The Indian Experience With Nonacog Beta Pegol for the Treatment of Hemophilia B in Children and Adolescents: A Safety and Efficacy Evaluation
Nehal Patel, Ghosha Pandav, Rashmi Thanvi, Priyanka Solanki, Dipti Shah, Anil Katara

TL;DR
This study shows that Nonacog Beta Pegol is a safe and effective treatment for hemophilia B in Indian children and adolescents, significantly reducing bleeding episodes.
Contribution
The study provides real-world evidence from India on the safety and efficacy of low-dose N9-GP prophylaxis for hemophilia B in children and adolescents.
Findings
N9-GP reduced the annualized bleeding rate from 21.1 to 0.42 bleeds/year.
Patients showed significant improvement in joint health and functional independence scores.
No adverse drug reactions or inhibitors were observed during the 12-month treatment period.
Abstract
Purpose: Regular prophylactic factor replacement is recommended as optimal therapy for hemophilia B. Factor concentrate with longer half-lives would allow successful prophylaxis as less frequent dosing would be less burdensome for patients and caregivers. Nonacog Beta Pegol (N9-GP), a glycopegylated factor IX with an extended half-life, has been established globally. However, real-world data from India remain limited. This study evaluates the safety, efficacy, and feasibility of low-dose N9-GP prophylaxis in Indian children/adolescents with hemophilia B. Methods: In this retrospective study, a total of seven patients with hemophilia B were included. Baseline assessments of the annualized bleeding rate (ABR), Functional Independence Score in Hemophilia (FISH), and Hemophilia Joint Health Score (HJHS) were conducted for all patients. Dosing was individualized (mean 34.76 IU/kg; range:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
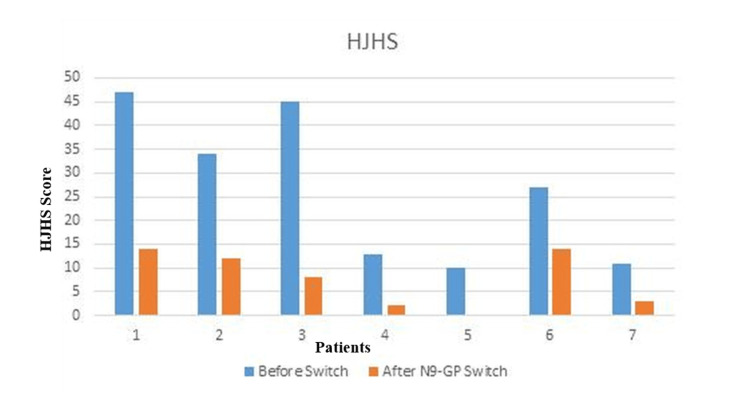 Figure 1
Figure 1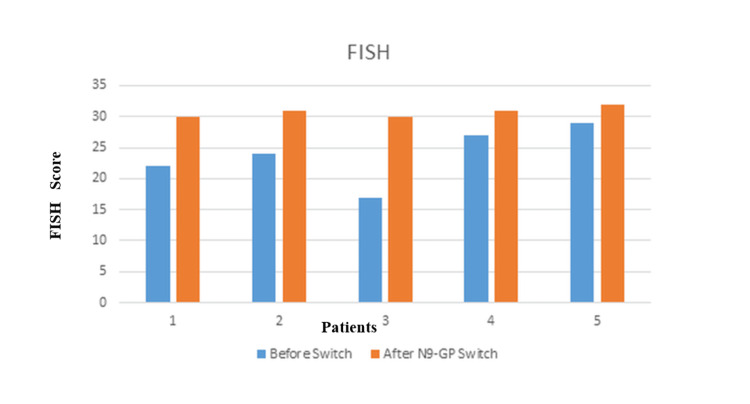 Figure 2
Figure 2| Patients | (SHL) Before prophylaxis IU/KG/year | (EHL) After prophylaxis IU/KG/year |
| Patient 1 | 960 | 561 |
| Patient 2 | 960 | 637 |
| Patient 3 | 1200 | 765 |
| Patient 4 | 960 | 629 |
| Patient 5 | 960 | 425 |
| Patient 6 | 480 | 680 |
| Patient 7 | 400 | 425 |
| Baseline Features | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 |
| Age (Years) | 18 | 17 | 14 | 13 | 9 | 5 | 4 |
| Weight (Kg) | 45 | 61 | 23 | 42 | 40 | 25 | 20 |
| Frequency of dosing (weekly) | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Dose (IU/Kg) | 33.33 | 37.5 | 45 | 37.5 | 25 | 40 | 25 |
| Bleeding sites | Knee joint | Knee joint | Joint bleed, hematuria | Ankle joint | Muscle bleeds | Joint | Muscle, joint |
| Target joints at baseline | One | One | Three | One | One | Two | Zero |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | ||
| Overall ABR | Before | 24 | 24 | 30 | 24 | 24 | 12 | 10 |
| After | 0 | 1 | 0 | 1 | 0 | 1 | 0 | |
| Spontaneous ABR | Before | 24 | 24 | 30 | 24 | 24 | 12 | 10 |
| After | 0 | 1 | 0 | 1 | 0 | 0 | 0 | |
| Traumatic ABR | Before | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| After | 0 | 0 | 0 | 0 | 0 | 1 | 0 | |
| Bleed resolution after 1 or 2 injections. (Y/N) | - | Y | - | Y | - | Y | - | |
| Target joints after N9GP Prophylaxis | 0 | 0 | 1 | 0 | 0 | 0 | 0 | |
| Remaining Bleed free after N9 GP Prophylaxis (Y/N) | Y | N | Y | N | Y | N | Y | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemophilia Treatment and Research · Blood Coagulation and Thrombosis Mechanisms
Introduction
Hemophilia B is a rare genetic disorder, with an estimated incidence of 1 in 30,000 male births. Like hemophilia A, hemophilia B also leads to spontaneous bleeding, particularly in joints, muscles, and internal organs, resulting in pain, disability, and reduced quality of life [1]. Despite advances in treatment, hemophilia management remains a significant challenge, especially in developing countries like India, where access to healthcare limits the treatment options [2].
