Urinary TWEAK reflects disease activity in ANCA-associated vasculitis
Ásta Dögg Jónasdóttir, Peter Hemmingsson, Angelina Schwarz, Magnus Söderberg, Annika Wernerson, Abdul Rashid Qureshi, Aleksandra Antovic, Iva Gunnarsson, Annette Bruchfeld

TL;DR
This study shows that urinary TWEAK levels correlate with disease activity in patients with ANCA-associated vasculitis, suggesting it could be a useful biomarker.
Contribution
The study identifies urinary TWEAK as a novel biomarker for monitoring disease activity in ANCA-associated vasculitis.
Findings
Urinary TWEAK-to-creatinine ratio was significantly higher at baseline compared to follow-up in AAV patients.
Urinary TWEAK levels correlated with disease activity, albuminuria, and crescentic changes in AAV.
Serum TWEAK levels did not differ between patients and controls and did not correlate with disease activity.
Abstract
The aim of the study was to investigate urinary and serum tumour necrosis factor (TNF)-like weak inducer of apoptosis (TWEAK) as potential biomarkers in a longitudinal cohort of patients with ANCA-associated vasculitis (AAV). Patients with active AAV were included in the study. The Birmingham Vasculitis Score 2003 (BVAS) was used for assessment of disease activity and C-reactive protein (CRP), creatinine, albuminuria, and serum (s) and urinary (u) TWEAK levels were measured at baseline and 6-month follow-up. sTWEAK was measured in population-based controls for comparison. Kidney biopsies from AAV patients were stained for TWEAK and its receptor fibroblast growth factor-inducible 14 (Fn14) using immunohistochemistry (IHC). sTWEAK was measured in 74 patients and uTWEAK in 69 patients, 42 of whom had kidney involvement. uTWEAK-to-creatinine ratio (uTWEAK/Cr) was significantly higher at…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
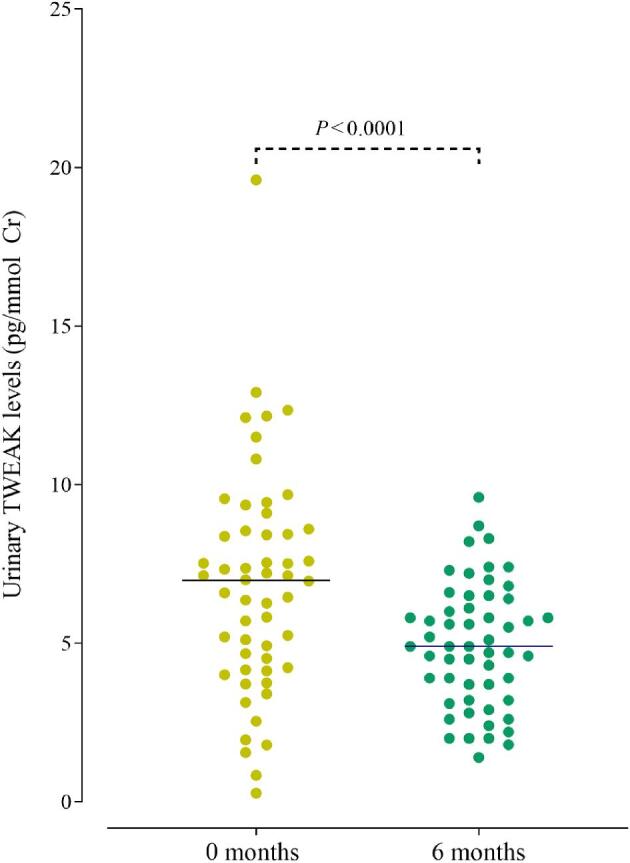 Figure 1
Figure 1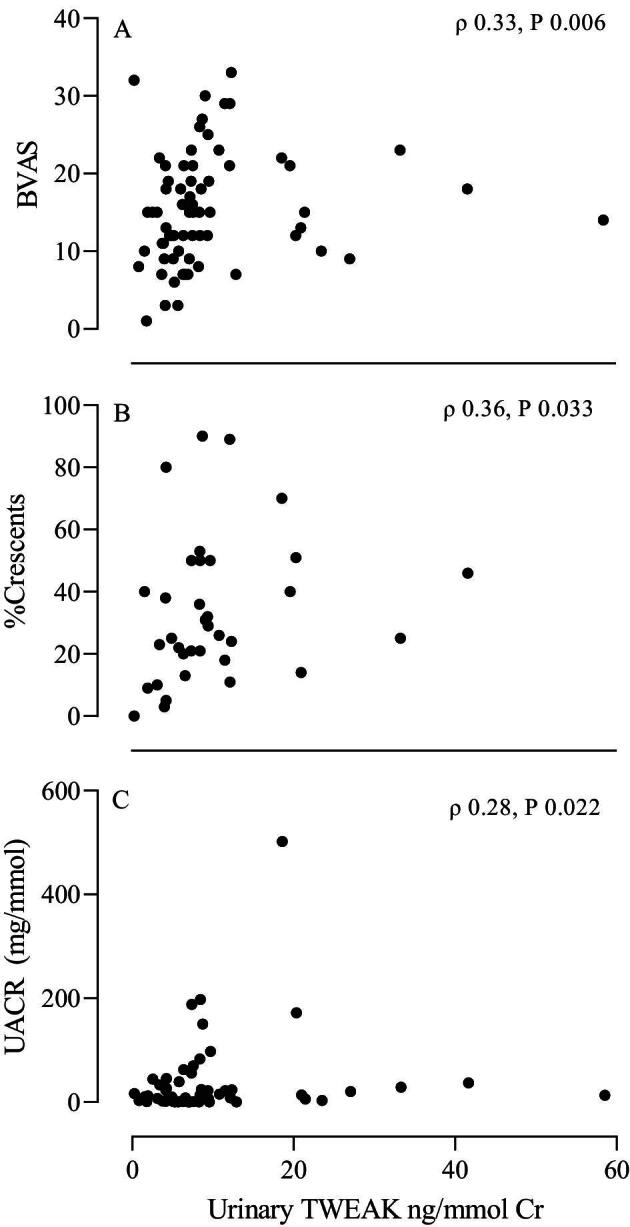 Figure 2
