Efficacy and safety of fondaparinux in elective total hip arthroplasty and hip fracture surgery: a systematic review and meta-analysis
Gonzalo Mariscal, Francisco José Tarazona-Santabalbina, Oliver Marin-Peña, Erika Rotavista, Sara Arroyo Martín, María Estrella Fernández de Sevilla, Jesús Gómez-Vallejo

TL;DR
This study finds that fondaparinux is more effective than other anticoagulants in preventing blood clots after hip surgeries, with similar safety and lower costs.
Contribution
A systematic review and meta-analysis comparing fondaparinux to other anticoagulants in hip surgery patients, highlighting its efficacy, safety, and cost-effectiveness.
Findings
Fondaparinux significantly reduced VTE and DVT compared to LMWHs in hip surgery patients.
Fondaparinux had similar bleeding rates but lower costs per thromboembolic event than enoxaparin.
Proximal DVT was significantly reduced with fondaparinux, though not significantly compared to enoxaparin.
Abstract
As life expectancy increases, the incidence of hip fractures and the demand for total hip arthroplasties (THA) are expected to rise. This demographic shift poses significant challenges, particularly in managing post-operative complications such as venous thromboembolism (VTE), a major cause of mortality. Despite advancements, the effectiveness of various anticoagulants, in preventing VTE post-THA or hip fracture surgery remains unclear due to conflicting study results. This study aims to thoroughly evaluate the efficacy and safety of fondaparinux in patients undergoing elective THA or hip fracture surgery. This review adhered to PRISMA guidelines. Inclusion criteria targeted studies on hip surgery patients treated with fondaparinux versus placebo or other anticoagulants. Data was collected from three major databases in November 2024 using the PICOS framework, focusing on following…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
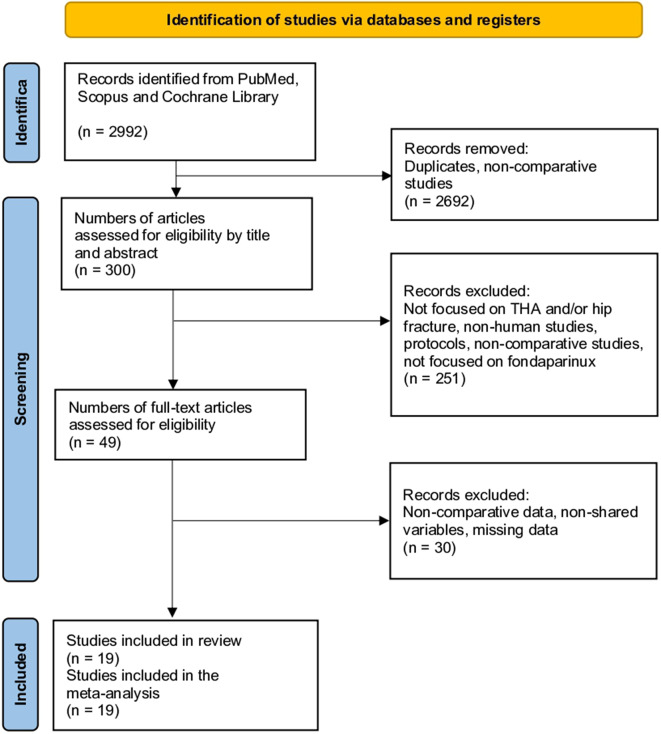 Figure 1
Figure 1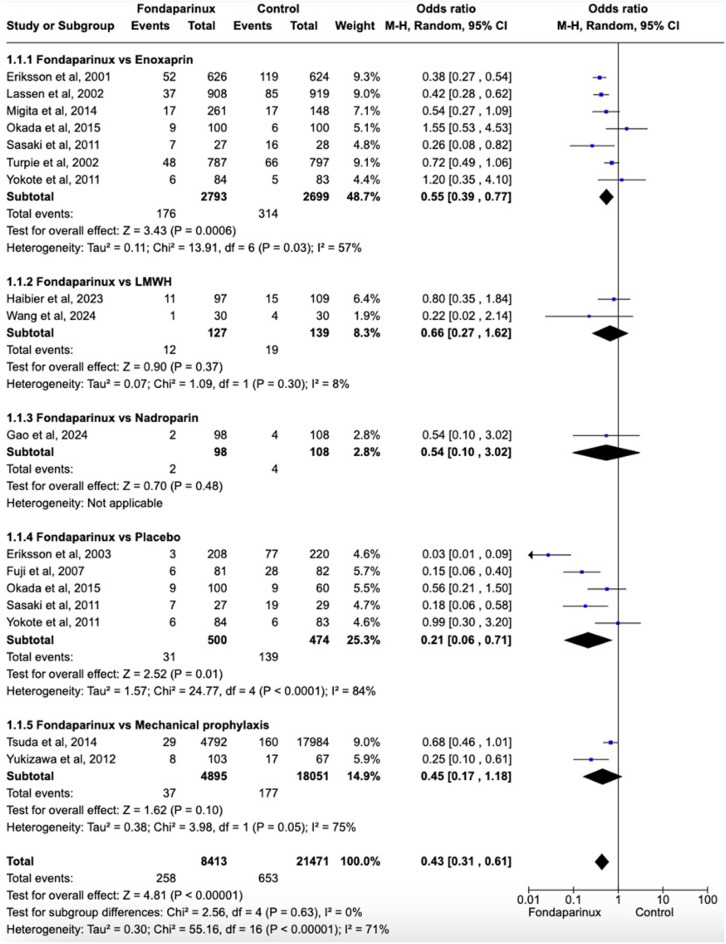 Figure 2
Figure 2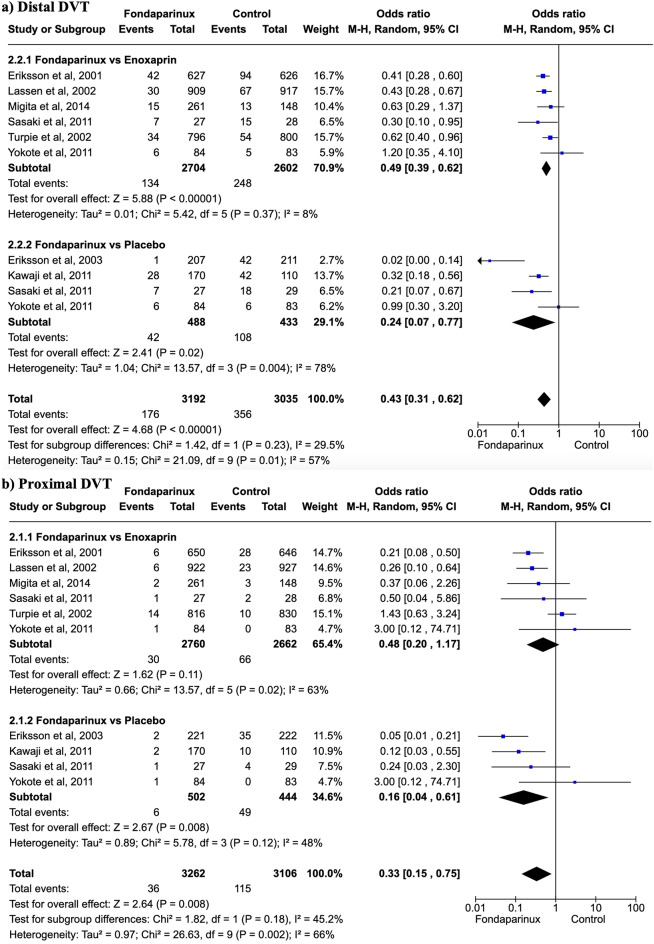 Figure 3
Figure 3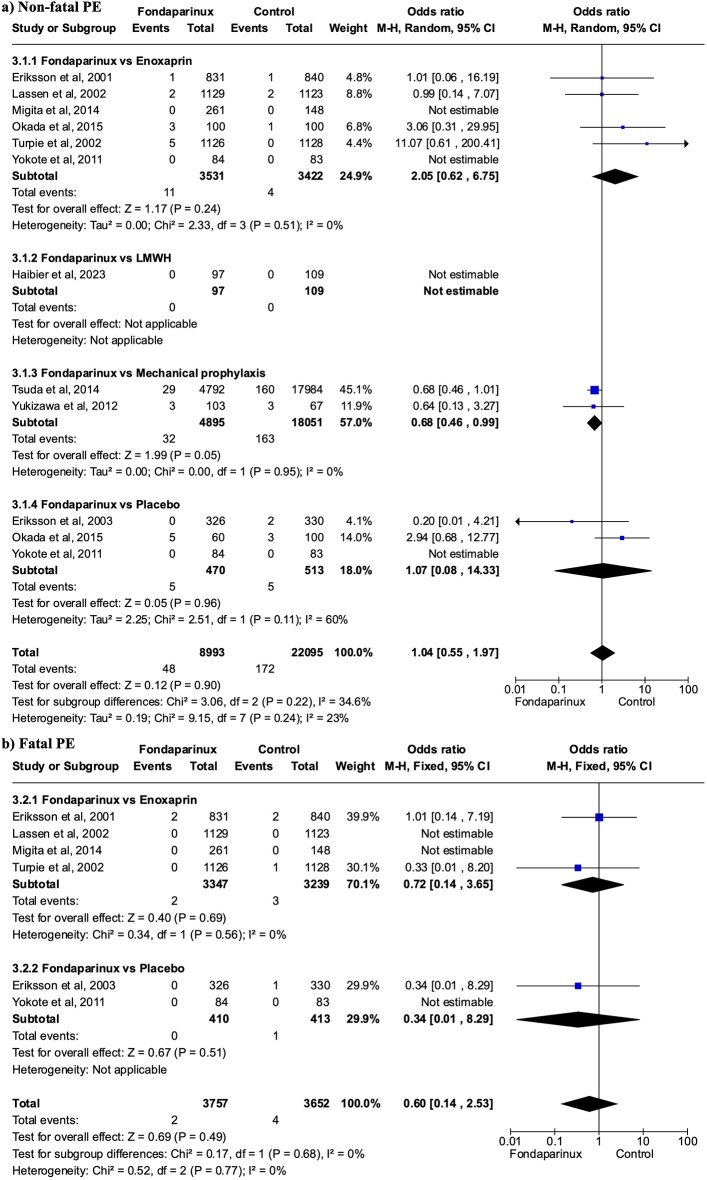 Figure 4
Figure 4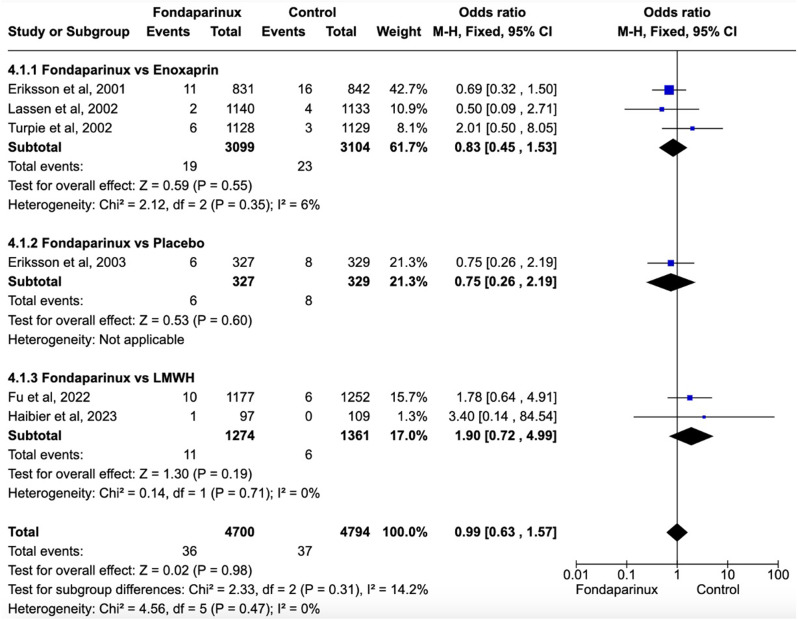 Figure 5
Figure 5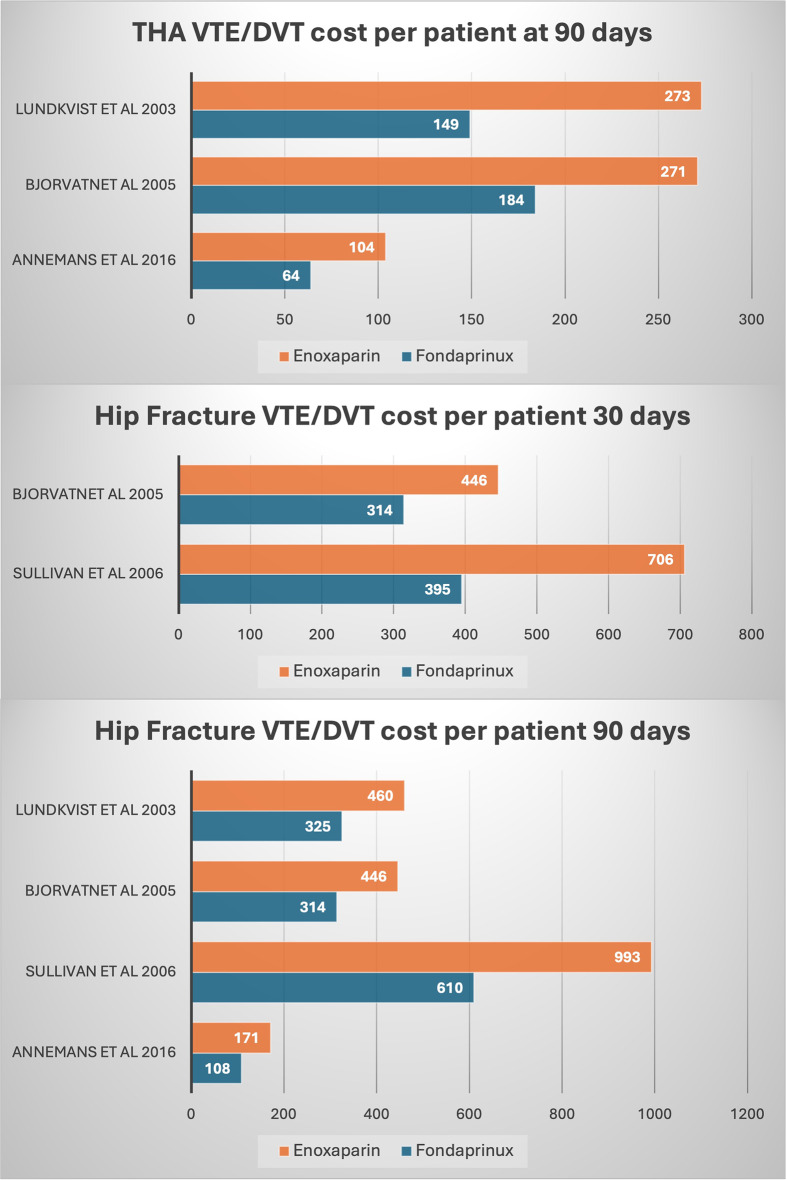 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Heparin-Induced Thrombocytopenia and Thrombosis · Orthopaedic implants and arthroplasty
Introduction