N9-GP, a recombinant factor IX with glycopegylated modification that prolongs its half-life, is a valuable treatment option for hemophilia B patients. This extended half-life factor can increase the half-life by fivefold compared to the standard factor IX. It has been extensively studied through the PARADIGM clinical trial program, which investigated the safety and efficacy of N9-GP across diverse patient populations for prophylaxis, on-demand treatment, and in perioperative settings, a comprehensive development pathway evaluating its safety, efficacy, and long-term outcomes across diverse patient populations. The trials have demonstrated that N9-GP is effective in preventing bleeding episodes, minimizing joint damage, and significantly improving quality of life for individuals with hemophilia B. Because of the longer half-life of N9-GP, it also offers the benefit of achieving the clinical outcomes, with reduced frequency of injections compared to standard half-life factors [3-8].
According to Annual Global Survey 2020, only 9% and 4% of children and adults with hemophilia were on prophylaxis, respectively [9]. Studies have pointed out a higher degree of disability in patients with hemophilia in India. India is one of the countries with a large number of patients diagnosed with hemophilia in the world, and the majority of these patients are on episodic treatment rather than the standard of care prophylaxis because of resource constraints, leading to increased morbidity and mortality [10].
Against this backdrop, this case series aims to highlight the efficacy and safety of low-dose N9-GP prophylaxis in children and adolescents with hemophilia B. By investigating the use of low-dose N9-GP, we hope to provide a more accessible and affordable treatment option for patients in India and similar resource-constrained settings. Our study will assess the impact of low-dose N9-GP on bleeding frequency, joint health (HJHS), and functional ability (FISH), providing valuable insights into the potential of this treatment approach.
Materials and methods
Study design
This retrospective observational study conducted between 13th August 2021 (first patient first visit) and 23rd May 2023 (last patients last visit) involves seven children and adolescents with severe hemophilia B, who were receiving prophylaxis with standard half-life (SHL) Factor IX, who were switched to extended half-life factor (N9-GP) at baseline, at a tertiary care center in Gujarat. Patient data were retrieved from medical records (MR).
Study population
The study included patients diagnosed with hemophilia B who were aged 18 years or younger and had initiated prophylaxis with N9-GP; written informed consent was obtained from adult participants or from the legal guardians of minor participants. Patients with a history of inhibitors, incomplete medical records, or those who did not provide informed consent were excluded.
Baseline data included the age and weight of the patients, as well as their treatment history. The dose and frequency of injections were documented, with patients receiving N9-GP at a dose of 34.76 IU/kg (range: 25-40 IU/kg) every three weeks for one year. Joint status and bleed status were assessed at baseline, with annualized bleed rates calculated from the number of bleeds in the preceding year. Joint status was evaluated using the Hemophilia Joint Health Score (HJHS) version 2.1, and functional independence was assessed with the Functional Independence Score in Hemophilia (FISH) score, both at baseline and at 12 months after initiation of N9-GP. After 12 months of treatment, data regarding the overall bleeds, spontaneous bleeds, and traumatic bleeds were recorded and their relation to treatment administration was noted. Data regarding target joint resolution was collected at the end of the observation period by the HJHS score and the FISH score.