Figure 2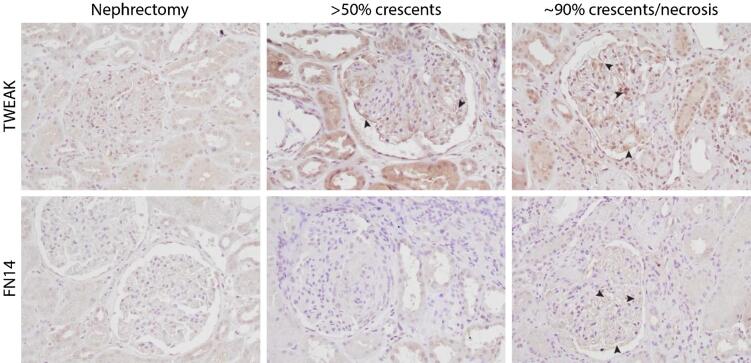 Figure 3
Figure 3|
|
|
|
|
|---|---|---|---|
| Age, years | 58 (48–69) | 64 (59–70) | .12 |
| Sex, female/male | 32 (43.2)/42 (56.8) | 6 (30)/14 (70) | .32 |
| ANCA | |||
| PR3 | 47 (63.5) | ||
| MPO | 27 (36.5) | ||
| Diagnosis | |||
| GPA | 53 (71.6) | ||
| MPA | 17 (23.0) | ||
| EGPA | 4 (5.4) | ||
| New diagnosis | 65 (87.8) | ||
| Relapse | 9 (12.2) | ||
| Kidney involvement | 42 (56.7) | ||
| Treatment prior to inclusion | |||
| GCs | 67 (90.6) | ||
| Intravenous GCs | 29 (39.2) | ||
| Median cumulative GC dose at baseline, mg | 525 (150–1875) | ||
| Cyclophosphamide | 21 (28.4) | ||
| Rituximab | 3 (4.1) | ||
| Methotrexate | 6 (8.1) | ||
| Mycophenolate mofetil | 2 (2.7) | ||
| Induction treatment | |||
| Cyclophosphamide | 47 (63.5) | ||
| Rituximab | 16 (21.6) | ||
| Methotrexate | 12 (16.2) | ||
| Mycophenolate mofetil | 5 (6.8) | ||
|
|
|
|
|
|---|---|---|---|
| BVAS | 15 (9.8–21.0) | 0 (0.0–0.0) |
|
| Plasma creatinine, μmol/L | 86 (69.0–144.3) | 91.5 (80–124.5) | .93 |
| eGFR, mL/min/1.73 m2 | 79.5 (37.7–102.8) | 71.3 (45.8–89.3) | .06 |
| Serum CRP, mg/L | 10 (3.0–28.0) | 2 (0–4.3) |
|
| Haematuria, no. (%) | 42 (56.8) | 11 (15.3) |
|
| UACR, mg/mmol | 8.95 (0.9–25.8) | 3.0 (0.7–15.0) |
|
| Serum TWEAK, pg/mL | 465.6 (356.9–707.3) | 436.1 (347.6–547.3) |
|
| Urinary TWEAK, ng/mmol Cr | 7.2 (4.6–9.6) | 4.9 (3.6–6.5) |
|
|
| ||||
|---|---|---|---|---|
|
|
|
|
|
|
| BVAS | −0.062 | .596 | 0.327 |
|
| Serum CRP (mg/L) | 0.009 | .942 | 0.079 | .519 |
| Plasma creatinine (μmol/L) | −0.326 |
| 0.180 | .138 |
| eGFR | 0.313 |
| −0.208 | .087 |
| UACR (mg/mmol) | −0.146 | .234 | 0.277 |
|
| Serum TWEAK (pg/mL) | −0.156 | .201 | ||
| Urinary TWEAK ng/mmol Cr | −0.156 | .201 | ||
| Cumulative GC dose | −0.267 |
| 0.281 |
|
| Percentage crescents | −0.288 | .07 | 0.362 |
|
- —Region Stockholm
- —Swedish Kidney Foundation