Hip fractures and the need for total hip arthroplasty (THA) are on the rise in tandem with longer life expectancies and an aging population [1]. For healthcare systems around the world, this demographic transition poses serious issues, especially when it comes to managing postoperative complications [2, 3]. According to projection models, the aging population will be a major contributing factor in the huge increase in hip fracture incidence and health burden by 2029, which will present significant problems for the health and social care systems [4]. Venous thromboembolism (VTE), which includes the extremely severe conditions of deep vein thrombosis (DVT) and pulmonary embolism (PE) [5]. VTE has a major impact on quality of life, patient outcomes, and the use of medical resources [6]. VTE is one of the most common complications that lead to postoperative morbidity and mortality.
The overall mortality rate is still high even if the postoperative VTE rate is modest [5–7]. Due to their increased risk of postoperative complications and death, patients with hip fractures are especially vulnerable since they frequently have several comorbidities [5, 6]. To improve both immediate and long-term outcomes, a multidisciplinary approach might be essential [7]. During the pandemic, VTE-related death rates rose after remaining stable since 2008 [8].
Fondaparinux has shown significant potential, but its effectiveness in preventing VTE after hip fracture or THA compared with other anticoagulants remains debated. Conflicting findings from various studies have created uncertainty regarding the optimal role of fondaparinux as a prophylactic agent for VTE. Sasaki et al. demonstrated that fondaparinux had a lower incidence of VTE than enoxaparin [9]. However, other studies showed a tendency to favor fondaparinux but without statistically significant differences [10, 11]. Regarding the risk of bleeding, Erikson et al. observed less minor bleeding with enoxaparin; however, there was no difference in fatal bleeding. In contrast, Lassen et al. noted a lower incidence of DVT with fondaparinux but an increase in the number of transfusions [12]. However, the increased bleeding did not require reoperation. These inconsistent results highlight the need for a thorough analysis and careful evaluation of the available evidence.
These concerns have been the focus of previous meta-analyses, but they ran into issues that call for more research. Hur et al. [13], for instance, only examined four studies, which might not give a complete picture. Similarly, Huang et al. [14] ignored hip fractures in favor of concentrating only on total hip arthroplasty. There may be gaps in the results since these analyses did not take into consideration all the variables that were necessary to control heterogeneity.
In order to prevent VTE following THA and hip fracture surgery, this systematic review and meta-analysis sought to provide a thorough evaluation of fondaparinux’s safety and effectiveness in comparison to other options. Evidence-based recommendations for VTE prophylaxis can be influenced by these findings.
