Postdischarge Care of Acute Kidney Injury Survivors: An Opportunity for Targeted Nurse and Pharmacist Interventions
Melanie M. Manis, Jessica L. Wallace, Emily F. Boyd, Kaleab Z. Abebe, Linda Fried, Paul M. Palevsky, Paul T. Conway, Edward J. Horwitz, Kathleen D. Liu, Chirag R. Parikh, Emilio Poggio, Edward D. Siew, Javier A. Neyra, Matthew R. Weir, F. Perry Wilson, Sandra L. Kane-Gill

TL;DR
This paper discusses how nurses and pharmacists can improve post-discharge care for patients who have recovered from acute kidney injury.
Contribution
The paper highlights the roles of nurses and pharmacists in providing structured postdischarge care to AKI survivors.
Findings
Post-discharge follow-up within 90 days of AKI is recommended to promote kidney recovery.
Timely and coordinated postdischarge care is often lacking, leading to missed opportunities for preventing complications.
Interdisciplinary collaboration involving nurses and pharmacists is essential for effective post-AKI care.
Abstract
The incidence of acute kidney injury (AKI) is increasing, and with it, the population of individuals requiring post-AKI care. Post-discharge follow-up for AKI survivors is recommended within 90 days of an AKI episode to promote kidney recovery and potentially prevent progression of kidney disease. However, timely postdischarge care is often lacking or fragmented and poses a missed opportunity to prevent long-term complications of this condition. Suggested elements of follow-up care begin with a scheduled appointment with a physician and involve a bundled approach to care with health care providers’ communicating across sites, remote patient monitoring devices, review of medications, education, access, kidney care evaluation, and interdisciplinary collaboration to achieve these patient care goals. This article provides an overview of guidance documents for post-AKI care and the roles of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