- —Landspitali University Hospital Research Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNF-κB Signaling Pathways · Cell Adhesion Molecules Research · Nuclear Receptors and Signaling
INTRODUCTION
Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a group of necrotizing vasculitides characterized by inflammation of small- to medium-sized vessels and the presence of ANCAs [1]. The clinical presentation varies greatly, ranging from localized manifestations to multisystem organ involvement. Kidney involvement is common in AAV and can lead to kidney failure with the need for kidney replacement therapy [2, 3]. Disease flares are frequent, with >50% of patients experiencing a relapse within 5 years from diagnosis [2, 4, 5]. Simple and non-invasive methods for assessment of kidney disease activity are lacking, rendering follow-up of these patients challenging.
Tumour necrosis factor (TNF)-like weak inducer of apoptosis (TWEAK) is a type II transmembrane glycoprotein that belongs to the TNF cytokine superfamily. TWEAK is cleaved by proteolysis and circulates in the plasma in a soluble form in trimers. TWEAK expression has been demonstrated in various inflammatory cells such as dendritic cells, monocytes, and natural killer cells [6–8] as well as in tubular and endothelial cells in the kidney [9, 10]. TWEAK binds to its receptor, fibroblast growth factor-inducible-14 (Fn14) [11]. Fn14 is expressed by various cells, including endothelial and epithelial cells [12] as well as podocytes and tubular and mesangial cells in the kidney [13]. The expression of Fn14 is low in healthy tissues but is upregulated in tissue injury [14]. The effects of TWEAK/Fn14 vary depending on circumstances and cells involved but include upregulation of inflammatory cytokines [15], induction of endothelial cell survival and proliferation [16], cell death by apoptosis and necrosis [17, 18], and induction of fibrogenesis [19].