Methods
Eligibility criteria
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) were followed in the conduct of this review [15]. For this investigation, the protocol was registered with PROSPERO (CRD42025636847). To choose relevant studies, inclusion and exclusion criteria were developed. The PICOS framework was used in this study’s methodology: P (patients) comprised individuals undergoing hip fracture surgery or total hip arthroplasty; I (intervention) involved fondaparinux; C (comparator) comprised patients receiving a placebo or other therapeutic alternatives; O (outcomes) evaluated efficacy, safety and costs; and S (study design) only required comparative studies. No limitations existed on the basis of ethnicity, nation, or gender. Non-human studies (animal studies) and in vitro studies were excluded, as were certain publication types, such as book chapters, editorials, author responses, conference papers, posters, reviews, letters, patents, and papers available only as abstracts. Studies lacking extractable data, those with overlapping or unreliable data, and duplicates were also excluded.
Information sources and search methods for identification of studies
A comprehensive search was performed across multiple databases including PubMed, Scopus, and Cochrane Library in November 2024. Specific search terms were utilized: “fondaparinux,” “hip arthroplasty,” “hip replacement”, “hip fracture”, “orthopedic” and “orthopaedic” (Additional File 1). A manual search of the references was conducted to ensure a comprehensive coverage of the literature. No language or date restrictions were applied.
The study selection process was conducted in two distinct stages: (1) title and abstract screening and (2) full-text review. Initially, all records were identified through a database search, and duplicates were removed using EndNote Software Version (X-9). Two independent reviewers screened the titles and abstracts of all the unique records to assess their potential eligibility based on predefined inclusion and exclusion criteria. Any disagreements at this stage were resolved by discussion or consultation with a third reviewer. Records deemed potentially relevant were proceeded to the full-text review stage. In this phase, the same two independent reviewers assessed full-text articles for eligibility by applying the same inclusion and exclusion criteria in greater detail. The reasons for exclusion at the full-text stage were documented. Discrepancies between the reviewers were resolved by discussion or, if necessary, by a third reviewer.