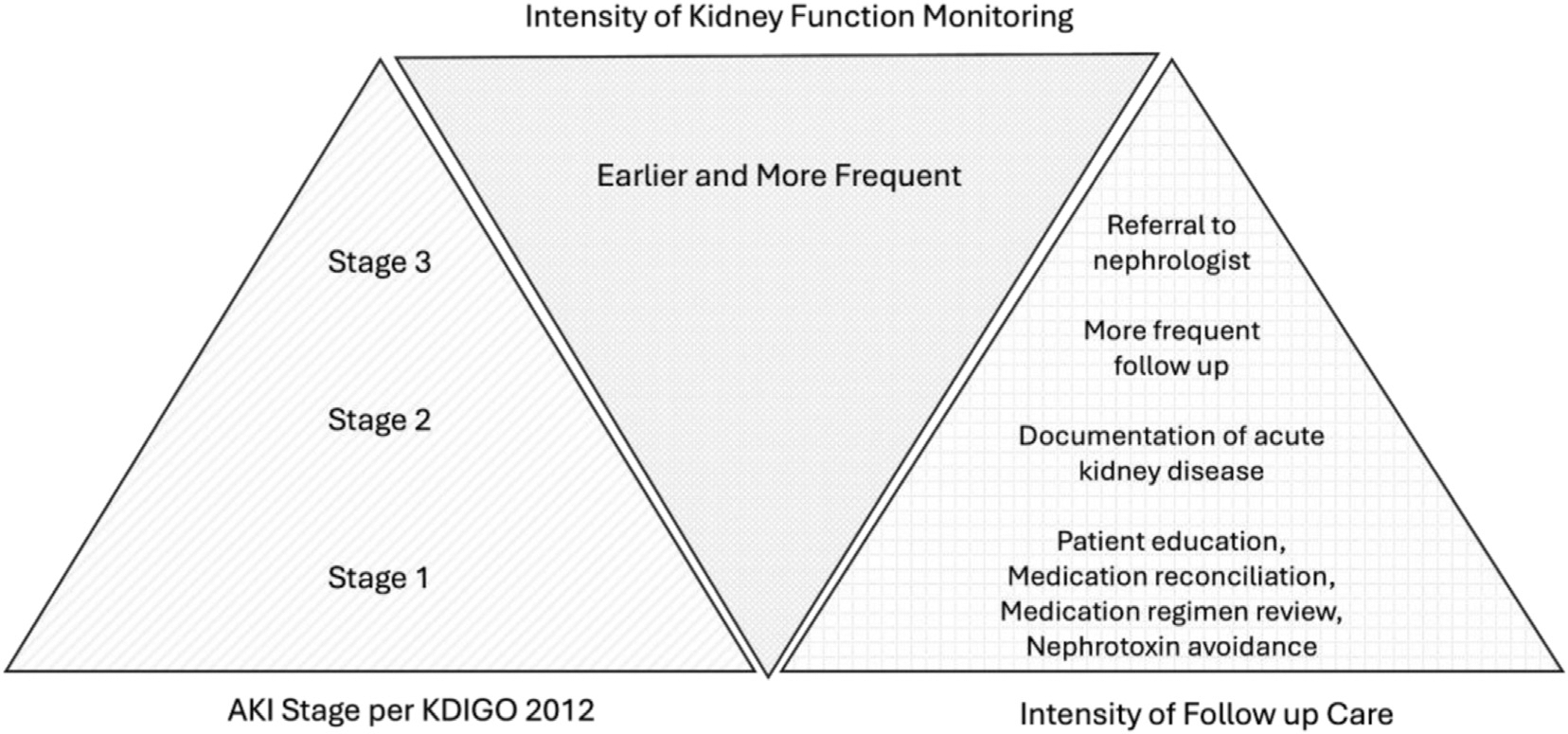 Figure 1
Figure 1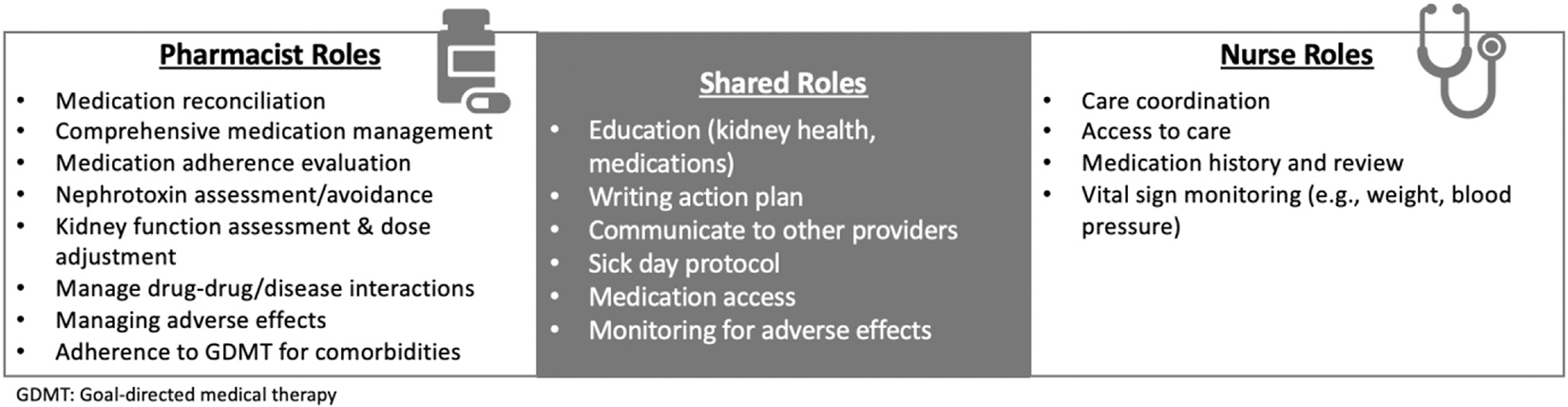 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmaceutical Practices and Patient Outcomes · Acute Kidney Injury Research · Dialysis and Renal Disease Management
Acute kidney injury (AKI) occurs in 15–20% of hospitalized patients. Notably, the incidence of AKI is increasing and thus the need for post-AKI care.^1,2^ Patients with AKI are at risk of developing recurrent AKI, acute kidney disease (AKD), chronic kidney disease (CKD), and end-stage kidney disease requiring dialysis, cardiovascular disease, and debilitation with poor health-related quality of life following a prolonged hospitalization with need for acute rehabilitation.^3^ Each year approximately 1.6 million Americans progress from AKI to CKD.^4^ Even those patients with an apparent reversible AKI prior to hospital discharge have a significant risk of developing de novo CKD.^5^ The transition to CKD can include AKD, as AKD is a decline in kidney function lasting for less than or equal to 3 months.^6^ Six months after a drug-associated AKI event, kidney damage persists in 70% of cases.^7^ Exposure to one or more potentially nephrotoxic drugs presents an increased risk of developing de novo or progressive CKD for AKI survivors.^8^ Timely, postdischarge care after an episode of AKI could curtail worsening kidney health and unnecessary burdens on patients, caregivers, and the overall health care system.
