A cautionary tale of false-positive histoplasma urine antigen in an HIV patient: a case report
Mohammad Z. Khrais, Jake Smith, Tanmay Gandhi, Shahrukh Arif, Juan Carlos Rico

TL;DR
An HIV patient was mistakenly diagnosed with histoplasmosis due to a false-positive test, but was later correctly diagnosed with coccidioidomycosis after invasive testing.
Contribution
Highlights the risk of false-positive histoplasma antigen tests in diagnosing fungal infections and emphasizes the need for invasive diagnostics in ambiguous cases.
Findings
A false-positive histoplasma urine antigen test led to misdiagnosis of histoplasmosis in an HIV patient.
Coccidioidomycosis was confirmed through bronchoscopy and fungal culture after clinical worsening on initial treatment.
False positives can occur due to cross-reactions with other fungal infections like blastomycosis or paracoccidioidomycosis.
Abstract
Introduction. Coccidioidomycosis, or Valley fever, is a fungal disease caused by Coccidioides species, prevalent in parts of the southwestern United States. It usually results from inhaling spores from soil and is a common cause of pneumonia in these regions. Case Presentation. We present a unique case of coccidioidomycosis in an immunodeficient male patient secondary to human immunodeficiency virus infection with poor adherence to anti-retroviral treatment. After presenting with non-specific symptoms and pre-syncope, he was initially diagnosed with pneumonia based on chest X-ray findings, but his symptoms failed to improve with antibiotics. He was treated for presumed pulmonary histoplasmosis following a positive histoplasma urine antigen test. However, the patient worsened clinically. Following a computed tomography scan demonstrating a large necrotic lung consolidation, fungal stain…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1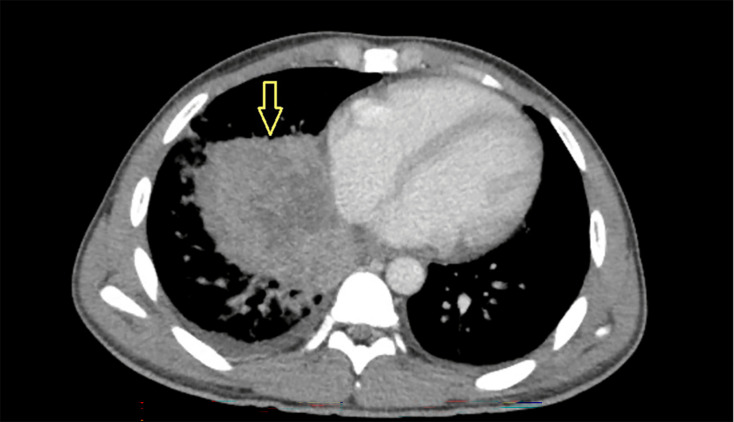 Fig. 2
Fig. 2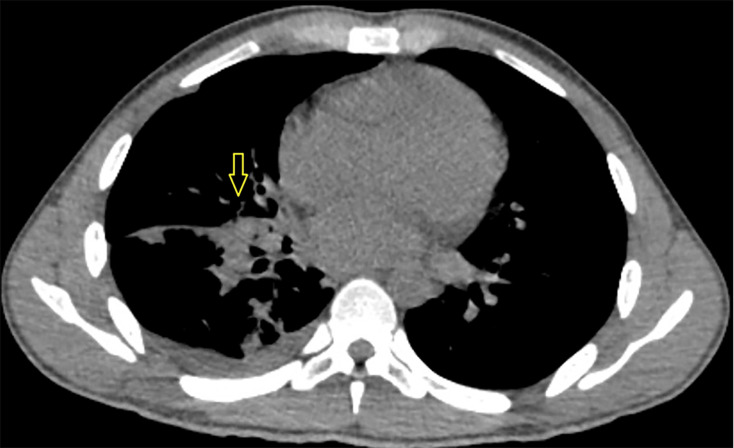 Fig. 3
Fig. 3| Test | Observed value | Reference range |
|---|---|---|
| CBC | ||
| Haemoglobin | 8.0 g dl−1 | 13.0–17.0 g dl−1 |
| WBC | 7.50 K µl−1 | 3.60–9.50 K µl−1 |
| Neutrophils | 69.9% – Absolute 5175 K µl−1 | |
| Lymphocytes | 5.3% – Absolute 397 K µl−1 | |
| Eosinophils | 0.0% – Absolute 0 K µl−1 | |
| Platelets | 532 K µl−1 | 150–450 K µl−1 |
| LDH | 262 IU l−1 | 100–248 IU l−1 |
| Procalcitonin | 0.05 ng ml−1 | 0.00–0.10 ng ml−1 |
| Peripheral smear | Mild hypochromic anaemia | |
| Serum β-glucan | 195 pg ml−1 | <80 pg ml−1 |
| Histoplasma antigens EIA | 1.56 ng ml−1 | None detected |
| Blastomyces antigens EIA | 1.11 ng ml−1 | None detected |
| COVID PCR | Negative | Negative |
| Screening MRSA PCR | Negative | Negative |
| Cryptococcal serum antigen | Negative | Negative |
| Aspergillus serum galactomannan | 0.11 | 0.00–0.49 |