Data extraction and data items
The data collected from these studies were independently reviewed by two authors. In cases of disagreement, a third author was consulted to resolve the issue and finalize the assessment. Baseline characteristics of the studies included region, study design, type of hip surgery, gender, age (years), BMI, history of venous thromboembolism, and doses of fondaparinux. The primary data extraction focused on VTE, defined as the number of deep vein thrombosis (DVT), pulmonary embolisms (PE), or both. Additional outcomes examined included the incidence of DVT, PE, mortality, and bleeding. For bleeding, rates of minor bleeding were recorded, along with more specific outcomes, such as bleeding in critical organs, bleeding leading to reoperation, fatal bleeding, and the number of transfusions. The costs were also analyzed. Other variables such as operative time, intraoperative blood loss, treatment duration, and creatinine levels were collected to ensure homogeneity between the groups regarding these potential confounding variables.
Assessment of risk of bias in included studies
For non-randomized studies, the risk of bias was assessed using the Methodological Index for Non-Randomized Studies (MINORS) with 12 items [16]. For non-comparative studies, scores ranging from 0 to 4, 5–7, 8–12, and ≥ 13 were categorized as very low, low, fair, and high quality, respectively. In the comparative studies, scores ranging from 0 to 6, 7 to 10, 11 to 15, and ≥ 16 were categorized as very low, low, fair, and high quality, respectively.
The Cochrane Review Manager tool was used to assess the risk of bias in the clinical trials. Randomization, allocation concealment, participant and outcome assessor blinding, insufficient outcome data, selective outcome reporting, and other sources of bias were among the considered domains taken into consideration. Every domain was evaluated for “low risk of bias,” “uncertain risk of bias,” or “high risk of bias” [17].
Assessment of results
Continuous variables measured on the same scale were analyzed for mean differences (MD) and 95% confidence intervals (CI). When outcomes were assessed on different scales or on the same scale with varying units, standard mean differences (SMD) with 95% CI were calculated. Odds ratios (OR) with 95% confidence intervals were used for dichotomous variables. Meta-analysis was conducted using Review Manager version 5.4.1. Heterogeneity among studies was assessed using the chi-square test and I² statistics, with I² values of 25%, 50%, and 75% indicating low, moderate, and high heterogeneity, respectively. A fixed-effects model was employed unless significant heterogeneity was detected (I² ≥ 50%). The variables from the figures were accurately extracted using WebPlot Digitizer 4.5. The handling of missing data adhered to the guidelines set forth in the Cochrane Handbook [18].
Publication bias
Publication bias was assessed using Review Manager software, which is widely utilized for systematic reviews and meta-analyses. To visually evaluate the presence of publication bias, funnel plots were generated. Plotting the treatment effects estimated from individual trials versus a metric of study size or precision—typically the standard error—is done graphically with funnel plots. Asymmetry in the data, which may be a sign of publishing bias, can be found using this technique. The horizontal axis (x-axis) in these maps denotes the study’s size, precision, or standard error, while the vertical axis (y-axis) shows the effects of the therapy. Asymmetry may signal that smaller, possibly unpublished studies with negative or null results are not included in the analysis, whereas a symmetrical distribution of data points around the effect size shows little to no publication bias.
Additional analysis
By removing the study with the highest weight from the comparison across all outcomes, a sensitivity analysis was carried out. For the primary outcomes, further sensitivity analyses were conducted, specifically by classifying the results according to the kind of surgery—total hip arthroplasty and hip fracture surgery.
According to the type of control groups employed, subgroup analyses were conducted using low molecular weight heparin (including studies that did not specify the type, as well as those employing enoxaparin and nadroparin), and comparisons with mechanical prophylaxis, no treatment, or placebo.
Additionally, the GRADEpro tool was used to apply the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework [19]. This method considers variables including risk of bias, heterogeneity, precision of results, and consistency across studies in order to assess the quality of the evidence and the strength of recommendations. A thorough examination and well-informed decision-making based on the quality and dependability of the available data are guaranteed by this all-encompassing method.
Results
Study selection
The initial database search yielded 2,992 studies. After filtering to include only clinical trials and observational studies, 2,692 were excluded, leaving 300 relevant studies. A further examination of titles and abstracts resulted in the exclusion of 251 studies that did not focus on total hip arthroplasty (THA) and hip fractures, were not human studies, lacked comparative data, were merely protocols, or did not concentrate on fondaparinux. After a full-text review of the remaining 49 articles, 30 were removed due to issues such as non-comparative data, non-shared variables, and missing data. No additional articles were identified through reference checks of the included studies. Ultimately, nineteen articles met al.l criteria and were included in the meta-analysis (Fig. 1) [9–12, 20–34].
Fig. 1. Study selection flow diagram (Preferred Reporting Items for Systematic Reviews and Meta-analyses)
Fig. 2. Forest plot showing effects of Fondaparinux in the incidence of VTE versus different control groups. Fondaparinux demonstrated significantly fewer VTE events compared to the control group (OR 0.43, 95% CI 0.31 to 0.61) including LMWHs (OR 0.55, 95% CI 0.41 to 0.74)
Fig. 3. Forest plot showing effects of Fondaparinux in the incidence of distal and proximal DVT versus different control groups. (a) Fondaparinux showed a lower incidence of distal DVT compared to the control group (OR 0.43, 95% CI 0.31 to 0.62), including enoxaparin (OR 0.49, 95% CI 0.39 to 0.62); (b) fondaparinux significantly reduced the incidence compared to the control group (OR 0.33, 95% CI 0.15 to 0.75) but there were no differences compared with enoxaparin (OR 0.48, 95% CI 0.20 to 1.17)
Fig. 4. Forest Plot showing effects of Fondaparinux in the incidence of pulmonary embolism. There were no significant differences neither in the case of non-fatal pulmonary embolism (a) nor fatal pulmonary embolism (b)
Fig. 5. Forest Plot showing effects of Fondaparinux in the incidence of mortality. There were no significant differences in mortality rates between groups
Fig. 6. Mean costs per patient per event of VTE/DVT for fondaparinux versus enoxaparin. Depending on the study, the costs were evaluated in euros, pounds, and/or dollars
Baseline characteristics
Table 1 summarizes the main characteristics of the included studies. There were 15 original studies (n = 32534 patients) based on real-world data comparing fondaparinux with other options [9–12, 20–24, 26–30] and four cost studies based on simulation models [25, 31–34], which is why there were no baseline characteristics for them. The studies were primarily conducted in Japan [9, 23–26, 28–30], China [10, 11, 27], and Sweden [18, 19], utilizing both randomized controlled trials (seven studies) [12, 20–23, 25, 26] and cohort designs (eight studies) [9–11, 24, 27–30]. Among these, seven studies compared fondaparinux with enoxaparin [9, 12, 21–24, 30], two with LMWH [10, 11], one with nadroparin [27], six with placebo [9, 20, 23, 25, 26, 30], and two with mechanical prophylaxis [28, 29]. There were three studies with more than two arms that included data for both the enoxaparin and the placebo groups [9, 23, 30]. Four studies focused on patients undergoing surgery after hip fracture, and eleven studies on elective THA [9, 20, 21, 29]. The average age ranged from 58.0 to 83.0 years. The BMI ranged from 21.4 to 28.0, and the dose of fondaparinux used in the studies was 2.5 mg, except for one study that used 0.25 mg. Regarding the doses of enoxaparin, three studies reported 40 mg [12, 21, 23], one study reported 30 mg [22], another 4000IU [30], and one 2000IU [9]. The remaining studies did not report the doses of enoxaparin, nadroparin, or any other type of LMWH. The type of examination and time of evaluation is shown in Additional Table 1.