It is unfortunate that post-AKI care is poor given the substantial negative consequences. In Medicare patients, only 13% saw a nephrologist within 90 days after an AKI episode.^3,9^ Additionally, many individuals with AKI were not aware they had the condition, making it less likely that they would seek follow-up.^10–14^ The lack of postdischarge AKI care is considered a missed opportunity to prevent chronic disease and complications.^15^ Evidence-based best practices for postdischarge care after an inpatient AKI event are unknown.
The reasons AKI survivors do not seek care, in addition to their lack of knowledge about kidney disease, include the feeling of hospital-related fatigue, a concern for adding more doctors to their care team, and the travel time to receive in-person care.^16^ Other individuals have challenges because post-AKI care co-ordination is lacking.^17^ These are opportunities for a nurse to provide supportive care, help with medical access, education, and coordinate AKI survivors’ follow-up care with the goal of improving patient outcomes.
Almost 5 million ambulatory care visits occur every year due to adverse drug events, and often these are associated with preventable medication errors.^18^ Complex medication regimens that require dose adjustments or drug discontinuation in the presence of reduced kidney function is a risk for medication errors in post-AKI survivors. A lack of an accountable clinician at hospital discharge to manage drug-related issues during transition of care is cited as a possible reason for missed medication errors.^19^ Patient-pharmacist interactions to enhance medication access, safety, and monitoring are well established. It is expected that AKI survivors are a vulnerable population that could benefit from pharmacist oversight during transitional care.^20,21^
This article provides an overview of the guidance documents for post-AKI care and the potential roles of the nurse and pharmacist as part of an interdisciplinary team in postdischarge care after a patient experiences an episode of AKI.
OPINION-BASED GUIDANCE DOCUMENTS FOR POST-AKI/AKD CARE AND OPPORTUNITIES FOR NURSE AND PHARMACIST INTERVENTIONS
Despite the importance of post-AKI care, recommendations and supporting evidence are sparse. The 2012 KDIGO guidelines suggest an evaluation “within 3 months to assess for resolution, new-onset, or worsening of pre-existing CKD.”^22^ Since 2012, several groups have recognized the lack of data on supportive patient care and have aimed to improve postdischarge AKI care processes by proposing bundled frameworks and quality indicators to drive future research. The bundled frameworks are summarized in Table 1 and highlight the potential role for nurse and pharmacist interventions in the care process.^23–27^
In 2017, the Acute Disease Quality Initiative (ADQI) consensus statement providing practice guidance for AKD management and renal recovery was released.^23^ In response to the lack of data for timing, frequency, and methods of evaluating kidney function following an episode of AKI, the group proposed a “layered” approach for follow-up with intensity of care based on the severity of kidney dysfunction and the risk of morbidity and mortality (Fig 1). Specific suggestions for drug management in patients with AKD were also provided supporting pharmacists’ involvement in the care of patients with AKD.
In 2019, ADQI published Quality Improvement Goals for AKI. The authors proposed key elements of an appropriate post-AKI/AKD Care Bundle that included components of KAMPS: kidney function assessment-advocacy-medications-pressure-sick day protocols for patients with AKI and WATCH-ME: weight assessment-access-teaching-clearance medication-hypotension for patients with AKI who require dialysis.^24^ The authors acknowledged the need for future research focused on optimal management strategies for each facet of the KAMPS/WATCH-ME bundles and the need for validation of the bundles. Notably, this is the only post-AKI/AKD care bundle that includes sick day protocols. A scoping review of 74 sick day medication guidance documents indicates consensus on how to apply this guidance is lacking, so inclusion in post-AKI care is questionable.^25^ Still, many aspects of KAMPS/WATCH-ME would benefit from nurses’ and pharmacists’ participation to facilitate implementation.