| Histoplasma serum antibodies | Not detected | Not detected |
| Test | Observed value | Reference range | |
|---|---|---|---|
| At the time of diagnosis | One year after diagnosis | ||
| Coccidioides IgM | 3.7 | 0.7 | <=0.9 |
| Coccidioides IgG | 1.2 | 11.1 | <=0.9 |
| ID band | Positive | Positive | Not detected |
| CF antibody | 1 : 4 | 1 : 65536 | <1 : 2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Antifungal resistance and susceptibility · Phytoplasmas and Hemiptera pathogens
Data Summary
This article was previously presented as an abstract at the 2023 CHEST Annual Scientific Meeting on 11 October 2023.
All data associated with this work is reported within the article.
Introduction
Fungal infections in patients with human immunodeficiency virus (HIV) remain a significant cause of morbidity and mortality [1]. Histoplasmosis is a common infection among people with advanced HIV disease. It is caused by inhalation of the dimorphic fungus Histoplasma capsulatum, which is found in soil contaminated by bird or bat droppings. Histoplasmosis can manifest with non-specific symptoms like weight loss, fever and dyspnoea or can involve multiple organs in disseminated cases. Histoplasmosis is endemic in the United States, particularly in Ohio and Mississippi River Valleys [2].
Coccidioidomycosis is a less common endemic fungal infection caused by Coccidioides species and is transmitted via inhalation of fungal spores from soil. It can infect both immunocompetent and immunocompromised patients, presenting as a spectrum ranging from asymptomatic or mild, self-limiting respiratory illness to life-threatening pneumonia. Extra-pulmonary manifestations involving the skin, bones and central nervous system have also been reported [3]. Notably, most cases of coccidioidomycosis occur in the southwestern region of the United States (California, Arizona, Texas and Utah), with over 95% of cases diagnosed in Arizona and California [45].
Case presentation
A male patient in his twenties with a medical history significant for congenital HIV, non-adherent to anti-retroviral treatment (ART) and cryptococcal meningitis presented to a rural hospital in Arkansas with fatigue and light-headedness. He was found to have a right lung opacity on chest X-ray (Fig. 1) and a positive urine histoplasma antigen test. However, the HIV workup indicated severe immunosuppression with a CD4 count of 4 cells µl^−1^ (Reference range: 430–1800 cells ul^−1^), and an HIV viral load of 75,432 copies ml^−1^ (Reference range: not detected). The patient was initially treated with amoxicillin–clavulanic acid for presumed bacterial pneumonia and fluconazole for presumed histoplasmosis.
Chest X-ray from admission demonstrating right lower zone radiopacity with air bronchograms.