Table 1. Baseline characteristics of included studiesStudiesRegionStudy designType of hip surgeryFollow-upSexM(F)Age (yrs)Mean (SD)* Median (Range)BMI (kg/m^2^)Mean (SD)* Median (Range)History of venous thromboembolismN (%)Dose Fondaparinux vs. Enoxaparin Eriksson et al. 2001 [21]SwedenRCTFracture6 weeks187 (644)/224 (618)76.8 (12.3)/77.3 (12.6)23.8 (4)/64.2 (13.8)29 (3.5)/32 (3.8)FDP: 2.5 mg; EXP: 40 mgLassen et al. 2002 [12]DenmarkRCTTHA6 weeks396 (512)/402 (517)* 67 (30–90)/67 (24–97)*26 (15–45)/26 (14–51)35 (4)/ 40 (4)FDP: 2.5 mg; EXP: 40 mgMigita et al. 2014 [24]JapanCohortTHANR128 (740)66.7 (10.5)23.6 (4.2)5 (0.6)FDP: 2.5 mg; EXP: NROkada et al. 2015 [30]JapanCohortTHA7 days22 (78)/9 (91)*58 (35–82)/61 (40–86)*23 (16–40)/24(17–45)NRFDP: 2.5 mg; EXP: 4000 UISasaki et al. 2011 [9]JapanCohortFracture14 days6 (21)/6 (22)79.7 (11.4)/82.4 (7.4)21.4 (4.27)/20.68 (3.58)NRFDP: 2.5 mg; EXP: 2000 UITurpie et al. 2002 [22]CanadaRCTTHA6 weeks556 (572)/522 (607)*67 (18–92)/*67 (19–91)*28 (14–73)/*28 (13–83)52 (5)/ 63 (6)FDP: 2.5 mg; EXP: 30 mgYokote et al. 2011 [23]JapanRCTTHA12 weeks14 (70)/16 (67)63 (10)/64 (11)22.5 (4.8)/23 (3.3)NRFDP: 2.5 mg; EXP: 40 mg Fondaparinux vs. LMWH Haibier et al. 2023 [10]ChinaCohortTHA1 month36 (61)/39 (70)77.17 (5.48)/76.27 (5.06)23.76 (4.03)/23.51 (3.54)NRFDP: 2.5 mg; LWMH: NRWang et al. 2024 [11]ChinaCohortTHA7 days10 (20)/14 (16)71 (2.128)/70.3 (1.714)NRNRFDP: 2.5 mg; LWMH: NR Fondaparinux vs. Nadroparin Gao et al. 2024 [27]ChinaCohortTHANR94 (220)/103 (175)67.06 (10.68)/ 68.85 (10.007)NRNRFDP: 0.25 mg; NDP: Not reported Fondaparinux vs. Placebo Eriksson et al. 2003 [20]SwedenRCTFracture32 days92 (235)/98 (231)*79 (23–94)/*79 (28.96)*24 (15–38)/*24 (15–41)13 (4)/12 (3.6)FDP: 2.5 mgFuji et al., 2007 [25]JapanRCTTHA17 days75 (351)/15 (72)71 (8)/70.4 (7.9)NRNRFDP: 2.5 mgKawaji et al. 2011 [26]JapanRCTTHA14 days22 (70)/15 (95)62.4/62.624.3/23.6NRFDP: 2.5 mgOkada et al. 2015 [30]JapanCohortTHA7 days78 (22)/91 (9)*****58 (35–82)/*****61 (40–86)*****23 (16–40)/*****24 (17–45)NRFDP: 2.5 mgSasaki et al. 2011 [9]JapanCohortFracture14 days6 (21)/5 (24)79.7 (11.4)/83 (7.5)21.4 (4.27)/20.83 (3.76)NRFDP: 2.5 mgYokote et al. 2011 [23]JapanRCTTHA12 weeks14 (70)/16 (67)63 (10)/63 (12)22.5 (4.8)/23.1 (8.1)NRFDP: 2.5 mg Fondaparinux vs. Mechanical prophylaxis Tsuda et al. 2014 [29]JapanCohortFractureNR925 (3867)/3639 (14345)79.2 (9.1)/79.6 (9.4)NRNRNRYukizawa et al. 2012 [28]JapanCohortTHA14 days27 (76)/20 (47)58 (8)/68 (8)24 (5)/24 (6)6 (0.6)/17 (25.4)FDP: 2.5 mgEXP: Enoxaparain; FDP: Fondaparinux; NDP: Nadroparin; NR: Not reported
Risk of bias
The risk of bias for the six clinical trials is shown in Additional Fig. 1. The studies primarily failed in reporting allocation concealment and in blinding outcome assessments (Additional File 2). Regarding the nine non-randomized studies, their evaluation is detailed in Additional Table 2. These studies were found to be of high quality.
Table 2. Bleeding assessmentEffect sizen participantsFixed effect model (OR 95% CI)I^2^ (%)P-Value Minor bleeding Fondaparinux vs. Placebo1019OR 4.19, 95% CI 1.17 to 14.9200.03Fondaparinux vs. Enoxaparin1928OR 1.91, 95% CI 1.10 to 3.3200.02 Bleeding in critical organ Fondaparinux vs. Placebo819N/EN/EN/EFondaparinux vs. Enoxaparin6203OR 0.33, 95% CI 0.01 to 8.19N/A0.50 Bleeding leading to reoperation Fondaparinux vs. Placebo819OR 1.01, 95% CI 0.14 to 7.19N/A1.00Fondaparinux vs. Enoxaparin6203OR 1.43, 95% CI 0.54 to 3.7700.47 Fatal bleeding Fondaparinux vs. Placebo875N/EN/EN/EFondaparinux vs. Enoxaparin6258OR 0.34, 95% CI 0.01 to 8.29N/A0.51 n Transfusions Fondaparinux vs. Placebo656OR 1.50, 95% CI 0.83 to 2.72N/A0.18Fondaparinux vs. Enoxaparin3946OR 1.11, 95% CI 0.98 to 1.26240.10N/A: Not applicable; N/E: Not estimable
Venous thromboembolism
Fondaparinux demonstrated significantly fewer VTE events compared to the control group (OR 0.43, 95% CI 0.31 to 0.61; participants = 29,884; studies = 17; I^2^ = 71%) (Fig. 2). Similarly, a significant difference was observed when compared to LMWHs, including enoxaparin and nadroparin (OR 0.55, 95% CI 0.41 to 0.74; participants = 5,964; studies = 10; I2 = 41%). When compared with placebo or mechanical prophylaxis, fondaparinux significantly reduced the incidence of VTE (OR 0.27, 95% CI 0.11 to 0.62; participants = 23,920; studies = 7; I2 = 84%).