The Optimum Care of AKI Survivors Not Requiring Dialysis after Discharge Report released in January 2024 by the American Society of Nephrology AKINow Recovery workgroup discussed the challenges and opportunities for post-AKI care.^26^ This report emphasized 6 domains: transitional care, education, collaborative care delivery, evidence and guidance for diagnostic and therapeutic interventions, and digital health applications. Ultimately, similar suggestions were made by AKINOW and previous guidance documents indicating that more research is needed to drive patient-centered, evidence-based care for AKI survivors. Interestingly, 5 and 8 of the 12 AKINow recommendations are prospects for nurses’ and pharmacists’ contributions, respectively. The AKINow Recovery workgroup is currently working on tools to assist in care continuity at the time of hospital discharge.
POTENTIAL ROLES FOR A NURSE NAVIGATOR IN POSTDISCHARGE AKI CARE
Postdischarge Care by Nurses
The nurse’s role in a transitional care capacity has been termed “nurse case manager,” “transition coach,” “nurse liaison,” and “nurse navigator.” This role of the nurse first originated in oncology to help bridge the care gap with the nurse serving as the main point of contact through the patient’s care trajectory, leading the coordination of care, and providing education to help patients throughout their health care journey.^28,29^ Nurses have demonstrated to be a beneficial member of an interdisciplinary team providing postdischarge care co-ordination in various other conditions. In a general population of hospitalized patients, a randomized trial demonstrated the value of a nurse “transition coach” to provide postdischarge care support including home visits and telephone calls to reduce hospital readmissions at 30 days (8.3 vs 11.9, P =.048) and 90 days (16.7 vs 22.5, P =.04). The 4 components of the intervention included (1) patient’s self-management of medications; (2) timely postdischarge follow-up; (3) self-monitoring of “red flags” and at-home response, and (4) patient-maintained medical record to aid in transitions of care.^30^ This intervention is easily translated to the AKI survivor population. Further, postdischarge transitional care nursing models are well described in heart failure patients, who are at high risk for readmission and could also be applied to AKI survivors.^31^
Postdischarge AKI Care by Nurses
AKI survivors face similar risk of rehospitalization with complexity of multimorbidity, often including concomitant heart failure, and prolonged hospitalizations, which warrant a nurse dedicated to coordinating care following discharge to arrange for critical follow-up visits given the coexistence of often both cardiac and renal complications of hospitalization and need for close monitoring of this dynamic patient. Beyond care coordination, education is also an essential role of the nurse. With 80% of patients estimated to be unaware of AKI diagnosis at time of hospital discharge, education by the nurse and continual reinforcement of that education is invaluable to promote kidney health.^11^ The role of the nurse as part of the interdisciplinary care team for AKI survivors supports nurses as the key educators at discharge utilizing a variety of educational resources (eg, video on AKI, verbal discussion, written materials) with standardized teach-back questions to verify understanding.^32^ Important components of AKI education identified by the nurses in this study included the potential for recovery and risk of reinjury. Furthermore, nurses may be used in the clinic setting postdischarge. In an interdisciplinary educational study of postdischarge AKI clinic patients, nurses engaged in a 10–15-minute educational interaction at the first clinic visit to identify what was unknown by the patient about AKI using open-ended questions and self-reflection of the hospital experience.^33^ The nurse answered questions and concerns and provided an AKI educational handout available from the National Kidney Foundation. The patient-nurse interaction was followed by patient interactions with the pharmacist and a physician. This was the first study to evaluate an educational effort by the interdisciplinary team and reported a significant improvement in patients’ self-perceived knowledge.
