Walking versus running and GFR trajectory in healthy young adults
Ronit Calderon-Margalit, Ruth Lev Bar-Or, Arnon Afek, Dorit Tzur, Dana Levin, Dror Ben-Ruby, Ariel Furer, Gilad Twig, Karl Skorecki, Asaf Vivante

TL;DR
Walking more than running is linked to slower kidney function decline in young adults, even within normal kidney function ranges.
Contribution
This study identifies walking as a protective exercise behavior against early kidney function decline in healthy young adults.
Findings
Consistent walking was associated with slower eGFR decline compared to inactivity.
Running was linked to faster eGFR decline and higher risk of future reduced kidney function.
Walking showed dose-dependent benefits with more weekly sessions.
Abstract
The effect of physical activity on the primary prevention of chronic kidney disease (CKD) is unclear. We assessed walking and running as exercise behaviors and their associations with individual-level risk for kidney function decline. We conducted a historical cohort study in which we followed 20,976 young adults. Participants were interviewed periodically about their lifestyle, and clinical parameters were assessed. The decline in estimated glomerular filtration rate (eGFR) over time was divided into quartiles. Using logistic regressions, we estimated the odds ratio (OR) for being in the slowest declining quartile by consistency of running or walking. We also used Cox proportional hazards models to estimate the associations of physical activity with future eGFR < 90 ml/min/1.73m2. All models were adjusted for age, sex, smoking status, family history of kidney diseases, BMI,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
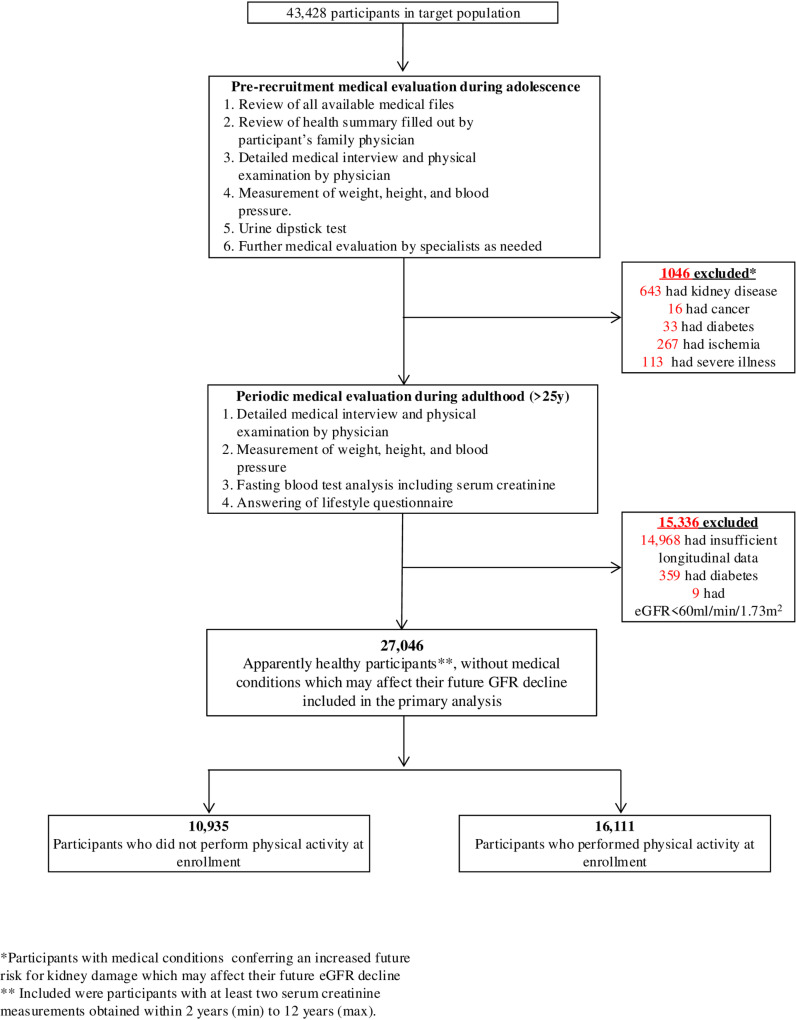 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDialysis and Renal Disease Management · Chronic Kidney Disease and Diabetes · Physical Activity and Health
Introduction
Chronic kidney disease (CKD) constitutes a major public health challenge, with an estimated 700–800 million patients globally and 2.6 million deaths in 2017 [1,2]. Therefore, primary prevention of CKD is a global priority. Inter-individual variability has been reported in the expected age-dependent decline of kidney function [3]. Several factors may contribute to this variability [4]. Lifestyle-related risk factors for kidney function decline are particularly worthy of investigation, as these are often modifiable and can be targeted as part of primary prevention interventions of progressive CKD.