Deep vein thrombosis
Fondaparinux showed a lower incidence of distal DVT compared to the control group (OR 0.43, 95% CI 0.31 to 0.62; participants = 6,227; studies = 10; I2 = 57%) (Fig. 3a). Fondaparinux also demonstrated a lower incidence of distal DVT compared to enoxaparin (OR 0.49, 95% CI 0.39 to 0.62; participants = 5,306; studies = 6; I2 = 8%) and placebo (OR 0.24, 95% CI 0.07 to 0.77; participants = 921; studies = 4; I2 = 78%).
Regarding proximal DVT, fondaparinux significantly reduced the incidence compared to the control group (OR 0.33, 95% CI 0.15 to 0.75; participants = 6,368; studies = 10; I2 = 66%) (Fig. 3b). Compared with enoxaparin, no significant differences were found (OR 0.48, 95% CI 0.20 to 1.17; participants = 5,422; studies = 6; I2 = 48%). Compared with placebo, fondaparinux significantly decreased the incidence of proximal DVT (OR 0.16, 95% CI 0.04 to 0.61; participants = 9,946; studies = 4; I2 = 48%).
Pulmonary embolism and mortality
Regarding non-fatal PE, there were no significant differences between groups (OR 1.04, 95% CI 0.55 to 1.97; participants = 31,088; studies = 12; I^2^ = 23%) (Fig. 4a). In terms of fatal PE, there were also no significant differences observed between groups (OR 0.60, 95% CI 0.14 to 2.53; participants = 7,409; studies = 6; I^2^ = 0%) (Fig. 4b). Additionally, there were no significant differences in mortality rates between groups (OR 0.99, 95% CI 0.63 to 1.57; participants = 9,494; studies = 6; I^2^ = 0%) (Fig. 5).
Bleeding
Minor bleeding was significantly lower in the control group compared with fondaparinux (OR 2.21, 95% CI 1.34 to 3.65; participants = 2,947; studies = 6; I2 = 0%). When divided by subgroups, enoxaparin presented lower minor bleeding (OR 1.91, 95% CI 1.10 to 3.32; participants = 1,928; studies = 3; I2 = 0%) as well as placebo (OR 4.19, 95% CI 1.17 to 14.92; participants = 1,019; studies = 3; I2 = 0%) compared with fondaparinux. There were no significant differences between the groups regarding bleeding in critical organs (OR 0.33, 95% CI 0.01 to 8.19; participants = 7,022; studies = 5; I2 = NA), bleeding leading to reoperation (OR 1.34, 95% CI 0.56 to 3.18; participants = 7,022; studies = 5; I2 = 0%), fatal bleeding (OR 0.34, 95% CI 0.01 to 8.29; participants = 7,133; studies = 7; I2 = NA), or regarding the number of transfusions (OR 1.13, 95% CI 0.99 to 1.28; participants = 4,602; studies = 3; I2 = 12%). Table 2 presents the outcomes related to bleeding.
Costs
The costs were evaluated in euros, pounds, and/or dollars depending on the study. In elective THA at 90 days, fondaparinux presented a cost of 132 versus 216 for enoxaparin. In hip fracture surgery at 30 days, fondaparinux showed a cost of 355 versus 576 for enoxaparin, while at 90 days post-hip fracture surgery, fondaparinux had a cost of 339 versus 518 for enoxaparin. Figure 6 displays the mean costs per patient per event of VTE/DVT for fondaparinux versus enoxaparin.
Sensitivity analyses
Upon removing the study with the most weight from all the main variables, all variables maintained the direction of their results except for proximal DVT, which changed from showing no significant differences between groups to showing that fondaparinux significantly reduced the incidence of proximal DVT compared with enoxaparin (OR 0.27, 95% CI 0.16 to 0.47; participants = 3,776; studies = 5; I2 = 0%).
When assessing the effect according to the type of indication (Table 3), fondaparinux showed a reduction in the incidence of VTE and DVT (proximal and distal) in hip fracture surgery compared to LMWHs. On the other hand, in elective total hip arthroplasty (THA), fondaparinux showed a significant reduction in VTE and distal DVT compared to LMWHs, but there were no differences regarding proximal DVT.
Table 3. Indication-based sensitivity analysis comparing Fondaparinux vs. LMWHs including Enoxaparin and NadroparinEffect sizen studiesn participantsFixed effect model (OR 95% CI)I^2^ (%)P-Value Hip Fracture VTE21305OR 0.37, 95% CI 0.27 to 0.520%< 0.00001Distal DVT21308OR 0.39, 95% CI 0.27 to 0.570%< 0.00001Proximal DVT21351OR 0.22, 95% CI 0.10 to 0.510%0.0004 THA VTE84659OR 0.60, 95% CI 0.48 to 0.7527%< 0.0001Distal DVT43998OR 0.55, 95% CI 0.42 to 0.732%< 0.0001Proximal DVT44071OR 0.65, 95% CI 0.20 to 2.0666%0.46:Random effect model
Publication bias
Publication bias is demonstrated in Additional File 3. There was asymmetry and clustering of studies at the upper end of the funnel plot, indicating the presence of publication bias.
Grade
According to the GRADE framework, VTE, proximal DVT, and fatal bleeding were found to have moderate certainty. Distal DVT demonstrated high certainty, while non-fatal PE showed very low certainty. The studies exhibited publication bias, and for some variables, most of the study designs were non-randomized. Table 4 displays the certainty analysis.
