Negative health effects of dental X-rays: A systematic review
Laila Wiklander, Andreas Cederlund, Nils Kadesjö, Peggy Näsman, Sofia Tranaeus, Aron Naimi-Akbar, Mohmed Isaqali Karobari, Mohmed Isaqali Karobari, Mohmed Isaqali Karobari

TL;DR
This review finds that current evidence is insufficient to determine if dental X-rays in children and teens cause health issues.
Contribution
The study systematically reviews existing literature to assess the health risks of dental X-rays in young populations.
Findings
None of the selected studies met quality standards due to high bias risk.
There is a lack of reliable evidence on the negative health effects of dental X-rays in children and adolescents.
The review highlights the need for more accurate and updated research on this topic.
Abstract
This study evaluates whether exposure to dental X-ray examinations in childhood and adolescence results in negative health effects. This systematic review includes both primary studies and systematic reviews available in Medline, Embase, and Web of Science databases. Six reviewers read the full text of the selected studies. The literature search resulted in 10,949 publications. After title and abstract screening, 55 publications were selected for full text reading, resulting in a total of 18 reports, 7 systematic reviews, and 11 primary studies for quality assessment. None of the selected studies passed the quality assessment due to high or very high risk of bias. There is a gap of knowledge regarding negative effects of dental X-rays and a need for more accurate and updated studies.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
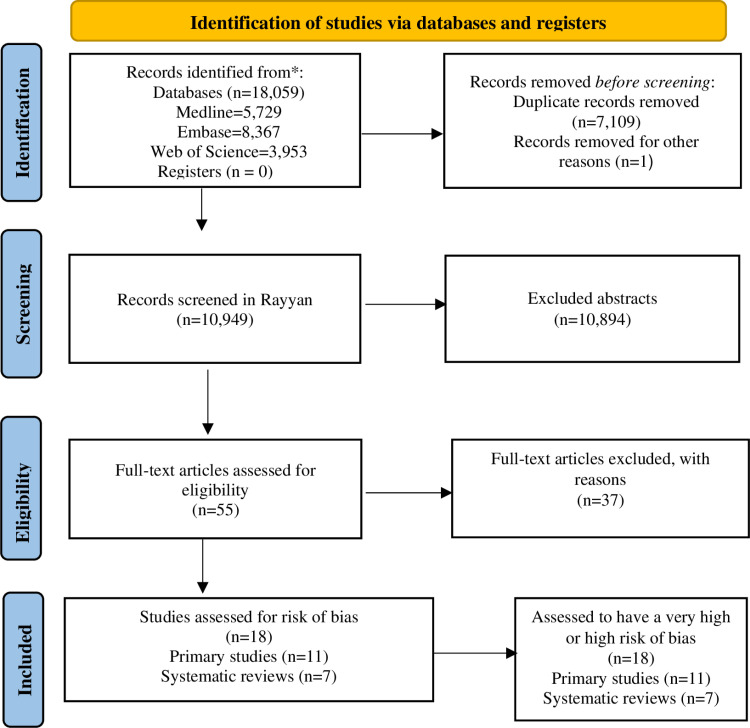 Fig 1
Fig 1- —Folktandvården stockholms län AB
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiation Dose and Imaging · Advanced X-ray and CT Imaging · Radiology practices and education
Introduction
Dental X-rays are a common procedure in dental care as a part of a clinical examination. Intraoral and extraoral examinations can be used to diagnose cavities, periodontal disease, and pathological problems or to evaluate disturbance in tooth development and growth. Between 2008 and 2022, annual dental radiology examinations increased from approximately 480 million to 1.1 billion [1]. This increase highlights the importance of studying the effects of radiation in dentistry. Intraoral radiographs – i.e., bitewing projections – are the most common radiographs for caries detection [2]. Panoramic and lateral cephalometric radiographs are extraoral x-ray examinations, which are often needed for orthodontic evaluation. Cone Beam Computed Tomography (CBCT) is another type of extraoral radiographic examination in dentistry which over the last 20 years has become more common, as an alternative and complement to the traditional examinations.
Optimizing and justifying every X-ray examination as well as keeping up with developments in radiology is important for ensuring patient safety. The technical advances in the last 20 years that should have lowered radiation exposure (i.e., dose) from intraoral examinations have not occurred due to increased accessibility of X-ray equipment and the use of multiple retakes [3,4]. Studies have shown that frequent bitewing examinations in childhood and adolescence are not necessarily connected to the risk of caries or based on individual indications, but rather as being part of a screening process where the dentists presume the risk of caries is higher than the risks associated with ionizing radiation [5,6].