Regular exercise behaviors may influence a person’s kidney function trajectory over time. However, evidence on physical exercise characteristics and kidney function trajectory or kidney disease progression in healthy individuals with normal kidney function is largely based on observational studies or cohorts which mainly investigated elderly patients [5] or persons with established CKD [4,6–8]. Moreover, while some studies suggest an association between physical activity as a kidney function protective behavior [9,10] others show no or inconsistent results [11,12]. Therefore, the long-term kidney health outcomes of consistent physical exercise as a lifestyle behavior among healthy young adults and its relation to other mediating factors remains largely unknown.
Consequently, we conducted a historical cohort study with the use of data from the Metabolic, Lifestyle, and Nutrition Assessment in Young Adults (MELANY) [13–15] Study of the Israel Defense Forces (IDF) Medical Corps and followed 20,976 apparently healthy young men and women to investigate the relationships between walking or running (the most prevalent leisure time physical activities globally [16]) and long-term risk of kidney function decline.
Methods
We conducted a cohort study within the setting of the IDF Medical Corps Staff Periodic Examination Center (SPEC), utilizing data on military personnel who were initially examined between 01/01/1999 and 31/12/2010 and were followed until discharge from military service or 31/12/2020. Data was accessed for research purposes between 01/01/2021 and 31/12/2023.
Study population and clinical assessment
The MELANY study [13–15] is an investigation of risk factors for common diseases in young adults, conducted at the IDF Medical Corps Staff Periodic Examination Center (SPEC). Since the mid-1990s, personnel remaining in the IDF beyond mandatory service were periodically evaluated (every 3–5 years) at the SPEC, beginning at approximately 25 years of age. At each examination, participants completed a detailed questionnaire to provide demographic, health, lifestyle and medical information. Blood samples were drawn following a 14-h fast. In addition, at each SPEC visit, weight, height, and blood pressure were measured, and complete medical interviews and physical examinations were performed. Between SPEC visits, primary care for IDF personnel was provided at designated clinics. For all participants, the SPEC database also includes information ascertained at age 17, coinciding with the initial military recruitment conscription assessment [17,18]. This medical evaluation includes a review of medical records obtained from primary care physicians, a detailed medical history and physical examination, including baseline measurements of weight and height and a manual sphygmomanometric blood pressure measurement (obtained on the right arm in the seated position), routine urinalysis, and, where indicated, referral for further specialty consultations as described below. Accordingly, for all cohort participants, the prior records were reviewed by IDF medical corps physicians, who then elicited and recorded a comprehensive medical history, and conducted a structured thorough and systematic physical examination, including anthropometric measurements, blood pressure, heart rate and a dipstick urinalysis test. If a specific diagnosis could not be fully verified or if its severity could not be graded after the primary medical evaluation, the participant was sent for additional tests and was referred to a board-certified specialist, who may order specific medical tests that will allow more precise diagnosis and classification. Moreover, for each diagnosis, including those established by the specialist during subsequent medical evaluation, the accuracy and completeness of the medical information was additionally assessed by two trained military service physicians who verified the medical information. Each diagnosis is assigned a numerical code and recorded in a central database. This process is uniform for the entire cohort (Fig 1).
Assessment of study participants and designation of study groups.