Increased expression of TWEAK and its receptor Fn14 has been described in the settings of acute and chronic kidney injury [20]. Fn14 expression is upregulated after kidney injury, and TWEAK exerts enhanced pro-inflammatory effects in these settings [13, 21].
Elevated serum TWEAK (sTWEAK) levels have been shown to correlate with disease activity in systemic lupus erythematosus (SLE) [22, 23]. Furthermore, urinary TWEAK (uTWEAK) has been suggested to be a potential biomarker in lupus nephritis (LN) and IgA nephropathy (IgAN) [24, 25].
The aim of this study was to investigate the role of serum and urinary TWEAK as potential biomarkers of disease activity and markers of kidney involvement in a longitudinal cohort of patients with AAV.
MATERIALS AND METHODS
Patients and methods
Patients with active AAV from the Departments of Nephrology and Rheumatology at Karolinska University Hospital in Stockholm were included close to the start of induction treatment for either newly diagnosed AAV, or a disease flare. Patients were followed prospectively for 6 months. Serum samples from a population-based cohort were used as a disease-free control group [26].
Disease activity and kidney involvement
The Birmingham Vasculitis Score 2003 (BVAS) [27] was used for assessment of the disease activity. Disease remission was defined as a BVAS of 0. Kidney biopsy consistent with pauci-immune-vasculitis or clinical findings of affected kidney function and/or significant haematuria (≥2+ on dipstick urinalysis and/or >10 erythrocytes per high-power field on urinary sediment) was defined as kidney involvement.
Treatment
Remission induction and remission maintenance therapy were documented. The cumulative glucocorticoid (GC) doses given before baseline sampling were calculated in prednisolone-equivalent milligrams and daily doses at inclusion and follow-up were recorded. In patients included at the time of a disease relapse, low-dose GCs (up to 10 mg) given before the relapse as maintenance therapy were not included in the calculation.
Ethics
The study was conducted in accordance with the Declaration of Helsinki and the study protocol was approved by the Regional Ethical Review Board in Stockholm and the Swedish Ethical Review Authority. A written informed consent was obtained from all participants at inclusion.
Laboratory analysis
Peripheral venous blood and urine samples were frozen and stored at −70°C for future analysis. Routine laboratory analyses were carried out using standard methods at the Karolinska University Hospital, including serum C-reactive protein (CRP) plasma creatinine, urine albumin-to-creatinine ratio (mg/mmol), and urinalysis. Urine kappa, lambda, and protein HC (α1-microglobulin) were measured using standard methods at the Karolinska University Hospital and normalized to urine creatinine concentrations. Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD–EPI) equation [28].
Analysis of ANCA serology was performed with an enzyme-linked immunosorbent assay (ELISA) (direct ELIA, Euro Diagnostic) or a multiplex (BioPlex™ 2200, Bio-Rad) according to routine clinical practice at the Department of Clinical Immunology at Karolinska University Hospital. sTWEAK and uTWEAK levels were measured with a commercially available ELISA kit from Bioscience (Hatfield, UK). uTWEAK levels were normalized to urine creatinine concentrations measured in the same urine sample (ng/mmol).
Immunohistochemical staining
Kidney biopsies from two AAV patients were stained using immunohistochemistry (IHC). Macroscopically unaffected tissue from nephrectomized kidney cancer patients was used as a control. The biopsies and tissues were paraffin-embedded and sectioned into 1.5-µm thick sections at the Pathology Kidney Laboratory at Karolinska University Hospital. For IHC the avidin/biotin blocking kit (Vector Laboratories SP2001) and DAB Substrate Kit, Peroxidase (Vector Laboratories SK-4100) were used according to the manufacturer's guidelines. Previous deparaffinization and hydration were performed through washing steps of xylene and ethanol (100%, 95%, 70%) and MilliQ. Antigen retrieval was achieved by microwaving the slides for 25 min in 10 mM citrate buffer (pH 6). Primary antibodies anti-human TWEAK R/Fn14 (R&D Systems, AF1199) and anti-TWEAK (Bioworld Technology, Inc., BS2454) were used at 4°C overnight, and as secondary antibodies horse anti-goat IgG antibody (H + L), biotinylated (Vector Laboratories, BA-9500-1.5), and goat anti-rabbit IgG, biotinylated (Vector Laboratories, BA-1000-1.5), were used.