Ionizing radiation can cause cancer and have negative effects on the eyes and thyroid gland. The radiation dose from dental X-ray examinations is low compared to most medical X-ray examinations. At these low dose levels, there is no clear epidemiological evidence for radiation-induced cancer from single X-ray examinations. However, very low cancer risks are still assumed but indistinguishable from the baseline cancer rate due to insufficient statistical power [7]. This implies the risk of radiation-induced cancer can accumulate with multiple examinations of the same individual or as a collective risk to the population. This understanding is especially important for dental X-rays as they are more frequently used than medical X-rays. The patients exposed to dental X-rays are also generally younger (usually children) and healthier than patients exposed to medical X-rays. Children are more sensitive to ionizing radiation, further increasing the need to understand the risks from dental X-rays.
Some studies conclude that there is a risk for meningioma [8,9] after dental X-rays. These results are based on historical data and on the participants’ ability to remember dental X-ray examinations from their childhood. Some studies use results from before 1945 when the doses were much higher than today. Systematic reviews have been done with mixed results, although they are mostly based on the same primary studies. This further shows the gap in knowledge and the need for a different approach where the qualities of the studies are assessed using well-established protocols before making any conclusions.
It is important to have reliable information regarding these risks. The risk with ionizing radiation concern patients. Studies showing potential risks of harmful medical impact may cause disproportionate negative media attention and public trust can be hard to regain.
If the use of X-rays in dentistry entails risks for the development of cancer, it is important that these risks are well described as they may affect patients’ willingness to undergo X-ray examinations.
Hence, this study addresses the following research question: What are the effect sizes of negative health effects of dental X-rays among children and adolescents?
Materials and methods
Objectives
This study investigates the evidence for health risks associated with dental X-rays. The protocol was registered at PROSPERO International prospective register of systematic reviews (CRD42022369405). PRISMA checklist is presented in in S1 File.
Eligibility criteria for studies
Eligibility criteria for inclusion of the studies were as follows: a predefined study population with age and sex registered. Population Exposure Control Outcome (PECO) as well as inclusion and exclusion criteria for eligible studies are summarized in Table 1.
Table 1: PECO and inclusion/exclusion criteria.
Literature search
A search was performed in the following databases: Medline (Ovid), Embase (embase.com), and Web of Science (Clarivate). The final search was conducted the 15^th^ of August 2024.
Search strategies
The search strategy was developed in Medline (Ovid) in collaboration with librarians at the Karolinska Institutet University Library. For each search concept, Medical Subject Headings (MeSH terms) and free text terms were identified. The search was then translated into the other databases with assistance from the Polyglot Search Translator [10]. The search was limited to studies written in English and databases were searched from inception. These strategies were reviewed by another librarian before execution. De-duplication was done using the method described by Bramer et al. [11]. An extra step was added to compare DOIs. A snowball search was applied to check references and citations of eligible studies from the database searches using EndNoteX9. The full search strategies for all databases are listed in Table 2.
Table 2: Search strategy.
Study selection
The Rayyan software program (Qatar Computing Research Institute; Data Analytics) was used to manage the references and 10,949 records were imported and in a first step duplicates were removed. The retrieved list of publications was subject to a crude exclusion of irrelevant publications based on title. In case of uncertainty, the publication remained included until the next selection step for the assessment of the abstracts. The abstracts were read by six reviewers independently divided into two groups: Aron Naimi-Akbar (ANA), Laila Wiklander (LW) and Nils Kadesjö (NK), in one group. Andreas Cederlund (AC), Sofia Tranaeus (ST), Peggy Näsman (PN), and LW in the other. 10,894 records were excluded after reading the abstracts because they did not meet the inclusion criteria presented in Table 1. Finally, 55 studies were selected for full text reading by all six reviewers (AC, ANA, LW, NK, PN, ST). Any disagreement during the screening process, from abstract to full text, was solved by discussion in the project group. Duplicates, non-relevant studies such as case reports, studies with wrong exposure, book chapters, letters to editor, comments, and studies with nonrelevant outcomes were excluded. All articles excluded (n = 37) are listed in Table 3 with the reason(s) for exclusion. The included articles are divided into systematic reviews (n = 7) and primary studies (n = 11).
Table 3: Reasons for exclusion (full text level).
Assessment of risk of bias
Systematic reviews.
The risk of bias in the included systematic reviews were assessed using ROBIS [12].
Primary studies.
The risk of bias of the included primary studies was assessed using ROBINS-E (version 2023, June 20) [13]. Before the assessment, the group prepared a list of very important and important confounding factors. In the group of very important confounding factors that can influence the outcome, ionizing medical radiation, radiotherapy, age, and gender were set. Additional important confounding factors were socioeconomic factors, lifestyle habits, genetics, radiation sensitivity, syndrome, disease, profession, environmental toxins, and natural background radiation.