Inclusion and exclusion criteria
The study comprised 20,976 participants with at least two serum creatinine measurements and at least two SPEC visits. We included persons with at least two serum creatinine measurements obtained over a time interval of between 2–12 years. These participants appeared similar to those with fewer than two serum creatinine measurements in the target population (Table S1). Patients were excluded from the study if they had any of the following at the time of enrollment: (a) confirmed type 1 or type 2 diabetes; (b) estimated glomerular filtration rates (eGFR) of less than 60 ml/min/1.73m^2^; (c) current or past medical history of any stage of acute or chronic kidney disease; (d) microscopic hematuria or proteinuria; (e) ischemic heart disease; (f) past or current diagnosis of cancer and (g) major chronic illness preventing them from military duty (Fig 1).
Physical activity assessment
At each SPEC examination, participants completed a detailed questionnaire containing structured multiple choice questions to provide demographic, health, lifestyle (including smoking), and medical information (including family history of kidney disease). Leisure-time physical activity was assessed in terms of type of exercise (e.g., running, walking, cycling, etc.), weekly frequency, and duration (<45 minutes vs. ≥ 45 minutes per session).
Follow-up and outcomes
Participants were followed-up from their first SPEC visits (01/01/1999-31/12/2010), until retirement from service, or 31/12/2020, whichever came first. We delineated two study outcomes: annual rate of eGFR decline and eGFR < 90 ml/min/1.73m^2^. eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) 2021 equation [19]. Creatinine measurements before 2010 were corrected by 4% reductions, to account for the transition from the Jaffe method to enzymatic creatinine measurements in Israel in 2010 [20]. The primary outcome of mean annual changes in eGFR trajectory was calculated as the eGFR difference divided by the interval in number of years between measurements and then categorized into quartiles. We looked at the lowest (slowest decline) quartile compared to the three upper quartiles.
Statistical analysis
Descriptive statistics of the study population by physical activity are presented as means with standard deviation or proportions. We studied consistency in performing specific types of physical activity, looking into whether a reported activity in the first questionnaire was reported also in a subsequent questionnaire. The associations between consistency of performing a specific type of physical activity and the lowest quartile of eGFR decline were estimated using logistic regressions where inconsistent and consistent physical activity were compared to no physical activity at baseline, controlling for sex, age, smoking, BMI, baseline eGFR, LDL-cholesterol, hypertension, and family history of kidney disease (all from the first questionnaire). We further studied the associations with the weekly mean number of activity sessions (averaged across the two questionnaires) and with the duration of sessions in each questionnaire (answers could not be averaged).
We further estimated the association between types of physical activity and reaching eGFR below 90 ml/min/1.73m^2^, counting time from first eGFR assessment in the cohort until reaching an eGFR < 90 ml/min/1.73m^2^ or last eGFR assessment. Associations were estimated using Cox proportional hazards models. All analyses were conducted in R, version 3.6.1, with the survival models fitted with the coxph function of the survival package. Two-sided p values of less than 0.05 were considered statistically significant.
The Institutional Review Board of the Israel Defense Forces Medical Corps approved the study and waived the requirement for written informed consent on the basis of preserving participants’ anonymity. More specifically, data was analyzed at secured computer stations in the IDF and in an anonymized fashion, such that the data analysts could not track back the participants.
Results
Characteristics of study participants
The characteristics of the cohort of 20,976 participants (85% men) with stratification according to leisure time physical activity (any vs. none) at enrollment are presented in Table 1. The mean age at the prerecruitment medical assessment was 17.5 ± 1.4 years and the mean BMI was 21.1 ± 3.3 kg/m^2^. The mean systolic and diastolic BP were 118.3 ± 11.4 and 73.6 ± 9.1 mmHg respectively.