Scoring and interpretation
Annualized Bleeding Rate (ABR)
The ABR is defined as follows:
Total bleeds during the observation period / Duration (in years). A lower ABR indicates better bleeding control.
HJHS 2.1 Score
The HJHS 2.1 score (range: 0 to 124) assesses joint health, including swelling, muscle atrophy, range of motion, and pain. Higher scores indicate worse joint damage. It includes a total score, joint-specific scores, and a global gait score.
FISH Score
The FISH score (range: 0 to 32) evaluates functional independence in daily activities. Higher scores reflect better physical function. Each activity is graded from 1 to 4 based on the amount of assistance required, and the score is determined through direct observation rather than self-reported ability.
There is no categorization (e.g., mild, moderate, severe) for either the HJHS or FISH scores.
The results are presented in descriptive form with mean and standard deviation. Inhibitor status of the patients was assessed throughout the observation period based on the routine monitoring plan.
Results
Demographics
Patients who were receiving prophylaxis with standard half-life (SHL) Factor IX and who were switched to extended half-life factor (N9-GP) at baseline are shown in Table 1. The mean age of the study patients was 11.2 years, with the youngest four years and the eldest 18 years (Table 2).
ABR outcomes
The mean overall ABR before using N9-GP was 21.1 (12 - 48) bleeds/year. N9-GP reduced the mean ABR from 21.1 to 0.42 bleeds/year, with 4/7 patients achieving zero bleeds. Three patients experienced minor bleeds pre-dose, suggesting potential for further dose optimization. Six patients had target joints before starting treatment. At the end of 12 months of prophylaxis, only one patient had target joint involving one joint with mobility and swelling improved (Figures 1, 2).
HJHS score before and after switching to N9-GP.HJHS: Hemophilia Joint Health Score; N9-GP: Nonacog Beta Pegol
FISH score before and after switching to N9-GP.FISH: Functional Independence Score in Hemophilia; N9-GP: Nonacog Beta Pegol
Four patients remained bleed free on N9-GP prophylaxis. Three patients presented with minor bleeds once before the next dose of prophylaxis. The bleeds were resolved with the standard treatment protocol.
Joint health & function
The baseline mean HJHS was 26.71/124 (10 - 47) which improved to mean of 7.5/124 (0-16) after 12 months on N9-GP. Before treatment, the mean FISH score was 23.8/32 (17-29) which also improved to mean FISH of 31.4/32 (28 - 31) after treatment (Table 3).
Safety profile
None of them developed any adverse drug reactions or thromboembolic events. None of the patients developed inhibitors. The dose of N9-GP used was 25-45 IU per kg with individualization.
Discussion
N9-GP 40 IU/kg/week is approved for prophylactic management of patients with hemophilia B [10,11]. However, low-dose prophylaxis is important in the context of resource-limited countries like India. An earlier study in India has shown that low-dose prophylaxis is better than on-demand treatment in children with hemophilia; it has shown not only to reduce the bleeds but also improve schooling and reduce hospital admissions [12]. Further health economic analysis has also shown that in Indian children, intermediate prophylaxis is better compared to on-demand treatment [13]. Studies done in other parts of the world also show that low-dose prophylaxis can provide a cost-effective option and play an important role in improving hemophilia care in developing countries [14,15]. At the end of 12 months of N9-GP prophylaxis, four patients remained bleed free, and three patients experienced minor bleeds once, just before the next dose of prophylaxis. Limited data on the efficacy of lower doses of 24N9 GP, especially in Indian patients, and the positive results from this study highlight the need for exploring dose individualization in patients with hemophilia B.
