Chronic wasting disease as a model for human prion therapy
Michael Bordonaro

TL;DR
The paper suggests using chronic wasting disease in cervids as a model to test therapies for human prion diseases, due to its natural occurrence and potential future transmission risks.
Contribution
The novelty lies in proposing CWD as a natural model for testing human prion therapies in real-world settings.
Findings
CWD occurs naturally in free-ranging cervids, making it a unique model for prion disease research.
Testing therapies on CWD could reduce animal suffering and prevent potential future transmission to humans.
Current therapies include prion expression knockdown and overexpression of dominant negative prion forms.
Abstract
Prion diseases, also known as transmissible spongiform encephalopathies (TSEs), are fatal neurodegenerative disorders that result from abnormally folded prion proteins. These disorders can be sporadic, acquired, or genetic. Acquired TSEs can be found in a number of animal species including sheep (scrapie), cows (bovine spongiform encephalopathy), and cervids (chronic wasting disease). Chronic wasting disease (CWD) is unusual in that it is found in free ranging animals in their natural environment. There has been heretofore no reported cases of CWD being transmitted to humans; however, the possibility of future adaption for human transmission exists. Several novel approaches for the prevention and treatment of prion disease in humans are under development, including knockdown of endogenous prion expression or overexpression of dominant negative prion forms. Here, I propose that CWD, as a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
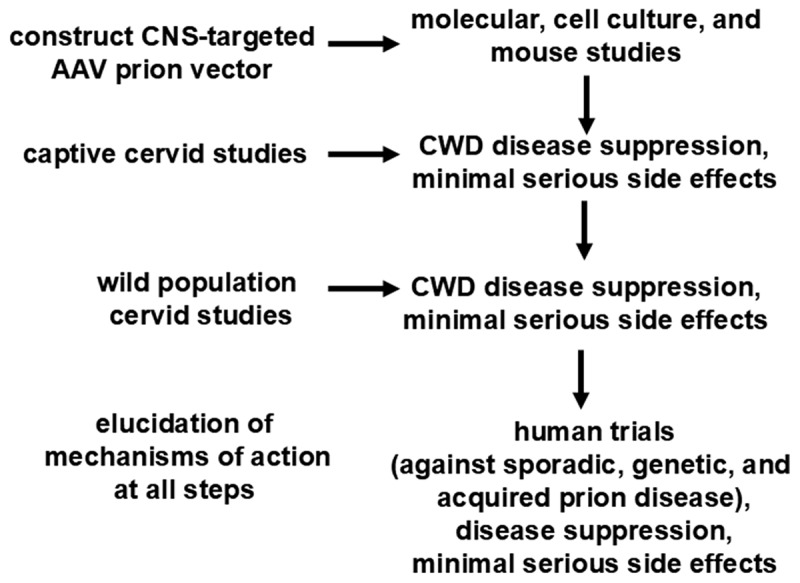 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrion Diseases and Protein Misfolding
INTRODUCTION
Prion diseases (transmissible spongiform encephalopathies or TSEs) are invariably fatal neurodegenerative disorders [1,2] that result from the downstream consequences of the accumulation of abnormally folded prion proteins (PrPs). TSEs can be sporadic; genetic, with an age-related onset [1–3]; or acquired.
Besides iatrogenic prion disease and variant Creutzfeldt Jakob Disease (vCJD) in humans, acquired TSEs can be found in a number of animal species including sheep (scrapie), cows (bovine spongiform encephalopathy, transmitted to humans as vCJD), and cervids (chronic wasting disease). Having an international distribution and currently concentrated in North America [4–10], chronic wasting disease (CWD) manifests in cervids with a variety of behavioural and physical changes leading to rapidly advancing morbidity and mortality.
CWD is unusual in that it is found in free ranging animals in their natural environment as opposed to being restricted to livestock [4–10]. Further, as the infectious agent is found not only in neuronal but also in extraneural tissue as well as in bodily fluids and excreta, horizontal transmission is common [5,11]. Transmissibility is exacerbated by the stability of the infectious prions in the natural environment. There are as of today no reported definitive cases of CWD being transmitted to humans [5]. Experiments in humanized mouse models of prion disease have not demonstrated transmission; however, in vitro experiments have shown contradictory results and the possibility of future adaption for human transmission exists [5]. Vertical transmission of CWD also occurs in cervids, contributing to disease prevalence [6]. Experimental transmission of CWD to a number of non-cervid (non-humanized) species has been observed, including sheep, rodents, primates, and various carnivores, with canids appearing to be resistant [8]. Vaccination against CWD has been explored as a preventive option, and is still under investigation [12,13] to address this disorder, but success has not yet been achieved. At best, a delay in symptomology in some animals has been observed.