Table 1: Characteristics of the study population according to physical activity at enrollment.*
Participants were 32.4 ± 5.4 years old at their first SPEC visit and their BMI was 25.8 ± 4.2 kg/m^2^. Participants averaged three SPEC visits per person during follow up (SD: 0.94, range 2–7), and their average first eGFR measured 115.6 (±10.0) ml/min/1.73m^2^ for men and 115.0 (±11.6) ml/min/1.73m^2^ for women. The annual average eGFR declined by 0.97 (±1.6) ml/min/1.73m^2^ per year. Mean quartiles of eGFR reduction rates were 0.31 ml/min/1.73m^2^ per year or less for the bottom quartile (Q1 = “slow GFR decline”) to 1.61 ml/min/1.73m^2^ per year or more for the top quartile (Q4 = “fast GFR decline”). The first estimated eGFR measurement at enrollment for slow decliners (Q1) and fast decliners (Q4) were 108.2 ± 10.8 and 117.3 ± 9.12 ml/min/1.73m^2^, respectively (p < 0.001).
Among the 13,512 participants who reported engaging in physical activity at enrollment, the two most common types of activity were running and walking, which were documented for 26.3% and 18.7% participants respectively. These activities were followed by team sports (9.8%), individual gym fitness workouts (9.2%) and cycling (7.4%). Other activities were reported by less than 5% of the study participants. Given that walking and running were the most common physical activities employed, our primary analysis focused on the associations of consistent walking or running as habitual exercise activities and the eGFR trajectory.
Walking versus running and GFR trajectory
Table 2 presents the associations between consistent and inconsistent engagement in running or walking compared to inactive participants and shows the odds for having a trajectory of slow eGFR decline (Q1). In multivariable models we found that consistent walking showed the highest odds for slow GFR decline as compared to inconsistent or inactive participants. Participants who reported in two consecutive questionnaires that they engaged in walking had an OR of 1.21 (95% CI:1.03–1.41) for being in the slowest eGFR decline quartile (Q1), whereas those who were not consistent in walking had an insignificant increased OR of 1.06 (0.81–1.22). Conversely, participants who consistently engaged in running had significantly decreased odds for slow eGFR decline (OR:0.81, 95% CI:0.71–0.93), whereas inconsistent running was associated with an insignificant reduction in odds (OR:0.87, 95% CI: 0.74–1.01). Similar results were obtained when the first and last questionnaires were analyzed (Table 2). Among consistent walkers, the average number of sessions per week was significantly associated with slow eGFR decline (OR:1.06 [1.00–1.12] per session per week), whereas the number of weekly running sessions was associated with reduced odds of being slow decliners (OR: 0.93 [0.90–0.98] per session per week). Supplementary figure 1 (Fig S1) presents the mean eGFR by age and type of physical activity.
Table 2: The association between consistent habitual running or walking and a slow trajectory of estimated GFR decline (quartile 1)*.
We further assessed whether any of these physical activities reduced future risks of reaching an estimated GFR below 90 ml/min/1.73m^2^ over the study period (Table 3). During 200,005 person years of follow-up (mean: 9.53 ± 4.8 years), 5,409 (25.8%) participants reached an eGFR below 90 ml/min/1.73m^2^. In multivariate Cox models consistent walking was associated with reduced risk for future GFR below 90 ml/min/1.73m^2^ (HR of 0.82 (0.72–0.95)), whereas inconsistent walking was not associated with a reduced risk (HR: 0.94, 95% CI: 0.82–1.07). Conversely, consistent running was associated with an increased risk for future GFR below 90 ml/min/1.73m^2^ (HR: 1.22, 95% CI: 1.09–1.35) while inconsistent running was not associated with increased risk (HR: 1.07, 95% CI: 0.93–1.20). Studying the association of the frequency of physical activity and future eGFR below 90 ml/min/1.73m^2^, we found that walking had an HR of 0.95 (0.90–1.00) for each additional practice per week and running had an HR of 1.07 (1.03–1.11) per practice per week. These associations were not modified by the duration of each practice. Restricting the analyses to those who had less than five years between the first and second questionnaires did not materially change the results. Similarly, stratifying the analyses of the SPEC by year of first SPEC visit (before or after 2010) showed similar results (Table S2). Furthermore, analysis by sex failed to find significant association in females, given the small number of female participants (Table S3).
Table 3: Association between consistent habitual walking or running and future risk of estimated GFR below 90 ml/min/1.73m2.