The next vital role of the nurse is close objective monitoring of blood pressure and body weight for volume management, which is an important component of care for AKI survivors. Often antihypertensives and/or diuretics are held or dose adjusted during hospitalization, making close monitoring necessary to avoid complications. Remote monitoring of vital signs by nurses in postdischarge AKI care has been described in the literature and may offer improved access to monitoring care.^34^ In a general patient population with various health conditions including most commonly COVID-19, heart failure, or hypertension, a nurse-led remote patient monitoring program allowed for improved connection with patients and access to care, resulting in a lower 30-day, all-cause hospitalization rate (13.7% vs 18.0%, P = 0.01), and high patient satisfaction.^35^ Beyond hospitalization rates and satisfaction, outcomes such as improved blood pressure control have been observed in the literature with remote monitoring programs implemented amidst the COVID-19 pandemic involving a multidisciplinary care team including nurse practitioners.^36^ AKI survivors could highly benefit from the application of this nurse-led remote monitoring care model given the need for ongoing assessment of blood pressure and weights.
When the nurse’s role on the interdisciplinary care team for post-AKI care is described in the literature, the role of the nurse is focused on a single role such as education or care co-ordination.^33,34,37^ Literature describing a comprehensive, multifaceted role of the nurse in postdischarge AKI care is limited. In a nonrandomized study of stage 2–3 AKI survivors after hospital discharge, Singh and colleagues outlined an AKI rehabilitation program that featured a nurse performing multiple different roles, which was associated with a reduced risk of mortality or rehospitalization at 30 days (odds ratio, 0.41; 95% confidence interval, 0.16–0.93) and 90 days (odds ratio, 0.52; 95% confidence interval, 0.25–1.05).^38^ In conclusion, nurses are crucial members of the care team to aid in providing postdischarge AKI care, with opportunities to enhance outcomes through roles such as care coordination, patient education, and monitoring. However, further pragmatic studies are needed to prospectively assess the impact of nurses’ contributions in AKI survivors.
POTENTIAL ROLES FOR A PHARMACIST IN POSTDISCHARGE AKI CARE
Postdischarge Care by Pharmacists
Pharmacists are widely engaged in transitional care of patients when resources are available to do so. A central activity is conducting medication reconciliation to identify discrepancies between hospital discharge prescriptions and a patient’s prehospital medications, thus preventing medication errors and adverse drug events. Transitional care pharmacists also educate patients and caregivers about proper medication use, side effects, lifestyle changes, and medication adherence and empower patients to manage their health independently. Studies have demonstrated that pharmacist-led interventions can reduce medication errors by at least 37%, decrease 30-day readmission rates by up to 20%, and improve disease management in conditions like heart failure, asthma, and diabetes.^39–42^ In patients with kidney injury, pharmacists’ involvement in transitional care is especially relevant given the complex medication challenges in this patient population.
Postdischarge AKI Care by Pharmacists
Pharmacists are the medication experts of the interdisciplinary care team with advanced pharmacokinetic knowledge including drug elimination and its impact on dosing in kidney dysfunction, as well as mechanisms of nephrotoxicity and management. Beyond kidney health considerations, pharmacists are trained to provide comprehensive medication management (CMM), patient education, and communication hand-off to other health care providers.^43^
Several studies have demonstrated the value of a pharmacist as part of the interdisciplinary team when providing postdischarge care.^44,45^ In an end-stage kidney disease Seamless Care Organization, pharmacists participated in an interdisciplinary medication therapy management intervention that identified 5466 medication therapy problems and reduced hospital readmissions (P < 0.001). In this intervention, the nurse provided an initial medication reconciliation while the pharmacist conducted a secondary medication review and created an action plan that was communicated to the nephrologist.^45^ Pharmacists have had a positive impact on clinical outcomes including readmission rates and death at 90 days and medication safety in other disease states, leading to the recognition of clinical pharmacists as an integral part of the patient care team by several organizations including the American Heart Association/American College of Cardiology/Heart Failure Society of America, the American Diabetes Association, the Society of Critical Care Medicine, and the Organ Procurement and Transplantation Network.^33,46–49^
AKI survivors are recognized as an ideal patient population that would benefit from pharmacists’ hypervigilance due to nuances in complex medication management as stated above.^50^ Nephrologists and primary care physicians requested clinical pharmacists’ engagement in medication management when caring for AKI survivors to overcome barriers in medication mismanagement and to provide medication-related guideline adherence.^51^ The ADQI Quality Improvement Goals for AKI recommend that pharmacists be included as a member of the dedicated interdisciplinary team and that pharmacists perform medication reconciliations, reviews, and management as part of the post-AKI/AKD kidney health bundle.^24^ Additional support for an elevated role of pharmacists on kidney interdisciplinary care teams and within national kidney care models, along with CMM for people with kidney disease, has gained support of kidney professionals and patients through the broad-based Optimizing Kidney Health through Optimal Medical Management collaborative and growing interest from the Centers for Medicare and Medicaid Services.^52^