Histopathological classification score
A histopathological classification score (Berden score) for AAV that distinguishes the pattern of kidney injury in four classes – focal, mixed, sclerotic, and crescentic – was used to score all available kidney biopsies [29]. An experienced kidney pathologist (M.S.), blinded to patient data, scored the biopsies. Kidney biopsy reports were also reviewed for percentage of crescents.
Statistics
Normally distributed variables are presented as mean and standard deviation (SD), non-normally distributed variables as median and 25th–75th percentiles, and categorical variables as frequency and percentage. The non-parametric Wilcoxon signed rank test was used for comparison between time points, the non-parametric Wilcoxon rank sum test to assess the difference between groups, and Fisher's exact test for comparison of categorical data. Correlations were analysed using the non-parametric Spearman rank test. Statistical significance was defined as P < .05. Statistical analysis was performed with JMP software (version 14, SA Campus Drive, Cary, NC, USA) and GraphPad Prism (version 9, GraphPad Software, La Jolla, CA, USA).
RESULTS
Patients
Seventy-four patients with active AAV were included in the study (Table 1). All patients were ANCA-positive, 47 for proteinase-3 (PR3) ANCA and 27 for myeloperoxidase (MPO) ANCA. For comparison, sTWEAK levels were also measured in 20 population-based controls. The baseline characteristics of patients and controls and demographic data are shown in Table 1.
Treatment
At inclusion all except seven patients had commenced induction treatment at the time of sampling (median 5 days, range 0–37 days). Treatment is shown in Table 1. At the 6-month follow-up, remission maintenance treatment with azathioprine, mycophenolate mofetil, methotrexate or rituximab had been initiated in 55 (74.3%) of the patients.
Disease activity and phenotype
The median BVAS at baseline was 15 and decreased to a median of 0 at the 6-month follow-up (*P *< .0001). Most of the patients had multi-organ involvement at inclusion but six patients had only localized ear, nose and throat manifestations. Forty-two (56.8%) of the patients had kidney involvement at baseline, in 39 patients confirmed with a kidney biopsy and in the remaining three by fulfilling the criteria for a clinical diagnosis (Table 1). At follow-up, all except five patients were in remission (BVAS 0); none had active kidney involvement.
Laboratory results
Urinary TWEAK
Urine samples for measurement of TWEAK-to-creatinine ratio (uTWEAK/Cr) were available in 69 of the subjects. uTWEAK/Cr levels were higher at baseline compared with follow-up (median 7.21 vs 4.94 ng/mmol, P < .001) (Table 2 and Fig. 1). uTWEAK/Cr was higher at baseline in patients with kidney involvement compared with those without (median 8.49 vs 6.34 ng/mmol, P = .03). PR3-ANCA-positive patients showed similar uTWEAK levels compared with MPO-ANCA-positive patients. There was no significant difference in uTWEAK/Cr between patients in remission and the five patients who remained active at 6 months.
Urinary TWEAK-to-creatinine ratio in ANCA-associated vasculitis patients at baseline (0 months) and 6-month follow-up. Non-parametric Wilcoxon signed rank test.
A correlation was found between uTWEAK/Cr and BVAS (ρ = 0.33, P = .006) and between the grade of albuminuria and uTWEAK/Cr (ρ = 0.28, P = .022) at baseline (Table 3 and Fig. 2). No difference in uTWEAK/Cr levels between patients with and without significant haematuria at baseline or at follow-up was found. No correlation was seen between uTWEAK/Cr and sTWEAK levels. Measurement of the low molecular weight proteinuria markers urine kappa, lambda, and protein HC was available in nine patients with kidney involvement at baseline. No correlation was found between any of these urine proteins and TWEAK/Cr (data not shown).
Correlation between urinary TWEAK-to-creatinine ratio and (A) disease activity (BVAS), (B) percentage crescents on kidney biopsy, and (C) urinary albumin-to-creatinine ratio (UACR) at baseline. Spearman correlation coefficient.