Discussion
In this study of 20,976 apparently healthy young adults, we found that physical activity behavior of consistent walking, but not consistent running, was associated with slower longitudinal eGFR decline compared to inactive participants. This association starts already within the normal GFR range and was independent of other established risk factors for kidney function impairment. Similar to previous observations [21], we showed that the yearly average physiological GFR decline during adulthood among healthy persons is ~ 1 ml/min/1.73m^2^. In this respect, walking was found to be associated with a higher likelihood of being at the slower eGFR trajectory decline quartile. In addition, walking was associated with lower likelihoods of reaching a eGFR below 90 ml/min/1.73m^2^ at the end of follow-up. Conversely, we found that habitual running might increase the physiological age-dependent kidney function decline. Our findings suggest that among young adults with normal kidney function, habitual walking may have a kidney protective effect.
Several limitations of this study warrant consideration. First, physical activity characteristics (type, duration and frequency) were self-reported and not directly or objectively measured. Nonetheless, we focused on consistent reports across at least two structured questionnaires taken on different occasions and over several years. Second, eGFR was estimated based on serum creatinine and was not measured. This does not account for diet, hydration, or chronic NSAIDs use, which we did not have data on. In addition, we did not measure cystatin C. However, in the normal GFR range there is strong correlation between measured and estimated GFR using the CKD-EPI 2021 formulation [19]. Third, our study population included mainly young and healthy men, limiting the generalizability of our findings to other populations, or even having meaningful insights on gender differences. Finally, we did not have comprehensive information regarding participants’ muscle mass, nutrition and diet, which can also affect kidney health.
The strengths of this study include uniform and detailed data from periodic clinical assessments as well as systematic follow-ups and outcome definitions. In addition, the use of measured (rather than reported) values for the body mass index, blood pressure, and laboratory results with direct measurements of serum creatinine, lipids and glucose in fresh venous blood, provided reliable determinations. This allowed us to control for other confounding CKD risk factors. Moreover, the medical assessments of all study participants during adolescence which were performed under similar protocols as well as subsequent standardized follow-up medical evaluations, allowed us to adhere to consistent inclusion and exclusion criteria and to uniquely study the question of the association between physical activity among healthy adults and kidney function decline in our cohort.
Few previous studies [9,22] have shown an association between physical activity and improved kidney function. In a short-term prospective study among elderly participants (age 70–89 years) with baseline eGFR of 54 ml/min/1.73m^2^, moderate-intensity physical activity slowed the rate of decline in eGFR over a subsequent follow-up period of two years [22]. In another large cohort study of nearly 200,000 Taiwanese adults, a higher level of physical activity was associated with smaller decreases in eGFR and in a lower risk of developing CKD [9]. In a recent comprehensive study which included two large and heterogeneous cohorts from the UK Biobank, with participants having a mean age of 63 years, physical activity of light, moderate or vigorous intensity was associated with lower risks of developing CKD [5]. The latter association of intense physical activity as a kidney protective effect is opposed to our findings as well as to the conventional physiological knowledge and previous studies [23]. Our study confirms the protective effect of walking as opposed to running among healthy individuals already within the normal GFR range.
The lack of a renal protective effect among participants who run may have several explanations. First, during running, blood pressure increases [24,25], leading to renal autoregulation adjustments which in the long-term may affect the overall GFR trajectory. Second, runners may have subclinical myoglobinuria and hemoglobinuria which may lead to subtle kidney damage effecting the overall long-term physiological GFR decline [26]. Third, runners, as opposed to walkers, are prone to recurrent small volume depletion events, as well as to chronic use of non-steroidal anti-inflammatory (NSAIDs) nephrotoxic medications, both of which can contribute to ongoing subclinical kidney damage [27–29]. Finally, it is plausible that this negative effect of running on GFR trajectory is an isolated kidney-specific phenomenon [28,30], otherwise showing protective effect on cardiovascular morbidity and mortality. Therefore, the association between running and physiological GFR decline needs further investigation.
