Drainage for complete obstruction of the posterior bile duct after pancreatoduodenectomy with a forward-viewing echoendoscope
Shin Yagi, Susumu Hijioka, Yoshikuni Nagashio, Shota Harai, Mark Chatto, Yutaka Saito, Takuji Okusaka

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
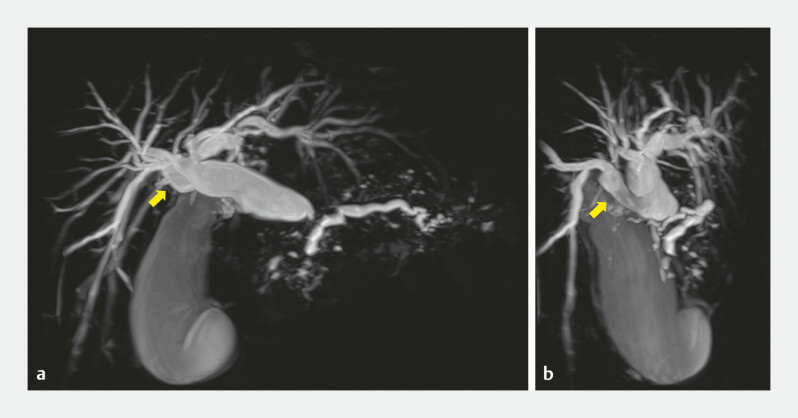 Fig. 1
Fig. 1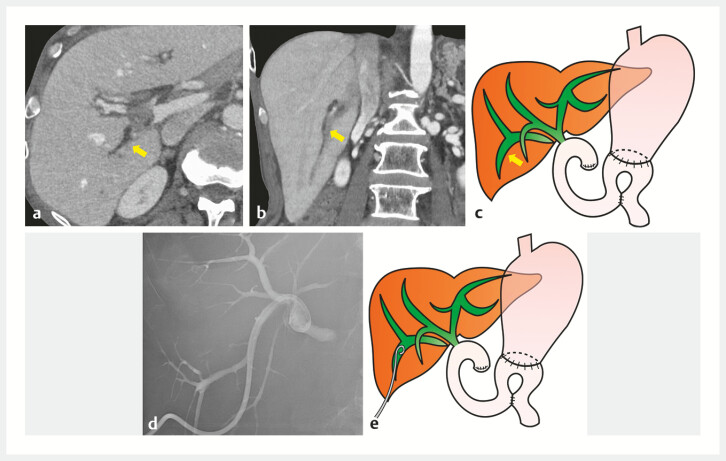 Fig. 2
Fig. 2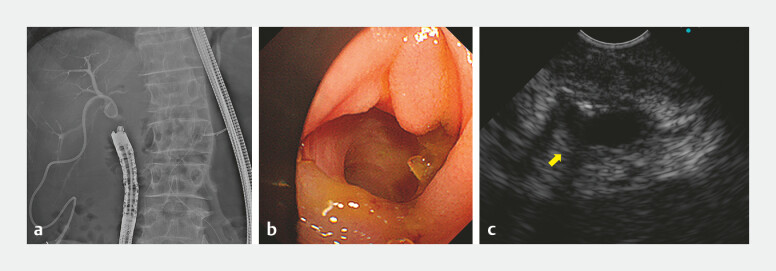 Fig. 3
Fig. 3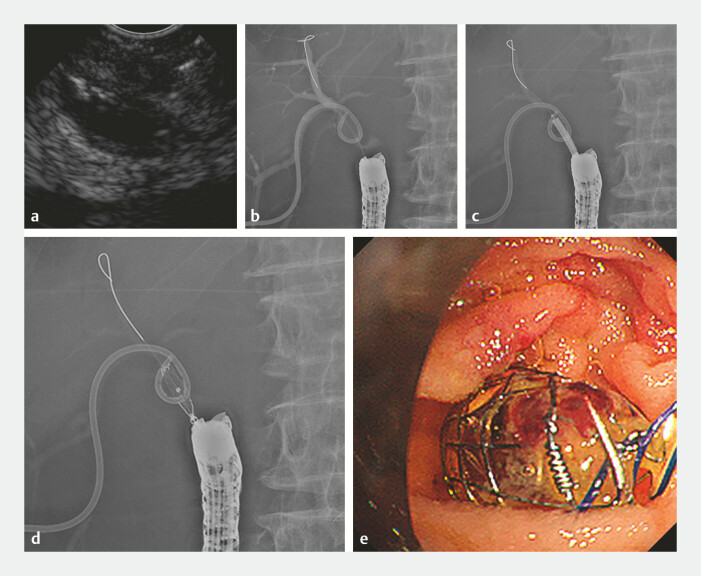 Fig. 4
Fig. 4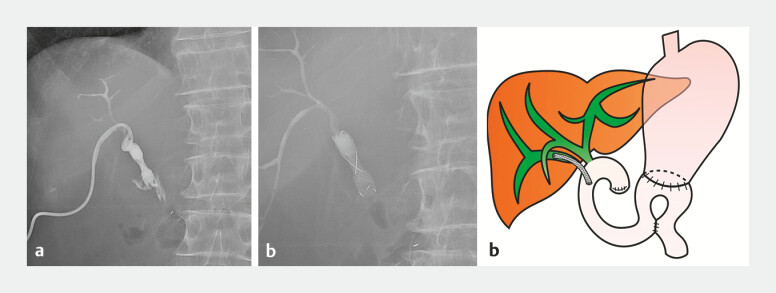 Fig. 5
Fig. 5- —National Cancer Center Research and Development Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gallbladder and Bile Duct Disorders · Pancreatitis Pathology and Treatment
The first-line treatment for hepaticojejunostomy anastomotic stenosis is balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography, which is difficult to perform in some cases 1 , despite the usefulness of a salvage method using a forward-viewing (FV) echoendoscope 2 3 . Here, we report a case of endoscopic ultrasound-guided biliary drainage (EUS-BD) using am FV echoendoscope in a patient with complete obstruction of the right posterior hepatic duct after surgery.