There are several novel approaches for the prevention and treatment of prion disease in humans currently under development. For example, a monoclonal antibody (PRN100) to cellular prion protein has been proposed as a treatment for human prion disease [14]. While not cytotoxic in initial testing, and reaching target drug concentrations, PRN100 treatment still resulted in all patients exhibiting progressive decline in neurological functioning [14]. Thus, while this approach is promising, it is prudent to continue the development of other novel therapies, such as molecular gene therapy approaches.
A potential problem with some proposed pharmacological and immunological therapeutic approaches, in both humans and in animals such as cervids, is the possibility of prion resistance to therapy based on conformational mutation and selection; this has been shown to occur in response to pharmacological therapeutics [15–19]. However, based on experience with Kuru in the Fore people and data from mouse models [20], molecular-directed therapies may be more stable with respect to resistance than are pharmacological or immunological interventions.
These molecular approaches include knockdown of endogenous prion expression [21,22] or overexpression of dominant negative prion forms [20,23,24]. The knockdown option involves depleting levels of the endogenous PrP substrate to reduce PrP availability for conversion, and thus delay disease progression, and has been suggested as a resistance-proof therapeutic strategy [17]. The overexpression option involves utilizing dominant negative exogenous PrP variants to inhibit endogenous PrP conversion and thus suppress disease development. Dominant negative prion variants adopt conformations that inhibit conversion and propagation of pathogenic prion forms [20–25]. The validity of the dominant negative approach is suggested by the existence of naturally occurring PrP variants, presumably existing because of selective pressure, which confer varying degrees of resistance to prion disease [20,25]. Combining overexpression with deletion molecular strategies [24] might be the optimal strategy for both prevention of prion conversion and prevention of resistance to therapy. In addition, resistance can apparently be reversed when the selective pressure is removed, suggesting intermittent changes in therapeutics could be helpful as a strategy against resistance in those cases in which resistance may occur [18]. In the case of molecular therapy, this suggests switching between endogenous PrP depletion and dominant negative PrP expression as a reasonable anti-resistance strategy.
With respect to designing the most appropriate dominant negative PrP molecular approaches for prion disease therapy, it is known that genetic variation in the PRNP gene can influence susceptibility to prion disease in humans [20,25], while codon 171 variants in sheep and codon 163 variants in Canidae confer prion disease resistance in those mammals [26]. PNRP genetic variation in cervids also influences susceptibility to CWD, but complete resistance has not been observed [6]. It is uncertain if complete resistance could be achieved with overexpression [20,23,24] of any known cervid prion variants; thus, it is possible that native PrP variants would not be suitable for overexpression therapy in cervids. If so, other types of dominant negative PrP variants would need to be used, either those adapted from other mammals [26] or via artificially generated variants, perhaps identified by computational modelling.
With respect to gene therapy for the central nervous system (CNS), an adeno-associated virus (AAV) capsid that binds the human transferrin receptor, which is expressed on the blood‒brain barrier, allows for increased CNS-specific expression in mouse models [27]. Thus, this system is a possible approach for CNS-targeted therapy for prion disease. Therefore, using gene therapy vectors for CNS-directed overexpression is theoretically possible [23,24] and the knockdown methodology is also feasible, with recent in vivo data supporting that approach [21,22].
PROPOSED APPROACH AND TESTING
This paper proposes that CWD should be utilized as a testing target for novel prion disease therapies, particularly those involving knockdown of endogenous prion expression or overexpression of dominant negative prion forms. This would allow testing of these approaches in a natural environment outside of controlled laboratory settings, and if successful would provide direction for human clinical trials; it would alleviate animal suffering in wild cervid populations afflicted with this devastating disease; and would lessen the probability of cross-species transmission to other mammals, including the possibility of adaption for human transmission.
The general approach would be as follows (Figure 1). Preliminary work would include designing the appropriate vectors and payloads for therapy, such as the therapy approaches discussed in the Introduction. A fundamental initial step would be to identify a PrP variant that would prevent prion conversion and disease progression in cervids. In vitro molecular and cell culture experiments could be performed to ascertain if abnormal prion seeding and spread is inhibited by the knockdown or overexpression approaches. However, there is a question whether in vitro studies can capture mechanisms of prion resistance using the dominant negative approach; it is possible in vivo mouse studies would be required [20,24]. The latter would require a mouse expressing cervid PrP; thus, akin to humanized mouse models, it may be necessary to create a ‘cervidized’ mouse that can serve as an appropriate in vivo experimental model for CWD. Since mouse experiments with the human V127 PrP variant suggests dosage effects in which optimized protection is observed with increasing expression of the variant vs. wild-type allele [20], it is possible that a successful gene therapy approach against prion disease would require a combination of methods [24]. First, knockdown of endogenous PNRP expression would reduce levels of the vulnerable wild-type PrP, and subsequent overexpression of the dominant negative form would tilt the balance towards optimized disease resistance. Figure 1.Process of assaying prospective therapies in deer. In vitro preliminary work at the molecular and cellular level and in vivo work with mice will be followed by in vivo experiments on captive cervids in controlled environments, followed by in vivo experiments on wild, free-ranging cervids in their natural environment. Optimal endpoints would be disease suppression and minimal serious side effects. Mechanism of action would be determined at each step, if possible. If this work is successful, it would provide further support for human clinical trials.Flowchart showing a prion vector strategy, leading from molecular studies to cervid and human trials, focusing on disease suppression and minimal side effects. The first step is a CNS-targeted AAV prion vector, for molecular, cell culture, and mouse studies. Next are captive and wild cervid studies to evaluate disease suppression and side effects. The last step is elucidation of mechanisms of action, followed by use against various forms of human prion disease.
