralazine recognize a broader array of auto-antigenic epitopes, which may explain the spectrum of antibody serology in our case [15].
Although DIL remained a consideration based on serology, the kidney biopsy findings of predominantly chronic crescents, low-grade IgG and C3 immune deposits, and the absence of a “full house” immunofluorescence pattern strongly favored a pauci immune process over classic lupus nephritis. These histopathologic features are consistent with ANCA-associated vasculitis and, in the context of hydralazine exposure, support a diagnosis of hydralazine-induced ANCA vasculitis.
Management of this patient was complex and necessitated rapid intervention due to the progression of both renal and pulmonary involvement, and prompt discontinuation of the offending agent, hydralazine. The initiation of pulse-dose steroids, plasmapheresis, and rituximab reflects the accepted aggressive approach aimed at controlling the autoimmune process and minimizing irreversible organ damage in such cases [16]. This case underscores the importance of recognizing the full spectrum of hydralazine-induced organ injury. Early recognition of both hydralazine-associated ANCA vasculitis and DIL is crucial, as the extent of organ damage, ranging from severe renal impairment to life-threatening pulmonary hemorrhage, demands prompt and targeted therapy to improve patient outcomes.
Conclusions
This case illustrates the potentially life-threatening nature of hydralazine-induced ANCA vasculitis and lupus, characterized by multi-organ involvement including pulmonary hemorrhage, crescentic glomerulonephritis, and pancytopenia. The temporal relationship between hydralazine dose escalation and symptom onset, coupled with positive serologic markers, underscores the importance of medication review in patients presenting with unexplained multi-system disease. Clinicians should maintain a high index of suspicion for drug-induced autoimmunity, particularly in elderly patients and those with risk factors such as higher doses or prolonged therapy. Early recognition, prompt discontinuation of the offending agent, and appropriate immunosuppressive therapy are crucial for preventing irreversible organ damage.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides Arthritis Rheum Jennette JC Falk RJ Bacon PA 1116520132304517010.1002/art.37715 · doi ↗ · pubmed ↗
- 2Drug-induced lupus erythematosus: incidence, management and prevention Drug Saf Chang C Gershwin ME 3573743420112151336010.2165/11588500-000000000-00000 · doi ↗ · pubmed ↗
- 3The lupus syndrome induced by hydralazine: a common complication with low dose treatment Br Med J (Clin Res Ed) Cameron HA Ramsay LE 410412289198410.1136/bmj.289.6442.410PMC 14424476432120 · doi ↗ · pubmed ↗
- 4Acetylator phenotype and lupus erythematosus Clin Pharmacokinet Uetrecht JP Woosley RL 11813461981701165610.2165/00003088-198106020-00003 · doi ↗ · pubmed ↗
- 5Drug-associated antineutrophil cytoplasmic antibody-positive vasculitis: prevalence among patients with high titers of antimyeloperoxidase antibodies Arthritis Rheum Choi HK Merkel PA Walker AM Niles JL 4054134320001069388210.1002/1529-0131(200002)43:2<405::AID-ANR 22>3.0.CO;2-5 · doi ↗ · pubmed ↗
- 6Hydralazine-induced autoimmune disease: comparison to idiopathic lupus and ANCA-positive vasculitis Mod Rheumatol Yokogawa N Vivino FB 3383471920091942477210.1007/s 10165-009-0168-y · doi ↗ · pubmed ↗
- 7Trojan horses: drug culprits associated with antineutrophil cytoplasmic autoantibody (ANCA) vasculitis Curr Opin Rheumatol Pendergraft WF 3rd Niles JL 42492620142427608610.1097/BOR.0000000000000014 · doi ↗ · pubmed ↗
- 8Updates on the treatment of lupus nephritis J Am Soc Nephrol Bomback AS Appel GB 202820352120102105174310.1681/ASN.2010050472 · doi ↗ · pubmed ↗