An elevated lipoprotein (a) level, rapid progression, and accumulation of lipidic plaque contents in a deferred coronary artery lesion despite lipid-lowering therapy
Tomomi Watanabe, Yu Kataoka, Aya Katasako, Teruo Noguchi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
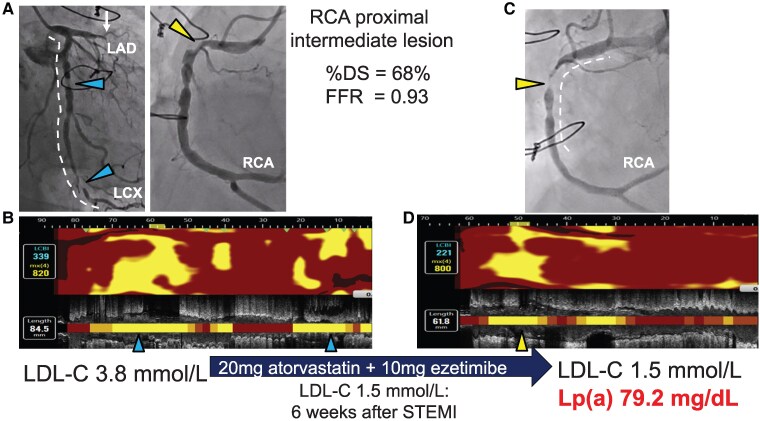 Figure 1
Figure 1- —Nakatani Foundation Research10.13039/501100008884
- —Taiju Life Social Welfare Foundation Research Grant10.13039/100016289
- —Terumo Life Science Foundation Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLipoproteins and Cardiovascular Health · Coronary Interventions and Diagnostics · Aortic Thrombus and Embolism
Case description
A 79-year-old male was hospitalized due to an abnormal ECG and akinesis in the anterior region on echocardiography. He had prolonged chest pain 2 weeks prior to hospitalization, which suggested ST-segment-elevation myocardial infarction (STEMI) 2 weeks previously. Coronary angiography revealed occlusion of left anterior descending, accompanied by two severe stenoses of left circumflex (LCX) artery and an intermediate stenosis at the proximal segment of right coronary artery (RCA) (see Supplementary material 8 online, Movies SI and SII). ECG and echocardiography suggested a non-viable myocardium in the anterior region, and wire-based fractional flow reserve (FFR) (Optowire, Zeon Medical, Japan) for an intermediate stenosis of the RCA was 0.93. Any intravascular imaging was not conducted to evaluate plaque features at this intermediate stenosis. Therefore, percutaneous coronary intervention (PCI) was performed on the LCX artery. Near-infrared spectroscopy (NIRS) imaging (Dualpro^TM^, Infraredx, Bedford, MA, USA) revealed extensive lipidic plaque materials [maximum lipid-core burden index (LCBI_4mm_) = 820] (Figure 1, Supplementary material 8 online, Movie SIII). Following completion of PCI, 20 mg atorvastatin and 10 mg ezetimibe were initiated, and LDL-cholesterol (LDL-C) level decreased to 1.6 mmol/L (58% reduction). Lipoprotein (a) (Lp[a]) level was not measured during initial hospitalization, whereas on-treatment LDL-C level was 1.5 mmol/L, 6 weeks post-hospitalization. However, he was re-hospitalized due to NSTEMI 6 months post-PCI (on-treatment LDL-C = 1.5 mmol/L). Coronary angiography revealed rapid progression of non-critical stenosis at the proximal segment of the RCA, which had an FFR ≥0.91 6 months previously (Figure 1, Supplementary material 8 online, Movies SIV and SV). NIRS imaging revealed substantial lipidic plaque materials at this lesion despite achieving LDL-C < 1.8 mmol/L (maxLCBI_4mm_ = 800) (Figure 1, Supplementary material 8 online, Movie SVI). Furthermore, he had an elevated Lp(a) level (79.2 mg/dL).
Rapid disease progression at deferred coronary artery lesions. Coronary angiography on 1st admission due to ST-segment-elevation myocardial infarction. The left anterior descending artery was occluded (white arrow). Two severe stenoses (blue triangles) in the left circumflex artery and one intermediate stenosis (yellow triangle) in the right coronary artery are also observed. Fractional flow reserve for the right coronary artery was 0.93. The white dotted line represents the image segment obtained using Near-infrared spectroscopy. The blue triangles correspond to those in (B). (A) Near-infrared spectroscopy chemogram within the left circumflex artery prior to percutaneous coronary intervention. Extensive lipid materials were present with a maxLCBI4mm of 820. The LDL-cholesterol level was 3.9 mmol/L. Following the completion of percutaneous coronary intervention, 20 mg atorvastatin and 10 mg ezetimibe were initiated, and the LDL-cholesterol level decreased to 1.6 mmol/L (58% reduction). (C) Coronary angiography at 6 months post-percutaneous coronary intervention. The deferred lesion in the right coronary artery has rapidly progressed (yellow triangle) and caused NSTEMI. The white dotted line represents the image segment obtained using Near-infrared spectroscopy. The yellow triangle corresponds to that shown in (D). (D) Near-infrared spectroscopy chemogram within the right coronary artery prior to the percutaneous coronary intervention. Despite lipid-lowering therapy (LDL-cholesterol, 1.5 mmol/L), there were substantial lipidic plaque materials in theright coronary artery. In addition, the Lp(a) level was 79.2 mg/dL. FFR, fractional flow reserve, LAD, left anterior descending artery, LCX, left circumflex artery, LDL-C, low-density lipoprotein cholesterol, Lp(a), lipoprotein (a), NSTEMI, non-ST-segment elevation myocardial infarction, PCI, percutaneous coronary intervention, RCA, right coronary artery, STEMI, ST-segment elevation myocardial infarction.
Recent observational studies reported very low event rates at lesions with an FFR ≥0.91.^1^ In our case, despite non-critical feature of stenosis at the proximal segment of the RCA, an accelerated progression with ongoing accumulation of lipid was observed during lipid-lowering therapy. Given the pro-atherogenic properties of Lp(a),^2^ the residual elevated Lp(a) level may require additional novel therapies for STEMI.
Supplementary Material
ytaf255_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kuramitsu S, Matsuo H, Shinozaki T, Horie K, Takashima H, Terai H, et al Two-year outcomes after deferral of revascularization based on fractional flow reserve: the J-CONFIRM registry. Circ Cardiovasc Interv 2020;13:e 008355.31884834 10.1161/CIRCINTERVENTIONS.119.008355 · doi ↗ · pubmed ↗
- 2Kronenberg F, Mora S, Stroes ESG, Ference BA, Arsenault BJ, Berglund L, et al Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European atherosclerosis society consensus statement. Eur Heart J 2022;43:3925–3946.36036785 10.1093/eurheartj/ehac 361PMC 9639807 · doi ↗ · pubmed ↗