The first in vivo experimental step involving the actual target species would be to ascertain if cervids – and we can propose that deer be the specific cervid used – treated with the relevant therapies are resistant to disease under controlled environmental conditions. Captive deer can be treated at four broad intervals: (1) before infectious exposure, (2) at different times after exposure but before any molecular signs of disease, (3) after molecular signs of disease but before symptomology, and then (4) after the first signs of symptomology. These deer would be compared to mock treated controls. Deer in both the experimental and control groups would be stratified as per their PRNP gene genetic background. Favourable results from these captive deer experiments can lead to the next steps involving free-ranging wild animals.
Progression from captive deer to wild population deer experiments will proceed only if the captive experiments do not result in significant long-term morbidity for the animals via serious side effects of treatment. Wild deer from areas with significant CWD prevalence can be captured, determined (to the extent possible) to be uninfected with CWD, assayed for genotype, labelled for subsequent tracking, treated with the appropriate therapies, and released back into the wild. Mock treated controls can be processed similarly. Rates of CWD incidence and prevalence in experimental vs. control animals would then be ascertained over time (stratified by genotypic data where available). Given that the incidence of CWD in the wild appears higher in male cervids, likely for behavioural reasons [8], the variable of sex would need to be evaluated in these studies. Neuropathology, immunohistochemistry, and other assays could be performed on post-treatment captured deer to track signs of progression in addition to evaluation of clinical symptomology. At all phases of experimental testing, potential side effects will be monitored. The hoped for outcome is decreased CWD in experimentally treated deer, with the optimal result being full, or at least a large degree of, CWD resistance. In addition, side effects of treatment should be short-term and relatively minimal.
Follow-up studies can attempt to ascertain if the predicted molecular mechanisms are responsible for any observed disease suppression. Success with this work would be further encouragement for the validity of the approach for human clinical trials, building upon experimental laboratory in vivo work studies utilizing established mouse models of prion disease.
CLARIFICATIONS AND OBJECTIONS
Before concluding this manuscript, clarifications of the concept as well as responses to potential objections are presented.
The current manuscript does not propose to use CWD in cervids to develop prion disease treatments for humans. The relevant mouse models adequately perform that role. Instead, I propose to utilize CWD in cervids as a testing model to evaluate genetic approaches developed in mice. Further, the current paper does not state that the cervid model is better than other alternative models and so should be used to the exclusion of other models. Instead, the argument is that free-ranging wild cervids and CWD represent a testing platform with useful features for evaluating potential human therapies, so that the cervid model is an important additional model to use in conjunction with others.
As stated above, the specific utility of the CWD-cervid model is the ability to evaluate novel prion therapies in a free-ranging mammalian population in its natural habitat, independent of a carefully controlled laboratory environment. An objection could be that the environment of wild cervids is quite different from that of humans. This is true, but the same can be said of any other animal model. However, some models are relatively more similar to the human condition than others. Thus, free-ranging, genetically diverse cervids interacting with their natural habitat can be considered conceptually more similar to the human condition compared to inbred mouse strains tested in artificial laboratory conditions. Humans are genetically diverse and interact with their environment independent of a controlled experimental protocol. In contrast, domestic cattle and sheep can be considered intermediate between laboratory mice vs. wild cervids. It is true that free-ranging sheep and scrapie can also serve as a natural testing model. However, CWD is an attractive target for testing given the rapidly spreading epidemic in wild cervid populations, particularly in North America, and the urgent need for effective treatments. CWD represents a convergence of practical need with experimental utility.
A related objection would be scepticism as to whether findings from CWD in cervids can be extrapolated to prion disease in humans. Of course, this is an issue with virtually all animal models, including laboratory mouse studies. However, the mechanisms of action for genetic therapies should in theory work against all prion diseases in all species that exhibit such disease. If in fact it is demonstrated that the results do not carry over from one species to others then this is an important data point that can inform directions for subsequent further experiments and optimization. If a general genetic approach works in the laboratory but not in the wild, this can serve as a warning that more work may be needed before human clinical trials.