His fever persisted, and his cough worsened. Three weeks after the initial presentation, he was transferred to our tertiary care centre. On presentation, he had a low-grade fever (maximum temperature of 100.5 °F), mild tachycardia (heart rate in the 100s-110s) and normal blood pressure and oxygen saturation on room air. Initial laboratory workup was significant for hypochromic anaemia with haemoglobin of 8 g dL^−1^, positive histoplasma and blastomyces antigen enzyme immunoassay (EIA) by MiraVista Diagnostics and a sputum fungal culture positive for one colony of Blastomyces dermatitidis (Table 1).
Computed tomography (CT) of chest with contrast revealed a necrotic lung mass in the right lower lobe measuring 9×6.5×8.5 cm, with internal septation and cystic changes (Fig. 2). The patient underwent fine-needle aspiration guided by endobronchial ultrasound (EBUS) of the right lower lobe mass and bronchoalveolar lavage (BAL) of the right lower lobe. BAL showed 39% neutrophils and 60% macrophages. The β-glucan level was elevated in BAL fluid analysis. Definitive diagnosis with BAL and tissue cultures grew Coccidioides immitis and Coccidioides posadasii, establishing a geographically rare and unexpected diagnosis. The potato dextrose agar and the brain heart infusion cultures were used, and both were positive. After seeing the organism on calcofluor white stain, serology for coccidioidomycosis was obtained and further confirmed the diagnosis (Table 2).
A CT scan with intravenous contrast demonstrating a necrotic lung lesion with small layering right-side pleural effusion.
The patient was initially started on itraconazole but continued to have fevers with a maximum temperature of 105 °F and decreased oxygen saturation requiring supplemental oxygen via nasal cannula. Itraconazole was switched to intravenous (IV) liposomal amphotericin with a resolution of fever. The patient continued to improve and was discharged home on itraconazole after completing 14 days of IV liposomal amphotericin. The patient missed follow-up appointments after discharge and was readmitted a year later with cough and fever. He received itraconazole for presumed relapsed coccidioidomycosis, likely due to poor adherence to ART and itraconazole. A follow-up chest CT showed that the lung mass had decreased in size to 4.4×3.1 cm (Fig. 3).
Repeat CT chest without contrast demonstrating decrease in size of right perihilar mass.
Discussion
Differentiating between histoplasmosis, blastomycosis or coccidioidomycosis can be challenging because these endemic mycoses often present with non-specific signs and symptoms. Additionally, high sensitivities and low specificities of their diagnostic tests can confuse diagnosis. This was particularly evident in our case, where the patient presented with non-specific symptoms, and both histoplasma and blastomyces antigen EIAs were positive on EIA. Furthermore, the patient’s non-invasive sputum culture grew a colony of B. dermatitidis. The MVista^®^ Quantitative Histoplasma Antigen EIA is a commercially available antigen test, which has 95–100 % sensitivity for histoplasma antigen in the urine [6]. Although antigen detection tests are most sensitive to diagnose histoplasmosis, they are prone to false-positive results due to cross-reactivity with other fungal infections such as blastomycosis, paracoccidioidomycosis, talaromycosis and aspergillosis, and even medications such as rabbit anti-thymocyte globulin infusions [710]. This cross-reactivity is due to galactomannan and other polysaccharides in the cell walls of different mycotic species, and those epitopes can be recognized by the same antibodies used in the antigen tests. In one study, histoplasma antigen tests were suggested as a potential diagnostic tool for coccidioidomycosis, as 11 of 19 (58%) patients with coccidioidomycosis had a positive histoplasma antigen test [11].
Traditional methods for detecting coccidioidomycosis, such as culture and direct visualization, have limitations and pose risks. KOH (potassium hydroxide) and Silver Stain are preferred for their simplicity and affordability in direct observation. Coccidioides antigen detection tests exist, but their sensitivity is lower than histoplasma antigen tests to detect Coccidioides. However, antigen detection using urine samples is non-invasive and appears more sensitive than serum or BAL. While antigen and antibody tests play important roles in clinical settings, they may be insufficient on their own [12]. Serology is a more reliable and commonly used test to diagnose coccidioidomycosis. Combining antigen and antibody EIA tests improves detection accuracy, and the measurement of combined IgM and IgG by EIA can increase sensitivity to 95% or higher [10]. Although culture or direct visualization is the gold standard for the diagnosis of coccidioidomycosis, its utility is limited by lower sensitivity and extended incubation times [13]. The GeneSTAT Coccidioides Assay is the first FDA-authorized real-time PCR-based test for the rapid detection of coccidioidomycosis, complementing serology and antigen detection to enhance diagnostic accuracy [14].