Unfortunately, the specific role of the pharmacist in providing postdischarge AKI care is difficult to elucidate, as they are often embedded in care teams where members’ activities target a variety of outcomes and key details are often missing or not fully described. But pharmacist-centric studies are being investigated, so we may have a clearer assessment in the future.^53^ A proposal for the role of a pharmacist caring for patients with AKD was published in 2017 and included enhancing health literacy about medication management, managing drug-drug interactions, avoiding or cautiously restarting nephrotoxins post-AKI, encouraging monitoring of kidney function, and managing diabetes and hypertension as part of the care team. Proposed activities occurred during hospitalization, at the time of discharge, and postdischarge and specifically encouraged telemedicine interactions and/or meeting patients in the post-AKI ambulatory clinics.^48^ A recently published scoping review evaluated the role of the pharmacist in providing postdischarge care to patients with AKI and CKD.^54^ Four postdischarge AKI care team models with pharmacists were identified.^33,37,53–56^ Although the role of the pharmacist varied significantly among interdisciplinary care team models, a medication regimen review was consistently performed by a pharmacist. Medication reconciliation and writing action plans were also commonly performed by the pharmacist. Still, it is proposed the pharmacist’s roles should expand beyond medication review and reconciliation to include CMM. Kidney function assessment with drug dosing modifications, education on medications and kidney disease, as well as assistance with medication access and adherence, and finally communication with other health care team members were also proposed.^48^ Figure 2 depicts proposed roles specific to the pharmacist based on their medication expertise.
CHALLENGES FOR NURSES AND PHARMACISTS IN THE ROLE OF AKI SURVIVOR CARE
Widespread use of nurses and pharmacists as part of an interdisciplinary team for AKI survivors’ care requires recognizing these patients as a priority so resources can be dedicated accordingly. In general, postdischarge patient care is important, so giving precedence to AKI survivors requires explicit evidence to support this narrow focus. A comprehensive team dedicated to postdischarge care of AKI survivors seems logical but requires a full understanding of the impact on patient outcomes to garner support. There has been at least one study suggesting a lack of benefit associated with pharmacist involvement in the care of CKD patients after hospitalization, but the intervention was limited to medication reconciliation and not a comprehensive medication review and did not focus on AKI survivors.^57^ Other studies have demonstrated the feasibility and potential for positive outcomes including better blood pressure control, improved urine albumin to creatinine ratio, improved kidney health literacy, and a reduction in 30-day rehospitalization and mortality having a nurse and pharmacist as part of the interdisciplinary team for AKI survivors.^37,38,54,58,59^ Still, other challenges include the shortage of nurses and pharmacists in the workforce to complete these duties and the financial support to secure dedicated positions.
ONGOING RESEARCH: CARING FOR OutPatiEnts AFTER ACUTE KIDNEY INJURY (COPE-AKI)
COPE-AKI is a randomized, prospective trial funded through National Institutes of Health/National Institute of Diabetes & Digestive & Kidney Diseases and seeks to provide evidence for many of the suggestions made in the guidance documents. Directed by AKI patient survivors’ insights, COPE-AKI study collaborators established a care bundle that includes communication/coordination, remote objective monitoring, review of medications, education, access, kidney care evaluation, and interdisciplinary collaboration of a study physician, nurse navigator, and pharmacist (Table 2).^27,60–62^ The nurse serves an integral role as the primary contact with the patients to co-ordinate postdischarge care. The nurse educates on self-monitoring and use of remote monitoring equipment (blood pressure cuff and weight scale). Postdischarge, the nurse navigator monitors the patient’s condition, facilitates scheduling of routine and ad-hoc medical follow-up, facilitates adherence with prescribed medical care and follow-up appointments, provides education, and serves as a resource for AKI-related management, along with ensuring psychosocial support.^27^ The pharmacist also plays an important role by performing a postdischarge telemedicine visit with the patient and completing a medication reconciliation plus a comprehensive medication regimen review. The pharmacist evaluates appropriate drug dosing based on kidney function, nephrotoxic burden, and drug-drug or drug-disease interactions. Education related to kidney injury, medications to avoid, and medication adherence is also provided. The pharmacist also assists with medication access and barriers to care.