Another objection to the proposed CWD-focused approach would be to question why we should focus on a prion disease not (currently) transmissible to humans, rather than on animal prion diseases that are. This can be answered three ways. First, nothing in the present manuscript precludes testing on other models of prion disease, including forms known to be transmissible to humans. Thus, the proposed genetic approach should work against vCJD in humans as well as BSE in cattle. As stated, the CWD-cervid testing model is not meant to be exclusive of others, but rather an important addition to other types of analysis. Second, the lack of (current) human transmissibility can be viewed as a safety advantage in conducting these experiments. Third, the potential for future transmissibility is a rationale for dealing with the CWD epidemic before such an eventuality occurs.
There is an urgent need for new human prion therapies. At the same time, there is also an urgent need to address the CWD epidemic. Novel genetic therapies aimed at inhibiting aberrant prion propagation in the CNS can serve both roles. For the reasons stated in this manuscript, testing these therapies in cervids against CWD would be a prudent additional step before human clinical trials. There is no compelling reason not to attempt this and no compelling reason to reject the opportunity to obtain potentially useful information for human trials while at the same time addressing the CWD crisis.
DISCUSSION
The proposed work has three potential practical benefits. First, using CWD as a natural environment, ‘real life’ model for testing novel preventive and therapeutic approaches against prion disease is of benefit to further evaluate approaches that could have potential human clinical utility. Unlike laboratory mice or livestock, free-ranging wild cervids have a more natural interaction with the environment and thus can more closely mimic the human situation in which prion disease can be acquired outside of carefully controlled conditions.
Thus, success would be an encouraging step towards human clinical trials. Second, from the standpoint of ethical promotion of animal well-being, effective treatment for CWD can alleviate significant suffering in cervid populations, decreasing morbidity and mortality from this disease. Thus, treating CWD in cervids is a positive step in its own right, independent of potential utility for human clinical testing. If molecular therapies work, there is an ethical imperative to alleviate animal suffering. Further, a similar approach can be used for other animal species that suffer from prion disease (e.g., sheep, cattle). As described above, alternative approaches, such as vaccination, have not been sufficiently effective and can in theory be countered by prion therapy resistance. Third, by decreasing the prevalence of prion disease in cervids, the risk of potential transmission to humans and other species [8,11,28] can be lessened.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gambetti P, Kong Q, Zou W, et al. Sporadic and familial CJD: classification and characterisation. Br Med Bull. 2003;66(1):213–239. doi: 10.1093/bmb/66.1.21314522861 · doi ↗ · pubmed ↗
- 2Kovács GG, Puopolo M, Ladogana A, et al. EUROCJD. Genetic prion disease: the EUROCJD experience. Hum Genet. 2006;118(2):166–174. doi: 10.1007/s 00439-005-0020-116187142 · doi ↗ · pubmed ↗
- 3Bordonaro M. Hypothesis: functional age and onset of autosomal dominant genetic prion disease. Theory Biosci. 2023;142[2(2):143–150. doi: 10.1007/s 12064-023-00389-x PMID: 37017882.37017882 · doi ↗ · pubmed ↗
- 4Williams ES. Chronic wasting disease. Vet Pathol. 2005;42(5):530–549. doi: 10.1354/vp.42-5-530 PMID: 16145200.16145200 · doi ↗ · pubmed ↗
- 5Hannaoui S, Schatzl HM, Gilch S, et al. Chronic wasting disease: emerging prions and their potential risk. Plo S Pathog. 2017 Nov 2;13(11):e 1006619. doi: 10.1371/journal.ppat.1006619 PMID: 2909592.29095921 PMC 5667731 · doi ↗ · pubmed ↗
- 6Rivera NA, Brandt AL, Novakofski JE, et al. Chronic wasting disease in cervids: prevalence, impact and management strategies. Vet Med (Auckl). 2019;10:123–139. doi: 10.2147/VMRR.S 197404 PMID: 31632898.31632898 PMC 6778748 · doi ↗ · pubmed ↗
- 7Winter SN, Escobar LE. Chronic wasting disease modeling: an overview. J Wildl Dis. 2020;56(4):741–758. doi: 10.7589/2019-08-213 PMID:32544029 Review.32544029 · doi ↗ · pubmed ↗
- 8Otero A, Velásquez CD, Aiken J, et al. Chronic wasting disease: a cervid prion infection looming to spillover. Vet Res. 2021;52(1):115. doi: 10.1186/s 13567-021-00986-y PMID: 34488900.34488900 PMC 8420063 · doi ↗ · pubmed ↗