Table 4GRADE assessmentCertainty assessment№ of patientsEffectCertaintyImportance№ of studiesStudy designRisk of biasInconsistencyIndirectnessImprecisionOther considerationsFondaparinuxControlRelative(95% CI)Absolute(95% CI) VTE 17non-randomised studiesnot seriousnot seriousnot seriousnot seriouspublication bias strongly suspected^a^258/8413 (3.1%)653/21,471 (3.0%) OR 0.43 (0.31 to 0.61) 17 fewer per 1000 (from 21 fewer to 12 fewer)⨁⨁⨁◯Moderate^a^CRITICAL Distal DVT 10randomised trialsnot seriousnot seriousnot seriousnot seriouspublication bias strongly suspected^a^176/3192 (5.5%)357/3035 (11.8%) OR 0.43 (0.30 to 0.61) 63 fewer per 1000 (from 79 fewer to 42 fewer)⨁⨁⨁⨁High^a^CRITICAL Proximal DVT 10randomised trialsnot seriousnot seriousnot seriousnot seriouspublication bias strongly suspected^a^36/3262 (1.1%)115/3106 (3.7%) OR 0.33 (0.15 to 0.75) 24 fewer per 1000 (from 31 fewer to 9 fewer)⨁⨁⨁◯Moderate^a^CRITICAL Non-fatal PE 12non-randomised studiesnot seriousserious^b^not seriousnot seriouspublication bias strongly suspected^a^48/8993 (0.5%)172/22,095 (0.8%) OR 1.04 (0.55 to 1.97) 0 fewer per 1000 (from 3 fewer to 7 more)⨁◯◯◯Very low^a, b^CRITICAL Fatal Bleeding 7randomised trialsnot seriousnot seriousnot seriousserious^c^none0/3561 (0.0%)1/3572 (0.0%) OR 0.34 (0.01 to 8.29) 0 fewer per 1000 (from 0 fewer to 2 more)⨁⨁⨁◯Moderate^c^CRITICAL(a) Suspicion of publication bias when visualizing funnel plots; (b) Results show wide variability or unexplained heterogeneity; (c) Wide confidence intervals; CI. confidence interval; OR. odds ratio
Discussion
According to the present meta-analysis, fondaparinux reduced VTE in individuals undergoing THA and those with hip fractures more effectively than LMWH. Remarkably, fondaparinux continuously demonstrated higher effectiveness in lowering proximal and distal DVT. This effect, which was particularly noticeable in cases of hip fractures, was seen in patients having hip fracture surgery as well as those getting elective THA. The risk of clinically severe bleeding events did not differ significantly. In addition, fondaparinux was less expensive per patient than enoxaparin for thromboembolic events.
The physiological justification for the efficacy of Fondaparinux, a selective inhibitor of Factor Xa, a crucial participant in the coagulation cascade, is provided by its mode of action [35]. The synthetic pentasaccharide fondaparinux binds specifically to antithrombin III, boosting its activity to inhibit just Factor Xa rather than thrombin (Factor IIa), which is different from how heparins work [36]. This selective action allows for more precise and effective coagulation inhibition by reducing thrombus formation without significantly altering bleeding time.
Notable characteristics of fondaparinux’s synthetic chemical composition include a quick onset of action, a lengthy half-life, direct renal excretion and 100% bioavailability when administered subcutaneously [35].
In our study, when only studies that conducted venography were assessed, fondaparinux showed a significantly lower risk of VTE, with a risk ratio of 0.30 (0.17–0.54) compared to enoxaparin. In contrast, when compared with studies that used ultrasound to evaluate VTE, fondaparinux showed a reduced risk of VTE but to a lesser extent compared to enoxaparin, with a risk ratio of 0.55 (0.30–1.01). This may indicate that when more precise diagnostic tests are used, fondaparinux demonstrates a greater reduction in VTE risk. This suggests that the diagnostic methodology could influence the results. This is logical since venography is the standard in diagnosing DVT [37, 38].
On the other hand, when evaluating the influence of the timing of evaluation, it did not appear to affect the results. Although most diagnostic tests were conducted between the 5th and 11th day.
In our study, potential confounding factors were analyzed to assess whether they were balanced between the experimental and control groups. For example, it has been observed that patients with a higher BMI are at greater risk of VTE [39]. In our study, no differences in BMI were observed between the control and experimental groups. Similarly, other parameters that have been shown to increase the risk of thromboembolism, such as increased intraoperative bleeding, surgery duration, or renal function [40–42], showed no differences between the two groups, indicating that both started from a similar baseline. Additionally, other factors such as gender and age, which have also been shown to influence thromboembolism, with it being more common in men and older individuals, were evenly distributed across both groups. There were also no differences in the duration of treatment between groups.
Despite its potent anticoagulant activity, fondaparinux maintains a safety profile comparable to that of low molecular weight heparins, due to its selectivity which reduces the risk of hemorrhagic complications. Previous studies have identified several factors that increase the risk of bleeding with fondaparinux, including male gender and low body weight [43]. Specifically, a body weight under 50 kg and moderate renal insufficiency can increase drug exposure, thereby elevating the risk of bleeding [44]. On the contrary, the involvement of an orthogeriatrician has been shown to improve discharge optimization in patients with hip fractures, resulting in better hemoglobin levels at discharge [45].
In these studies, patient comfort or satisfaction with the different options was not analyzed due to the lack of studies reporting these outcomes. Generally, fondaparinux is seen as easier to manage by the patient because it is administered at a fixed dose, does not require monitoring, and reduces the incidence of subcutaneous hemorrhage [36].
Wang et al. observed that subcutaneous ecchymosis was 3.3% on the seventh day in the fondaparinux group compared to 20.0% in the LMWH group, reaching significant differences [11]. Additionally, the circumference of swelling was also significantly smaller. Wang et al. also observed less pain on the seventh day, assessed using the VAS scale in the fondaparinux group, with no differences found on the third and fifth days.
Another important aspect to consider is treatment compliance. In a recent study [46], 73% of patients treated with fondaparinux showed a preference for the subcutaneous route of administration. On the other hand, approximately 85% of patients who received new oral anticoagulants—which have also demonstrated favorable outcomes in total hip arthroplasty—preferred this form of administration [47]. Furthermore, a high level of treatment compliance was observed, reaching 99% across all groups, regardless of the route of administration used.
The lower cost of fondaparinux as compared to enoxaparin, may be explained by the effectiveness of reducing thromboembolic events, which can minimize the costs of treating these consequences [48]. In particular, the fondaparinux group spent an average of 132 euros per patient per VTE/DVT event in THA at 90 days, while enoxaparin cost 216 euros. The average cost per patient for a VTE/DVT event in the case of a hip fracture at 30 days was 576. Additionally, the cost per patient for a VTE/DVT incident at 90 days after a hip fracture was 339 (euros/dollars), while the cost for enoxaparin was 518. The extended hospital stays, and increased resource usage may help to explain this.
It is essential to consider any potential interactions or confounding factors pertaining to the antithrombotic under analysis that might have impacted the outcomes in addition to the previously mentioned factors. The effectiveness and safety of thromboprophylaxis can be impacted by a variety of drugs, nutraceuticals, and diets, including fondaparinux and LMWHs [49].