This case report highlights the importance of considering diagnoses even beyond commonly accepted geographic boundaries. While endemic mycoses have been historically named after their approximate geographic distribution, their ranges can be broader than their names suggest, leading to incorrect or missed diagnoses [15]. Our patient was diagnosed in an area with a high incidence of histoplasmosis and outside of the endemic geographic range of coccidioidomycosis, with minimal incidence of coccidioidomycosis (less than 5 cases per 100,000 people) [1617]. Furthermore, patients travel. Our patient made frequent trips to Texas for work, which actually may have been the location of his exposure.
Coinfection with different endemic mycoses should be considered, especially in immunocompromised patients. In the case of our patient, it remains unclear whether the single B. dermatitidis colony that grew from the sputum culture was misidentified, was correctly identified but did not contribute to the patient’s pathology or contributed to his pathology but was treated effectively by the itraconazole prescribed for Coccidioides. This case highlights the potential consequences of relying solely on antigen tests, as exemplified by documented cases of delayed diagnosis, prolonged symptoms and possible unnecessary antibacterial treatment in patients with coccidioidomycosis diagnosed outside endemic areas [1718]. Finally, BAL and EBUS should be considered when diagnosis is uncertain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sati H Alastruey-Izquierdo A Perfect J Govender NP Harrison TS et al HIV and fungal priority pathogens Lancet HIV 202310 e 750e 75410.1016/S 2352-3018(23)00174-137827187 PMC 7615271 · doi ↗ · pubmed ↗
- 2Valdez AF Miranda DZ Guimarães AJ Nimrichter L Nosanchuk JD Pathogenicity & virulence of Histoplasma capsulatum - a multifaceted organism adapted to intracellular environments Virulence 2022131900191910.1080/21505594.2022.213798736266777 PMC 9621017 · doi ↗ · pubmed ↗
- 3Kim MM Blair JE Carey EJ Wu Q Smilack JD Coccidioidal pneumonia, phoenix, arizona, USA, 2000-2004 Emerg Infect Dis 20001510.3201/eid 1503.081007 PMC 268111919239751 · doi ↗ · pubmed ↗
- 4Ashraf N Kubat RC Poplin V Adenis AA Denning DW et al Re-drawing the maps for endemic mycoses Mycopathologia 202018584386510.1007/s 11046-020-00431-232040709 PMC 7416457 · doi ↗ · pubmed ↗
- 5Mc Cotter OZ Benedict K Engelthaler DM Komatsu K Lucas KD et al Update on the epidemiology of coccidioidomycosis in the United States Med Mycol 201957 S 30S 4010.1093/mmy/myy 09530690599 PMC 6823633 · doi ↗ · pubmed ↗
- 6Myint T Leedy N Villacorta Cari E Wheat LJ HIV-associated histoplasmosis: current perspectives HIV AIDS 20201211312510.2147/HIV.S 185631 PMC 709019032256121 · doi ↗ · pubmed ↗
- 7Persaud SP Lawton T Burnham C-A Anderson NW Comparison of urine antigen assays for the diagnosis of Histoplasma capsulatum infection J Appl Lab Med 2019437038210.1373/jalm.2018.02891031659074 · doi ↗ · pubmed ↗
- 8Gajurel K Dhakal R Deresinski S Diagnosis and treatment of histoplasmosis in solid organ transplant patients Curr Opin Infect Dis 20183130130810.1097/QCO.000000000000045729738315 · doi ↗ · pubmed ↗