A 50-year-old man underwent a pancreaticoduodenectomy for pancreatic head cancer. The patient presented with an infraportal anomaly in the right posterior bile duct ( Fig. 1 a, b ) 4 . Ignorance of this anomaly during a pancreaticoduodenectomy led to complete iatrogenic transection of the right posterior hepatic duct, leading to its complete obstruction and resulting in postoperative cholangitis development ( Fig. 2 a–c ). Percutaneous transhepatic biliary drainage (PTBD) was performed for cholangitis ( Fig. 2 d, e ); however, the guidewire was unable to advance from the PTBD side to the intestine owing to complete obstruction. Therefore, we decided to perform EUS-BD with an FV echoendoscope ( Video 1 ). An FV echoendoscope was inserted to visualize the complete obstruction near the hepaticojejunostomy anastomosis ( Fig. 3 a–c ). A 19G needle (EZ Shot 3 Plus; Olympus Medical Systems, Tokyo, Japan) was used to puncture the right posterior hepatic duct, and a 0.025-inch guidewire was inserted into the bile duct ( Fig. 4 a, b ). The fistula was dilated with a 6-mm balloon catheter (REN; Kaneka Medix Corp., Osaka, Japan), and a fully covered metal stent (BONASTENT M-Intraductal, 8 mm, 3 cm; Medicoʼs Hirata, Tokyo, Japan) was placed ( Fig. 4 c–e ). After stent placement, a good outflow of contrast from the PTBD to the intestinal side was observed. A few days later, the PTBD was removed ( Fig. 5 a–c ); no recurrence of cholangitis was observed, and the patient was discharged.
Preoperative magnetic resonance imaging showed an infraportal anomaly of the right posterior bile duct (arrow).
a–c Computed tomography scan images and schema showed the completely obstructed and dilated right posterior hepatic duct (arrow). a, b Axial and coronal images. d, e Radiographic image and schema showed the right posterior hepatic duct after percutaneous transhepatic biliary drainage placement.
Endoscopic ultrasound-guided biliary drainage using a forward-viewing echoendoscope in a patient with complete obstruction of the right posterior hepatic duct after pancreaticoduodenectomy.Video 1
a Radiographic image showed the forward-viewing echoendoscope inserted near the hepaticojejunostomy anastomosis. b Endoscopic image showed the hepaticojejunostomy anastomosis. c Endoscopic ultrasound image showed the right posterior hepatic duct (arrow) visualized near the hepaticojejunostomy anastomosis.
a Endoscopic ultrasound image showed puncture of the right posterior hepatic duct using a forward-viewing echoendoscope. b Radiographic image showed the insertion of a guidewire into the bile duct. c Radiographic image showed dilation of the fistula with a 6-mm balloon catheter. d, e Radiographic image and endoscopic image after the placement of a fully covered metal stent.
a Radiographic image showed contrast flow from the percutaneous transhepatic biliary drainage to the intestinal side. b, c Radiographic image and schema after percutaneous transhepatic biliary drainage removal.
Hence, EUS-BD with an FV echoendoscope may be a useful option for complete biliary obstruction caused by surgical procedures, as in the present case.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yane K Katanuma A Maguchi H Short-type single-balloon enteroscope-assisted ERCP in postsurgical altered anatomy: potential factors affecting procedural failure Endoscopy 201749697410.1055/s-0042-11830127760436 · doi ↗ · pubmed ↗
- 2Iwai T Kida M Yamauchi HEUS-guided transanastomotic drainage for severe biliopancreatic anastomotic stricture using a forward-viewing echoendoscope in patients with surgically altered anatomy Endosc Ultrasound 202110333833473043 10.4103/eus.eus_72_20PMC 7980695 · doi ↗ · pubmed ↗
- 3Takeshita K Hijioka S Kawasaki Y Endoscopic ultrasound-guided hepaticojejunostomy for drainage of the right posterior hepatic duct enabled total liver drainage Endoscopy 202355 E 346E 34810.1055/a-1990-098236646120 PMC 9842443 · doi ↗ · pubmed ↗
- 4Takeishi K Shirabe K Yoshida Y Correlation between portal vein anatomy and bile duct variation in 407 living liver donors Am J Transplant 20151515516025521764 10.1111/ajt.12965 · doi ↗ · pubmed ↗