Data extraction
Systematic reviews.
No systematic review was eligible for data extraction after assessment of risk of bias by the research group.
Primary studies.
Data were extracted by AC, ANA, LW, PN and ST from the primary studies regarding population (number of patients/study subjects), study period, (length of follow-up), age, sex, and type of outcome. In October 2023 the extraction was finalized by ANA, ST and LW.
Certainty of evidence
The certainty of the evidence in the studies was evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) in four steps of evidence grading: high, moderate, low, and very low [14].
Results
Literature search and study selection
After the updated literature search in August 2024 a result of 10,949 publications were retrieved. In Table 2 the search strategy is presented for each database. The flow chart of the screening process for the studies is shown in Fig 1.
PRISMA flow chart [15].
A total of 55 potential publications were gathered for full text reading after the screening of titles and abstracts by the group. Any publications that were not relevant for the aim of this systematic review were excluded. All the excluded publications are presented in Table 3 with reasons for exclusion.
Assessment of risk of bias and data extraction
Systematic reviews.
All systematic reviews were assessed to have high risk of bias in several of the four domains (Table 4). However, in one of the reviews, Memon et al [53], relevant information was presented, which is set in relation to the present systematic review in the Discussion section.
Table 4: Assessment of risk of bias in the systematic reviews.
Primary studies.
The assessment of risk of bias resulted in eleven primary studies. The evaluation of domain 1(A) concluded that only four of the studies passed. In domain 1(A), the focus is on the confounding factors. As the rest had a very high risk of bias or high risk of bias, they were excluded (Table 5). In Table 6 all the eleven included studies are presented with type of study population characteristics, type of dental x-ray examination, exposure, outcome, statistical analyses, and comments.
Table 5: Assessment of risk of bias in the primary studies.
Table 6: Characteristics of included primary studies.
Meta-analysis
Due to the low quality of evidence for the review question, it was not possible to extract data for a meta-analysis or a Synthesis Without Meta-analysis (SWiM). Additionally, the heterogeneity between the included studies was extremely high.
Summary of findings
Table 7 summarizes the findings for effects of exposures on meningioma, breast cancer, thyroid cancer, and malignant tumors of the parotid gland. There is very low certainty of evidence for negative health outcomes due to dental x-rays.
Table 7: Summary of findings for effects of exposure on meningioma, breast cancer, thyroid cancer, and malignant tumours of the parotid gland.
Discussion
This systematic review study investigates evidence for health risks associated with dental X-rays including cancer, eye disease, or effects on the thyroid gland. Eleven primary studies and seven systematic reviews were included. The heterogeneity of the studies made a meta-analysis unsuitable.
The included systematic reviews were assed to have a very high or high risk of bias in most cases due to incomplete literature search, such as less than two data bases were searched and/or less than two data extractors. Also, the disclosure of conflict of interest were not presented in many studies. Memon et al. 2019 [53], systematic review presented some evidence for a risk of thyroid cancer due to dental radiography examinations but after the assessment by ROBIS for the identification and selection domain, with the result of a high risk of bias as presented in Table 4.
The literature search is a critical and crucial part of a systematic review that can result in a too narrow search field and/or limitation of keywords if executed careless. For the search and in the retrieving of publications, information specialists were therefore consulted. Our research group included experts in different fields, not only in dentistry for this review, but also an expert within Radiation physics and experts in Health Technology Assessment. But still there can be weaknesses in our study due to misjudgments during the screening process and assessments.
Some of the included studies are old and based their results on material from the first half of the 20^th^ century with the normal settings for the dental radiographic examinations at that time. Preston-Martin et al [65–68] reused some material for more than one study, which has been commented in Table 6. In the same review, more than five studies were included, which decrease the overall certainty due to high risk of reporting bias. The lack of reporting confounding factors that are considered as very important confounders such as ionizing medical radiation, radiotherapy, age and gender for the presented outcome (Table 1); such as cancer, eye diseases, effects on thyroid gland with recall bias makes these studies less reliable. The age of the studies can matter in some of the weaknesses. Thus, to present results that did not pass the quality assessments in a meta-analysis or Synthesis Without Meta-analysis can give the impression of being accurate and reliable and must be avoided for further misinterpretations.
This systematic review shows that the studies included exhibit several weaknesses. Therefore, more studies are necessary to create knowledge based on verified data and contemporary digital techniques. The dental care system is responsible for keeping exposure to x-ray radiation as low as possible (i.e., avoiding overexposure) as dictated by the ALARA (As Low As Reasonably Archivable) principle. Because dental X-ray examinations are frequent, often from a young age, more accurate information from digital records is needed to keep recall bias to a minimum. Such accurate information can be used to discover whether dental X-rays have negative effects on health.
