Acute Spinal Cord Infarction Secondary to Spinal Dural Arteriovenous Fistula: A Rare Cause of Reversible Paraplegia
Chien-Wei Li, Chun-Hsin Teng, Tzu-Chao Lin, I-Hsiao Yang, Poyin Huang

TL;DR
A rare spinal dural arteriovenous fistula caused sudden paraplegia, but quick treatment led to partial recovery.
Contribution
Highlights a rare but treatable cause of acute paraplegia through a case report and successful intervention.
Findings
AV fistula was identified as the cause of acute spinal cord infarction in a 76-year-old male.
Urgent embolization led to significant recovery of muscle strength despite persistent neurogenic bladder.
Timely diagnosis and intervention are crucial for managing reversible paraplegia.
Abstract
Acute spinal cord infarction due to spinal dural arteriovenous (AV) fistula is a rare etiology of acute paraplegia that challenges timely diagnosis. We report a case of a 76-year-old male presenting with sudden bilateral lower extremity weakness, urinary retention, and constipation. Diagnostic evaluation revealed an AV fistula causing spinal cord infarction, confirmed by imaging. Urgent embolization resulted in significant recovery of muscle strength, though neurogenic bladder persisted. This case underscores the importance of identifying reversible causes of acute paraplegia and the critical role of prompt intervention.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
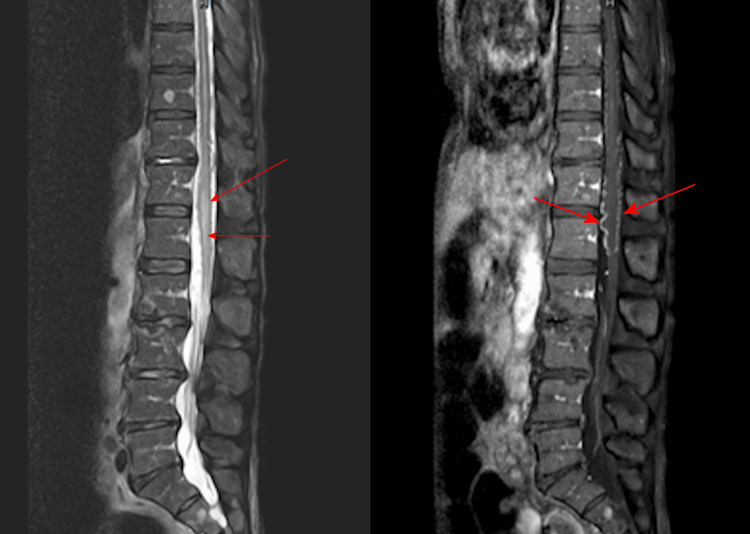 Figure 1
Figure 1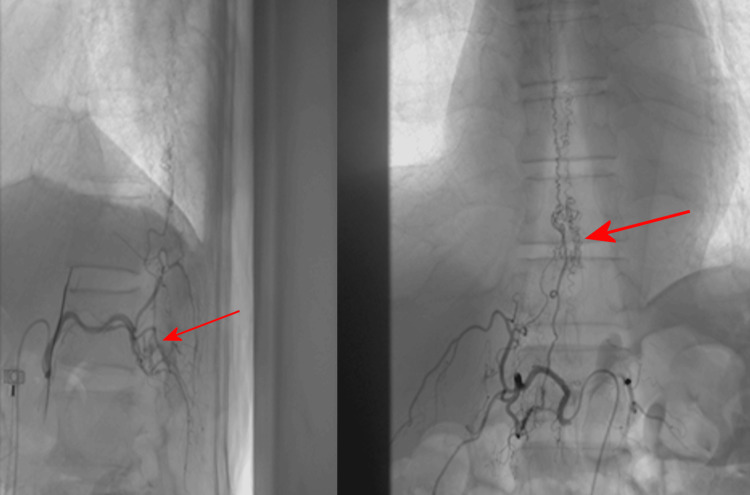 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations Diagnosis and Treatment · Intracranial Aneurysms: Treatment and Complications · Aortic aneurysm repair treatments
Introduction
Acute paraplegia is a medical emergency requiring timely diagnosis to address reversible etiologies and prevent permanent neurologic damage. Common non-traumatic causes include Guillain-Barré syndrome (GBS), transverse myelitis, and tumor-related compression or metastasis, often accompanied by autonomic dysfunction. Rarely, spinal cord infarction secondary to vascular malformations, such as spinal dural arteriovenous (AV) fistulas, may present similarly [1]. Though uncommon, early recognition and intervention can significantly improve the outcome. Here, we report a case of acute paraplegia resulting from AV fistula-induced spinal cord infarction, emphasizing the critical importance of timely recognition and early intervention.