Compared to LMWHs and other anticoagulants, fondaparinux, exhibits fewer medication interactions. However, the risk of bleeding is also increased by concurrent use of other medications that influence hemostasis, such as nonsteroidal anti-inflammatory drugs (NSAIDs), especially when these medications are taken with platelet inhibitors (e.g., clopidogrel, aspirin) [50].
The risk of bleeding during LMWH medication may be substantially increased by concurrent use of NSAIDs, SSRIs, and SNRIs [51].
Several differences were found between our study’s results and those of other meta-analyses on the subject. For example, Hur et al. discovered fondaparinux was linked to a greater risk of bleeding than LMWH after examining just four studies [13]. On the other hand, our meta-analysis found no significant differences between the groups and differentiated between small and extensive bleeding. Li et al. also noted that fondaparinux enhanced the risk of hemorrhage [52]. Turpie et al. presented the idea of clinically meaningful bleeding in another meta-analysis [53], however they found no distinction between fondaparinux and enoxaparin. Huang et al. reached to the conclusion that fondaparinux was superior to LMWH in lowering VTE; however, their research was constrained because it only examined THA without examining hip fractures and neglected to take into consideration all of the variables [14], we thought of in order to control for heterogeneity. Only two fondaparinux trials were included in the most current meta-analysis, which was carried out by Migliorini et al. in 2024 [47]. Our results, which also included cost analysis after prophylaxis in hip fracture surgery, are consistent with a meta-analysis of cost analysis studies conducted by Dranitsaris et al., which found fondaparinux to be more cost-effective than enoxaparin in antithrombotic prophylaxis following THA and TKA [54]. These fondaparinux results align with other indications, such total knee replacement [55].
Most studies utilized the approved dosage of 2.5 mg as stable and recommended by the European Medicines Agency (EMA) [56]. For patients with moderate renal impairment, the dose should be reduced to 1.5 mg once daily [57].
Limitations
This study has several limitations. The research encompassed a variety of study designs, both randomized and non-randomized. Additionally, the small number of studies within certain subgroups curtailed the robustness of sensitivity analyses and the ability to achieve consistent results across different settings and populations. The inability to perform meta-regression to adjust for confounding variables or external influences further limited the interpretability of the data. The original studies did not assess whether a tourniquet was used during THA [58]. The assessment of publication bias relied solely on visual inspection of funnel plots due to software constraints (Review Manager 5.4.1), which does not support statistical tests like Egger’s regression. A significant limitation across the studies was the uniform use of a 2.5 mg dose, which is the standard recommended dosage but restricted the assessment of the efficacy and safety of alternative dosing regimens. This uniformity in dosing precludes any analysis on dose-response relationships that could be crucial for optimizing treatment protocols. Information gaps regarding clinically significant bleeding outcomes were also evident; many studies did not sufficiently report how bleeding events impacted patient health or the timing of these events, which are critical for understanding the risk profile of the treatment. Other clinically relevant variables such as pain from injections or specific analytical values were rarely assessed or reported inconsistently, making it difficult to compare these factors statistically across studies. Cost assessments were particularly challenging due to the lack of dispersion data in the studies, forcing reliance on estimation models or Cochrane rules for approximations. Some studies did not specify the total number of participants at the point when variables were measured, necessitating the use of initial participant totals for calculations. Additionally, there was a lack of specified follow-up periods, which is crucial when assessing the timing and impact of certain events. Most studies have focused on fractures, including various types of treatments, ranging from intramedullary nail fixation to prostheses, and the results were not divided. This lack of division in the results could introduce heterogeneity into the interpretation of the findings. Finally, there was a lack of comparative evidence between new oral anticoagulants and fondaparinux.
Conclusion
Based on the results from this meta-analysis, fondaparinux significantly reduces the incidence of venous VTE and distal DVT, compared to controls and LMWHs in patients undergoing elective THA and hip fracture surgery. Fondaparinux maintains a safety profile comparable to enoxaparin, with no significant differences in clinically significant bleeding. Additionally, fondaparinux is more cost-effective, presenting lower average costs per thromboembolic event per patient than enoxaparin. These findings support the use of fondaparinux as a well-tolerated, effective, and economically advantageous alternative for thromboprophylaxis in hip surgery.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
Supplementary Material 5
Supplementary Material 6
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. Wiley; 2019.10.1002/14651858.ED 000142 PMC 1028425131643080 · doi ↗ · pubmed ↗
- 2Turpie AG, Bauer KA, Eriksson BI, Lassen MR, PENTATHALON 2000 Study Steering Committee. Postoperative fondaparinux versus postoperative enoxaparin for prevention of venous thromboembolism after elective hip-replacement surgery: a randomised double-blind trial. Lancet. 2002;359(9319):1721-6. 10.1016/S 0140-6736(02)08648-8. Erratum in: Lancet 2002;360(9339):1102.10.1016/S 0140-6736(02)08648-812049860 · doi ↗ · pubmed ↗
- 3Fuji T, Fujita S, Ochi T. Fondaparinux prevents venous thromboembolism after joint replacement surgery in Japanese patients. Int Orthop. 2008;32(4):443– 51. 10.1007/s 00264-007-0360-7. Epub 2007 Apr 28. PMID: 17468868.10.1007/s 00264-007-0360-7PMC 253227517468868 · doi ↗ · pubmed ↗
- 4Okada Y, Endo H, Mitani S, Fujiwara K, Tetsunaga T, Kagawa Y et al. Venous thromboembolism after total hip arthroplasty diagnosed by enhanced computed tomography:comparison of selective thromboprophylaxis and no thromboprophylaxis. Acta Med Okayama. 2015;69(4):205– 12. doi: 10.18926/AMO/53556. Erratum in: Acta Med Okayama. 2015;69(5):325. 10.18926/AMO/5368010.18926/AMO/5355626289911 · doi ↗ · pubmed ↗
- 5Sullivan SD, Kwong L, Nutescu E. Cost-effectiveness of Fondaparinux compared with Enoxaparin as prophylaxis against venous thromboembolism in patients undergoing hip fracture surgery. Value Health 2006 Mar-Apr;9(2):68–76. 10.1111/j.1524-4733.2006.00085.x 10.1111/j.1524-4733.2006.00085.x 16626410 · doi ↗ · pubmed ↗
- 6Hirsh J, Bauer KA, Donati MB, Gould M, Samama MM, Weitz JI. Parenteral anticoagulants: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):141S-159S. 10.1378/chest.08-0689. Erratum in: Chest. 2008;134(2):473.10.1378/chest.08-068918574264 · doi ↗ · pubmed ↗
- 7Arixtra. Fondaparinux sodium. Summary of Product Characteristics. European Medicines Agency. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/arixtra#product-details