The estimated individual radiation dose may be widely inaccurate if medical radiation exposures are not considered. Some medical exposures, such as from brain CT, could result in radiation doses that are one or several orders of magnitude higher than from dental examinations. Furthermore, it is possible that some conditions require repeated use of both dental and medical X-ray examinations. Thus, failure to account for medical exposures could result in a systematic overestimation of the risks from dental X-ray examinations.
Another known bias is reverse causation between a cancer and radiological examination. It is possible that an x-ray examination was performed because of symptoms from a developing cancer, even though the cancer was not diagnosed until a later examination. An increased cancer incidence has been shown a short time after X-ray examinations, even though the timespan was too short for the cancer to develop [69]. Therefore, an exclusion period, based on the cancer development rate, should be employed before a cancer diagnosis is made.
Future studies must include much larger cohorts and be register-based to avoid the risk of recall bias. Confounding factors that can influence the outcome must also be weighed in. Collaborations with other research groups can be a possible way for more statistical power and accurate data and keeping the risk of reporting bias low.
The technical advances in health and dental care systems with digitalized records makes it possible to follow children from birth up to 18 years of age and assess the exposures of ionizing radiation. Because of the higher accessibility to radiographic examinations, especially in many developed countries, it is important to include all examinations of ionizing radiation even those with low dose such as intraoral radiographs.
Future studies are therefore needed to assess the risk of long-term effects of dental radiography.
In the medical health care, there are joined systems for radiographic examinations that can be accessed by private and public clinics and hospitals. It would be of high value if dental clinics could have the same possibilities to avoid overexposures especially of children and adolescents that are more sensitive to ionizing radiation.
Conclusion
We were unable to establish evidence for negative health effects of dental X-rays among children and adolescents. Our findings highlight the fact that there is a need for new studies with thorough study protocols, including number of subjects, verified data, and adjustments for predefined confounding factors to improve scientific knowledge.
Supporting information
S1 FilePRISMA_2020_checklist.(DOCX)
S1 TableWith 10949 included records.(XLSX)
S2 TableWith 11 included primary studies.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Freeman JP, Brand JW. Radiation doses of commonly used dental radiographic surveys. Oral Surg Oral Med Oral Pathol. 1994;77(3):285–9. doi: 10.1016/0030-4220(94)90301-8 8170662 · doi ↗ · pubmed ↗
- 2Granlund C, Thilander-Klang A, Ylhan B, Lofthag-Hansen S, Ekestubbe A. Absorbed organ and effective doses from digital intra-oral and panoramic radiography applying the ICRP 103 recommendations for effective dose estimations. Br J Radiol. 2016;89(1066):20151052. doi: 10.1259/bjr.20151052 27452261 PMC 5124795 · doi ↗ · pubmed ↗
- 3Matzen LH, Christensen J, Wenzel A. Patient discomfort and retakes in periapical examination of mandibular third molars using digital receptors and film. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(4):566–72. doi: 10.1016/j.tripleo.2008.10.002 19121963 · doi ↗ · pubmed ↗
- 4Gröndahl HG, Lith A, Jönsson G, Persson Y. Approximal caries and frequency of bitewing examinations in Swedish children and adolescents. Community Dent Oral Epidemiol. 1992;20(1):20–4. doi: 10.1111/j.1600-0528.1992.tb 00667.x 1547607 · doi ↗ · pubmed ↗
- 5Gustafsson A, Svenson B, Edblad E, Jansson L. Progression rate of approximal carious lesions in Swedish teenagers and the correlation between caries experience and radiographic behavior. An analysis of the survival rate of approximal caries lesions. Acta Odontol Scand. 2000;58(5):195–200. doi: 10.1080/000163500750051737 11144869 · doi ↗ · pubmed ↗
- 6Sources, effects and risks of ionizing radiation. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) 2012 REPORT.Annex A, VI. Summary and conclusion. p 29–30.
- 7Claus EB, Calvocoressi L, Bondy ML, Schildkraut JM, Wiemels JL, Wrensch M. Dental x-rays and risk of meningioma. Cancer. 2012;118(18):4530–7. doi: 10.1002/cncr.26625 22492363 PMC 3396782 · doi ↗ · pubmed ↗
- 8Preston-Martin S, Mack W, Henderson BE. Risk factors for gliomas and meningiomas in males in Los Angeles County. Cancer Res. 1989;49(21):6137–43. 2790826 · pubmed ↗