Another interesting finding gleaned from our study is that participant with GFR towards the higher limit of the normal GFR range, had a faster GFR decline compared to participants with lower, normal values. While no single definition of glomerular hyperfiltration has been agreed upon, a commonly used definition for normal GFR is 90–120 ml/min/1.73m^2^ [31–34]. In this study, participants with GFR at the ~ 110 ml/min/1.73m^2^ range had a slower GFR decline compared with those in the 120 ml/min/1.73m^2^ range. This may imply that a GFR of 120 ml/min/1.73m^2^ represents relative “hyperfiltration” which may be more detrimental to the future kidney function trajectory over time and, therefore, we should set the “normal” GFR at the 110 ml/min/1.73m^2^ range. Consequently, this highest eGFR level within the normal GFR range may constitute an independent risk factor for future faster GFR decline among healthy adults.
In conclusion, this large-scale, long-term follow-up study suggests that consistent walking as a physical exercise has a protective effect on kidney health that may delay the physiological kidney function decline. This is an important finding given that mitigating age-related reduction in GFR by habitual walking behavior can be easily applied and prescribed for healthy individuals, as well as to persons with increased risk for future chronic kidney disease.
Supporting information
Table S1Characteristics of 21,038 apparently healthy participants who were not included in the primary analysis compared to the study cohort.(DOCX)
Table S2Sensitivity analysis by year of first SPEC visit.(DOCX)
Table S3Association between consistent habitual running or walking and a slow trajectory of estimated GFR decline stratified by sex.(DOCX)
Fig S1eGFR trajectories by type of physical activity.(TIF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395(10225):709–33. doi: 10.1016/S 0140-6736(20)30045-3 32061315 PMC 7049905 · doi ↗ · pubmed ↗
- 2Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl (2011). 2022;12(1):7–11. doi: 10.1016/j.kisu.2021.11.003 35529086 PMC 9073222 · doi ↗ · pubmed ↗
- 3Li L, Astor BC, Lewis J, Hu B, Appel LJ, Lipkowitz MS, et al. Longitudinal progression trajectory of GFR among patients with CKD. Am J Kidney Dis. 2012;59(4):504–12. doi: 10.1053/j.ajkd.2011.12.009 22284441 PMC 3312980 · doi ↗ · pubmed ↗
- 4Nicholas SB. Structural Predictors of Renal Function Decline. Clin J Am Soc Nephrol. 2016;11(2):202–4. doi: 10.2215/CJN.13431215 26792531 PMC 4741051 · doi ↗ · pubmed ↗
- 5Zhang X, Liu Y-M, Lei F, Huang X, Liu W, Sun T, et al. Association between questionnaire-based and accelerometer-based physical activity and the incidence of chronic kidney disease using data from UK Biobank: a prospective cohort study. E Clinical Medicine. 2023;66:102323. doi: 10.1016/j.eclinm.2023.102323 38024479 PMC 10679485 · doi ↗ · pubmed ↗
- 6Zhang L, Wang Y, Xiong L, Luo Y, Huang Z, Yi B. Exercise therapy improves e GFR, and reduces blood pressure and BMI in non-dialysis CKD patients: evidence from a meta-analysis. BMC Nephrol. 2019;20(1):398. doi: 10.1186/s 12882-019-1586-5 31664943 PMC 6821004 · doi ↗ · pubmed ↗
- 7Kelly JT, Su G, Zhang L, Qin X, Marshall S, González-Ortiz A, et al. Modifiable Lifestyle Factors for Primary Prevention of CKD: A Systematic Review and Meta-Analysis. J Am Soc Nephrol. 2021;32(1):239–53. doi: 10.1681/ASN.2020030384 32868398 PMC 7894668 · doi ↗ · pubmed ↗
- 8Robinson-Cohen C, Katz R, Mozaffarian D, Dalrymple LS, de Boer I, Sarnak M, et al. Physical activity and rapid decline in kidney function among older adults. Arch Intern Med. 2009;169(22):2116–23. doi: 10.1001/archinternmed.2009.438 20008696 PMC 2878734 · doi ↗ · pubmed ↗