Results from this study may help further define the role of the nurse and pharmacist in post-AKI care. This is the first randomized prospective study to include a multifaceted nurse role as part of the interdisciplinary care team for postdischarge AKI care. Pragmatic studies evaluating kidney disease patients are increasing with inclusion of both pharmacists and nurse on the multidisciplinary care team.
SUMMARY
Opportunities to improve care of AKI survivors after hospital discharge include supporting appropriate provider follow-up to ensure CMM and monitoring of kidney function. Postdischarge AKI care by an interdisciplinary team has been proposed to improve outcomes in these individuals. Nurses could play a critical role in care coordination for post-AKI patients to improve medical access along with providing ongoing patient communication to deliver education about kidney health and monitoring of the patient’s condition. AKI survivors often have multimorbidity and complex medication regimens at hospital discharge; pharmacists are essential in performing medication reconciliation, medication regimen reviews, and education. By coordinating care across different settings, interdisciplinary teams ensure smooth transitions of patients and prevent gaps in care that could lead to readmissions. While many guidance documents propose the optimal care of patients with AKI and AKD, further research is needed to evaluate the impact of these care bundles, assess the impact on patient outcomes, determine effective implementation strategies, and inform future policy proposals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Waikar SS, Curhan GC, Wald R, Mc Carthy EP, Chertow GM. Declining mortality in patients with acute renal failure, 1988 to 2002. J Am Soc Nephrol. 2006;17(4):1143–1150.16495376 10.1681/ASN.2005091017 · doi ↗ · pubmed ↗
- 2Swaminathan M, Shaw AD, Phillips-Bute BG, Trends in acute renal failure associated with coronary artery bypass graft surgery in the United States. Crit Care Med. 2007;35(10):2286–2291.17944016 10.1097/01.ccm.0000282079.05994.57 · doi ↗ · pubmed ↗
- 3Silver SA, Siew ED. Follow-up care in acute kidney injury: lost in transition. Adv Chronic Kidney Dis. 2017;24(4):246–252.28778365 10.1053/j.ackd.2017.05.008 · doi ↗ · pubmed ↗
- 4Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. 2012;81(5):442–448.22113526 10.1038/ki.2011.379PMC 3788581 · doi ↗ · pubmed ↗
- 5Bucaloiu ID, Kirchner HL, Norfolk ER, Hartle JE, Perkins RM. Increased risk of death and de novo chronic kidney disease following reversible acute kidney injury. Kidney Int. 2012;81(5):477–485.22157656 10.1038/ki.2011.405 · doi ↗ · pubmed ↗
- 6Levey AS, Eckardt KU, Dorman NM, Nomenclature for kidney function and disease: report of a kidney disease: improving global outcomes (KDIGO) consensus conference. Kidney Int. 2020;97(6):1117–1129.32409237 10.1016/j.kint.2020.02.010 · doi ↗ · pubmed ↗
- 7Menon S, Kirkendall ES, Nguyen H, Goldstein SL. Acute kidney injury associated with high nephrotoxic medication exposure leads to chronic kidney disease after 6 months. J Pediatr. 2014;165(3):522–527.e 2.24928698 10.1016/j.jpeds.2014.04.058 · doi ↗ · pubmed ↗
- 8Schreier DJ, Rule AD, Kashani KB, , ACT Study Team. Nephrotoxin exposure in the 3 Years following hospital discharge predicts development or worsening of chronic kidney disease among acute kidney injury survivors. Am J Nephrol. 2022;53(4):273–281.35294951 10.1159/000522139 PMC 9090945 · doi ↗ · pubmed ↗