Serum TWEAK
sTWEAK levels were significantly higher at baseline compared with follow-up (median 465.6 vs 436.1 pg/mL, P = .009) (Table 2). However, no significant differences were found between sTWEAK levels in controls compared with patients at baseline (P = .67) or follow-up (P = .054). Moreover, no differences were found in sTWEAK levels in remission and in those with active disease at follow-up or in patients with kidney involvement compared with those without.
No association was noted between sTWEAK levels and BVAS at inclusion but a correlation was found between sTWEAK levels and creatinine (ρ = −0.326, P = .005) and eGFR (ρ = 0.313, P = .007) (Table 3)
CRP levels
CRP decreased significantly from inclusion to follow-up (median 10 vs 2 mg/L, P < .0001) (Table 2). There was neither a correlation between CRP and BVAS at baseline nor one between CRP and sTWEAK levels or uTWEAK/Cr (Table 3).
Treatment and TWEAK levels
The uTWEAK/Cr levels at baseline were significantly higher in patients who had received immunosuppressive treatment at inclusion compared with those who were treatment-naive (7.5 vs 5.7 ng/mmol, P = .03). No difference was found in sTWEAK levels between these groups.
A significant correlation was found between the cumulative GC dose at inclusion and uTWEAK/Cr (ρ = 0.28, P = .02) and a negative correlation between the cumulative GC dose at inclusion and sTWEAK levels (ρ = −0.27, P = .02) (Table 3). No association was observed between sTWEAK or uTWEAK/Cr and the daily GC dose at the 6-month follow-up.
There was no difference in sTWEAK levels between patients who had received treatment with cyclophosphamide at inclusion compared with those who had not. However, uTWEAK/Cr levels were higher in patients who had received cyclophosphamide compared with those who had not (9.35 vs 6.30 pg/mL, P = .005). No differences were observed between other treatments groups.
Immunohistochemical staining
Kidney biopsies from two active AAV patients were stained using IHC, one with ∼90% crescents/necrosis and one with >50% crescents. The staining showed a clear expression of TWEAK in the kidney biopsies from AAV patients, involving both glomerular and tubular areas when compared with control kidney tissue. In the glomeruli we found TWEAK accumulation in the formed crescents and podocyte cell body as well as a distinct linear staining pattern, indicating expression in the podocyte foot processes. There was TWEAK expression in circular shapes of endothelial cells lining the capillary walls. Both proximal and distal tubules exhibited increased TWEAK expression. Evaluating TWEAK's receptor, Fn14, we found a slight increase in expression mainly in the kidney sample from the AAV patient with severe crescent/necrosis (around 90%). The control tissue showed faint podocyte and endothelial glomerular staining but in the severe AAV case there was upregulated expression of Fn14 in a linear pattern, indicating expression in the podocyte foot processes and increased Fn14 expression in the glomerular endothelial cells, seen as small circles (Fig. 3).
Immunohistochemical staining of kidney biopsies from patients with ANCA-associated vasculitis (AAV) against TWEAK and its receptor, Fn14. Both anti-TWEAK and anti-Fn14 show increased stain for the patients’ biopsies with crescentic manifestations of AAV compared with the control nephrectomy tissue. The arrows highlight a few points of expression in the glomeruli and podocytes. Magnification 20×.
Histopathological classification score
Kidney biopsies were available for 39 patients. Histopathological Berden classification was performed on 28 biopsies. Twelve of the biopsies were classified as focal, eight as mixed, three as sclerotic and five as crescentic. There were no significant differences in sTWEAK or uTWEAK/Cr levels across these groups (Supplementary Table 1). All biopsy reports (n = 39) were subsequently reviewed for percentage of crescents. A significant correlation was found between the percentage of crescents and uTWEAK/Cr (ρ = 0.36, P = .03) (Fig. 2) but was not observed for sTWEAK.