There are many studies that highlight the benefits of switching from standard half-life factors to extended half-life factors. Switching to extended half-life factors has been shown to reduce ABRs and reduce injection frequency and overall factor consumption [16,17]. An earlier real-world evidence study from Canada has shown that switching to N9-GP, irrespective of the previous product SHL or other EHLs, has been shown to reduce the median ABR and median factor consumption [18]. The Hemophilia Joint Health Score (HJHS) was specifically developed by the Physical Therapy Expert Working Group of the International Prophylaxis Study Group to detect early joint changes in boys aged 4 to 18 years with hemophilia. The current HJHS version 2.1 comprises an assessment of specific features, or items, of the six index joints and an assessment of global gait. For each of the six joints, the following items are scored: swelling (scored 0‐3), duration of swelling (0‐1), muscle atrophy (0‐2), crepitus on motion (0‐2), flexion loss (0‐3), extension loss (0‐3), joint pain (0‐2), and strength (0‐4). The maximum score for an individual index joint is 20. Gait is scored 0 to 4. The maximum HJHS total score is 124, with a higher score indicating worse joint health [19]. The HJHS reduced from 26.71/124 (range 10-47) to 7.5/124 (range 0 - 16) in the seven study participants after 12 months of low-dose N9 GP prophylaxis. Similarly, we have seen an improvement in the FISH score in patients who switched from SHL to N9-GP in our study. This is one of the first studies to report the improvement in HJHS after N9-GP prophylaxis in India. Similarly, we have seen an improvement in the FISH score in patients who switched from SHL to N9-GP in our study. HJHS improvements (26.71 → 7.5) and target joint resolution in 6/7 patients suggest N9-GP’s joint-protective effects, though the small sample warrants cautious interpretation. Even in this patient, the joint mobility and swelling were improved compared to the baseline.
At the end of 12 months of N9 GP prophylaxis, four patients remained bleed free, and three patients experienced minor bleeds once, just before the next dose of prophylaxis. Our study has shown resolution in the target joint in all but one patient. Even in this patient, the joint mobility and swelling were improved compared to the baseline.
Limitations
Though this descriptive case series has highlighted several advantages of using an individualized plan for managing patients with hemophilia, it has a small sample size, and without a control group, it is hard to apply the findings broadly. We propose doing a study involving multiple centers across India, probably register-based, involving a large number of patients.
Conclusions
Low-dose N9-GP prophylaxis significantly reduced bleeding and improved joint health in this Indian cohort, offering a feasible option for resource-limited settings. Larger studies are needed to validate dosing strategies. N9-GP has reduced bleeding episodes with less frequent injections, thus reducing infusion burden and facilitating adherence to prophylaxis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bleeding outcomes and factor utilization after switching to an extended half-life product for prophylaxis in haemophilia A in Austria Sci Rep Ay C Feistritzer C Rettl J Schuster G Vavrovsky A Perschy L Pabinger I 129671120213415522910.1038/s 41598-021-92245-5PMC 8217178 · doi ↗ · pubmed ↗
- 2Hemophilia A and B: molecular and clinical similarities and differences Haematologica Castaman G Matino D 1702170910420193139952710.3324/haematol.2019.221093 PMC 6717582 · doi ↗ · pubmed ↗
- 3Iranian low-dose escalating prophylaxis regimen in children with severe hemophilia A and B Clin Appl Thromb Hemost Eshghi P Sadeghi E Tara SZ Habibpanah B Hantooshzadeh R 513518242018 https://doi.org/10.1177/1076029616685429.2804935910.1177/1076029616685429 PMC 6714659 · doi ↗ · pubmed ↗
- 4Recombinant long-acting glyco PE Gylated factor IX (nonacog beta pegol) in haemophilia B: assessment of target joints in multinational phase 3 clinical trials Haemophilia Negrier C Young G Abdul Karim F 5075132220162693622710.1111/hae.12902 · doi ↗ · pubmed ↗
- 5Recombinant long-acting glyco PE Gylated factor IX in hemophilia B: a multinational randomized phase 3 trial Blood Collins PW Young G Knobe K 3880388612420142526119910.1182/blood-2014-05-573055 PMC 4271178 · doi ↗ · pubmed ↗
- 6Nonacog beta pegol (N 9-GP) in haemophilia B: A multinational phase III safety and efficacy extension trial (paradigm™4)Thromb Res Young G Collins PW Colberg T 697614120162697071610.1016/j.thromres.2016.02.030 · doi ↗ · pubmed ↗
- 7Insight into health-related quality of life of young children with haemophilia B treated with long-acting nonacog beta pegol recombinant factor IX Haemophilia Carcao M Kearney S Santagostino E 0423201710.1111/hae.1319528371032 · doi ↗ · pubmed ↗
- 8Long-term safety and efficacy of Nonacog Beta Pegol (N 9-GP) administered for at least 5 years in previously treated children with hemophilia B Thromb Haemost Carcao M Kearney S Lu MY Taki M Rubens D Shen C Santagostino E 73774612020203236984510.1055/s-0040-1709521 · doi ↗ · pubmed ↗