Case presentation
A previously healthy 76-year-old male presented with acute bilateral lower extremity soreness below the umbilicus and lower back pain. Three days later, he developed urinary retention and constipation, followed by sudden bilateral lower extremity weakness with an ascending pattern on day 4. Additionally, he described a tingling sensation, initially in the right leg and then the left. No preceding trauma, infection, vaccination, or systemic symptoms were reported. Initial differential diagnoses included GBS, transverse myelitis, and anterior spinal artery infarction.
On admission, neurologic examination revealed flaccid weakness in both lower extremities (worse distally), bilateral plantarflexion, impaired joint position sense, and relatively preserved pinprick sensation. Pulse therapy of corticosteroids was used initially but in vain, and muscle strength deteriorated by day 2 to a Medical Research Council (MRC) scale score of 1 proximally and 0 distally bilaterally. Thoracolumbar spine magnetic resonance imaging (MRI) with and without contrast demonstrated myelopathy at T12-L1, suggestive of acute spinal cord infarction secondary to an AV fistula (Figure 1). Further digital subtraction angiography confirmed the diagnosis of AV fistula at T12-L1 with venous congestion (Figure 2).
Myelopathy at T12-L1 under thoracolumbar spine magnetic resonance imaging (MRI) Coronal T2-weighted MRI of the thoracolumbar spine showing longitudinal spinal cord edema (red arrows), suggesting acute infarction due to venous congestion resulting from a dural arteriovenous fistula.
An AV fistula at T12-L1 with venous congestion under angiographyDigital subtraction angiography demonstrating an AV fistula at T12-L1 (red arrow) with associated venous congestion (large red arrow), thereby confirming the underlying cause of the spinal cord infarction.AV: arteriovenous
Neurosurgical consultation deemed surgery inappropriate, and urgent embolization was performed. After the therapeutic procedure, his strength in bilateral lower extremities improved markedly, and paresthesia partially resolved. However, the neurogenic bladder persisted, necessitating an indwelling catheter. He was transferred to a rehabilitation unit for ongoing care.
Discussion
Acute paraplegia requires urgent assessment, since delay in diagnosis may result in irreversible neurological deficits. In comparison with other frequent culprits, spinal cord infarction is extremely rare, accounting for less than 1% of all infarctions [2]. The resulting sequelae, including paraplegia, quadriplegia, ataxia, or autonomic dysfunction, are determined by the spinal segment involved. In most cases, spinal cord infarction stems from extravertebral artery or aortic injury (e.g., surgical clamping or severe hypotension), while spinal vascular malformations (e.g., dural AV fistulas) are only implicated in a minority of instances. Representing 70% of spinal vascular malformations, dural AV fistulas cause infarction via venous congestion, leading to intramedullary edema and hypoxia [3,4].
In this patient, thoracolumbar MRI helped with identifying spinal infarction, and angiography further confirmed a dural AV fistula as the cause. Embolization rapidly improved motor function, consistent with prior reports of reversible deficits when venous hypertension is alleviated promptly. However, autonomic dysfunction, such as neurogenic bladder, often persists, reflecting differential recovery potential among spinal cord functions [5].
Conclusions
This case illustrates that spinal cord infarction secondary to dural AV fistula, though rare, should be considered in case of acute paraplegia with autonomic features. Urgent MRI and angiography, coupled with timely embolization, can reverse motor deficits and avert catastrophic outcomes. Clinicians should remain vigilant and consider these reversible causes in their differential diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spinal stroke in older people secondary to dural arteriovenous fistula BMJ Case Rep Pillai SK Subramaniam T Rao GG 2011201110.1136/bcr.06.2011.4373 PMC 317104622688942 · doi ↗ · pubmed ↗
- 2Spinal dural arteriovenous fistulas AJNR Am J Neuroradiol Krings T Geibprasert S 6396483020091921381810.3174/ajnr.A 1485 PMC 7051782 · doi ↗ · pubmed ↗
- 3Spinal dural arteriovenous fistula: the pathology of venous hypertensive myelopathy Neurology Hurst RW Kenyon LC Lavi E Raps EC Marcotte P 13091313451995761718910.1212/wnl.45.7.1309 · doi ↗ · pubmed ↗
- 4Management of spinal dural arteriovenous fistulas: report of 12 cases and review of literature Clin Neurol Neurosurg Rashad S Abdel-Bary M Aziz W Hassan T 818612520142510869710.1016/j.clineuro.2014.07.028 · doi ↗ · pubmed ↗
- 5Multidisciplinary management of spinal dural arteriovenous fistulas: clinical presentation and long-term follow-up in 49 patients Stroke Van Dijk JM Ter Brugge KG Willinsky RA Farb RI Wallace MC 157815833320021205299410.1161/01.str.0000018009.83713.06 · doi ↗ · pubmed ↗