DISCUSSION
In this study, the role of TWEAK as a possible biomarker was investigated in a longitudinal cohort of AAV patients. We found that uTWEAK levels were higher in patients with active disease compared with at follow-up and correlated with disease activity assessed by BVAS. We also found an association between uTWEAK and albuminuria as well as the extent of crescentic changes on kidney biopsies. uTWEAK levels were elevated in patients with AAV kidney manifestations compared with those without. Our findings indicate a role for TWEAK in AAV and suggest that uTWEAK could be a potential non-invasive biomarker in AAV.
Our findings are in line with LN studies where higher levels of uTWEAK have been observed in active compared with inactive disease [30–32]. Interestingly, 14 AAV patients with kidney involvement were included in one of these studies as a disease control group and no difference was observed between uTWEAK levels in patients with AAV and LN [33], suggesting that uTWEAK may be a useful marker of kidney inflammation in general. uTWEAK levels have also been shown to be increased in other glomerular diseases [24]. TWEAK is a multifunctional cytokine, believed to promote tissue reparation and regeneration following acute injury, but it also induces tissue damage in the setting of chronic injury [34]. Fn14 and TWEAK have been shown to be upregulated in inflammation in kidney injury and appear to regulate inflammatory responses in tubular epithelial and mesangial cells [9, 35]. We observed increased staining of TWEAK in glomerular and tubular areas in kidney tissue from patients with crescentic pauci-immune necrotizing glomerulonephritis but not in control kidney tissue. This is similar to previously reported findings in patients with IgAN and AAV, where TWEAK and Fn14 were detected in glomerular crescents [24]. Elevated uTWEAK levels in patients with kidney involvement and the upregulated TWEAK expression in kidney tissue from patients with AAV as well as the correlation between uTWEAK levels and the extent of crescentic changes in our study indicate that the TWEAK/Fn14 pathway may be involved in the pathogenesis of ANCA-associated glomerulonephritis. A correlation was found between uTWEAK and the percentage of crescents on the kidney biopsies but we did not observe any association with histopathological Berden classes. These findings could indicate that histopathological parameters such as the extent of crescents are better indicators of the disease severity [36, 37].
We found that uTWEAK levels correlated with albuminuria, but not with other urine proteins (kappa, lambda and protein HC) at baseline, suggesting that uTWEAK levels do not reflect low molecular weight proteinuria. Most LN studies have failed to demonstrate a link between proteinuria and uTWEAK levels [33, 38, 39], although such a correlation has been reported in IgAN [24]. This discrepancy in findings may indicate that uTWEAK is not only a marker of the degree of proteinuria but reflects increased local inflammatory activity and regeneration in the kidney. Sasaki et al. on the other hand reported a correlation between uTWEAK levels and proteinuria in patients with glomerular diseases not characterized by infiltrative inflammation, such as minimal change disease and membranous nephropathy [24]. Whether elevated uTWEAK levels truly reflect local kidney injury and inflammation or rather a damaged glomerular filtration barrier remains therefore unclear.
In contrast to urinary findings, sTWEAK levels did not correlate with disease activity and no significant difference was found in levels between patients and controls. Similarly, a recently published cross-sectional study from our group showed no significant difference in sTWEAK levels when comparing patients with active and inactive AAV or AAV patients and controls [40]. However, we found a correlation between kidney function and sTWEAK. Serum TWEAK levels have been reported to be decreased in patients with kidney failure compared with healthy controls [41, 42]. A potential explanation for this correlation between sTWEAK and eGFR could be an increased uptake of TWEAK by its receptor, Fn14, which is upregulated in inflammatory disease states and injury [13, 14, 43]. Another hypothesis is an upregulation of CD163, which is the TWEAK scavenger receptor [44, 45]. A case study demonstrated that CD163 is abundantly expressed in acute kidney injury [46] and the expression of CD163 has been shown to be upregulated in kidney tissue in acute crescentic glomerulonephritis [47]. TWEAK binding to CD163 results in internalization of TWEAK, potentially decreasing sTWEAK concentrations [48, 49]. Interestingly, urinary CD163 has been suggested to be a potential biomarker in ANCA-associated glomerulonephritis [50]. Future studies are, however, needed to better delineate the relationship between CD163 and TWEAK in AAV.
We found no correlation between serum and urinary TWEAK levels, which further suggests that TWEAK may be upregulated specifically in the kidney during the acute phase of AAV. This is consistent with the results of Sasaki et al. on TWEAK levels in IgAN, where no correlation was found between serum and urinary TWEAK levels [24].
uTWEAK levels were higher in patients on immunosuppressive treatment at baseline and in patients who had received cyclophosphamide compared with those who had not. A positive correlation was also found between the cumulative GC dose and the uTWEAK levels at baseline. This may be due to the size of the cohort but could also be explained, at least partly, by higher disease activity in these patients. Supporting this we found a significant correlation between BVAS and the cumulative GC dose at inclusion.
The strength of our study is the relatively large and well-defined cohort of AAV patients with diverse organ manifestations and the longitudinal follow-up making it possible to observe changes over time and the effect of treatment. One of the limitations of this study is that the majority of the patients were already on induction treatment at inclusion. However as AAVs often are acute and potentially life- and organ-threatening conditions, patient recruitment in studies before treatment onset is challenging. However, the use of immunosuppressive treatment at inclusion did not seem to influence the uTWEAK/Cr levels at baseline. Another limitation is the lack of urine samples from population-based controls for comparison as well as the lack of a disease control group. Furthermore, the relatively small patient cohort with available kidney biopsies might affect the histopathological and clinical correlations.
In conclusion, this longitudinal study of AAV patients demonstrated that uTWEAK was increased at baseline compared with 6-month follow-up. uTWEAK levels also correlated with BVAS and albuminuria and were associated with kidney involvement and histopathological changes, whereas sTWEAK levels were not. These novel findings suggest that uTWEAK may be an interesting non-invasive biomarker to study further in longitudinal AAV follow-up and relapse studies.
Supplementary Material
sfaf086_Supplemental_File
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jennette JC, Falk RJ, Bacon PA et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 2013;65:1–11. 10.1002/art.3771523045170 · doi ↗ · pubmed ↗
- 2Westman KW, Bygren PG, Olsson H et al. Relapse rate, renal survival, and cancer morbidity in patients with Wegener's granulomatosis or microscopic polyangiitis with renal involvement. J Am Soc Nephrol 1998;9:842–52. 10.1681/ASN.V 95842 9596082 · doi ↗ · pubmed ↗
- 3Aasarod K, Bostad L, Hammerstrom J et al. Renal histopathology and clinical course in 94 patients with Wegener's granulomatosis. Nephrol Dial Transplant 2001;16:953–60. 10.1093/ndt/16.5.95311328900 · doi ↗ · pubmed ↗
- 4Hogan SL, Falk RJ, Chin H et al. Predictors of relapse and treatment resistance in antineutrophil cytoplasmic antibody-associated small-vessel vasculitis. Ann Intern Med 2005;143:621–31. 10.7326/0003-4819-143-9-200511010-00005 16263884 · doi ↗ · pubmed ↗
- 5Westman K, Flossmann O, Gregorini G. The long-term outcomes of systemic vasculitis. Nephrol Dial Transplant 2015;30:i 60–6. 25601266 10.1093/ndt/gfu 392 · doi ↗ · pubmed ↗
- 6Michaelson JS, Wisniacki N, Burkly LC et al. Role of TWEAK in lupus nephritis: a bench-to-bedside review. J Autoimmun 2012;39:130–42. 10.1016/j.jaut.2012.05.00322727560 PMC 3428508 · doi ↗ · pubmed ↗
- 7Kim SH, Kang YJ, Kim WJ et al. TWEAK can induce pro-inflammatory cytokines and matrix metalloproteinase-9 in macrophages. Circ J 2004;68:396–9. 10.1253/circj.68.39615056843 · doi ↗ · pubmed ↗
- 8Maecker H, Varfolomeev E, Kischkel F et al. TWEAK attenuates the transition from innate to adaptive immunity. Cell 2005;123:931–44. 10.1016/j.cell.2005.09.022 16325585 · doi ↗ · pubmed ↗