Efficacy of brachytherapy for locally advanced bladder cancer: a single-center retrospective clinical study
Xuebing Han, Huiqing Chen, Bin Wang

TL;DR
A study found that adding brachytherapy to chemotherapy improves local cancer control in advanced bladder cancer patients undergoing surgery.
Contribution
The study demonstrates that brachytherapy combined with chemotherapy improves locoregional recurrence-free survival in locally advanced bladder cancer patients.
Findings
Brachytherapy + chemotherapy significantly improved 3-year locoregional recurrence-free survival compared to chemotherapy alone.
The treatment was safe with limited adverse effects and no major complications related to brachytherapy.
No significant differences in distant metastasis-free survival, disease-free survival, or overall survival were observed between groups.
Abstract
To explore the feasibility, safety, and effectiveness of brachytherapy of locally advanced bladder cancer, clinical data of 86 patients with locally advanced bladder cancer treated in the Department of Urology Surgery, Shanxi Provincial Cancer Hospital, between January 2015 and June 2019 were analyzed retrospectively. The patients were categorized into the study (n = 45) and control (n = 41) groups according to the treatment methods. Patients in the study group were treated with brachytherapy (intraoperative implantation of radioactive particles) + neoadjuvant chemotherapy (NAC), and those in the control group were treated with NAC. Patients in both groups underwent radical cystectomy (RC) + pelvic lymph node dissection. Postoperative pathological examinations proved that patients in both groups had urothelial carcinoma at stage pT3–pT4. The endpoints included 3-y locoregional…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
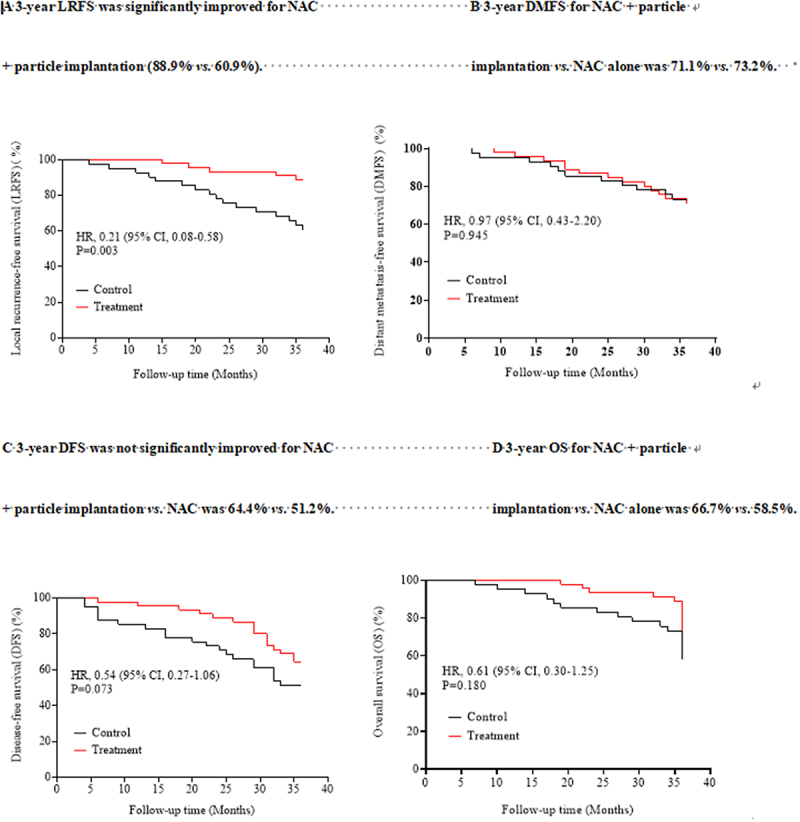 Figure 1
Figure 1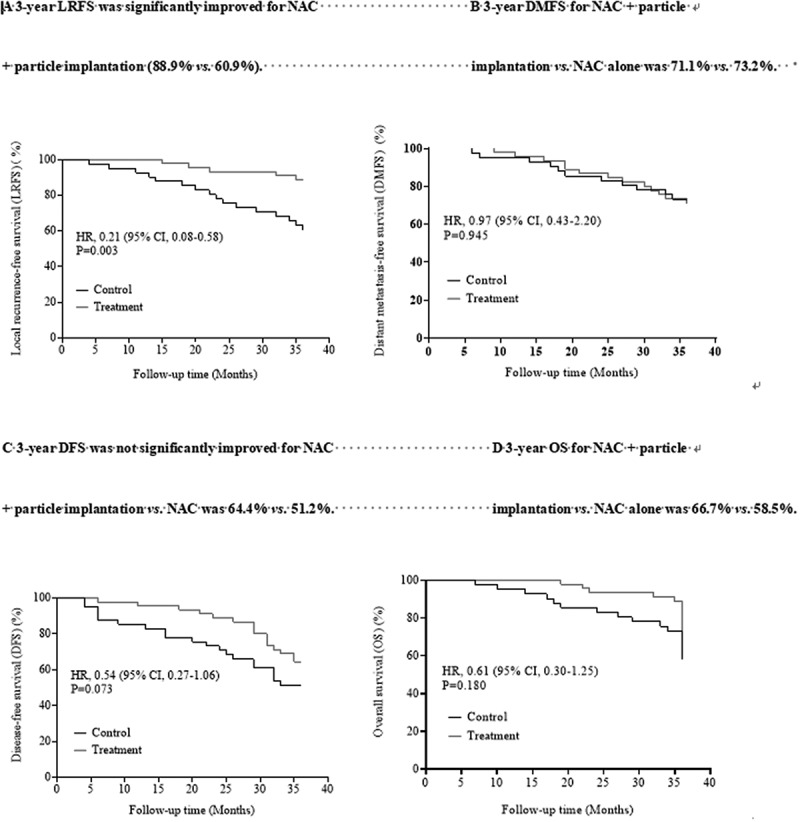 Figure 2
Figure 2- —Key Research and Development Program of Shanxi Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Urinary and Genital Oncology Studies · Urological Disorders and Treatments
Introduction
Urothelial carcinoma (UC) is one of the most common malignant tumors in the Urology Department, which includes upper tract urothelial carcinoma (UTUC) and urothelial bladder carcinoma (UBC). The incidence of UC is high, and the majority of the cases are UBC.^1^ The incidence of bladder cancer ranks 9^th^ among all malignant tumors globally; specifically, the incidence ranks 7^th^ in males and is <10^th^ in females. The mortality rate of bladder cancer ranks 13^th^ among all malignant tumors.^2^ According to the stages, primary bladder cancers can be classified into non-muscle-invasive bladder cancer (NMIBC) and muscle-invasive bladder cancer. Cisplatinum-based neoadjuvant chemotherapy (NAC), followed by radical cystectomy (RC) + pelvic lymph node dissection, has been the standard treatment for patients with MIBC for >10 y, which improves the survival rate of patients and prevents local recurrence and distal metastases.^3–5^ Recent studies have shown evolving treatment trends for muscle-invasive bladder cancer, such as in Germany from 2006 to 2019, reflecting advancements and changes in clinical practices.^6^ However, tumor recurrence at the surgical site in the pelvic cavity could occur in approximately 30% patients with locally advanced (T_3_-T_4_) UBC.^7–11^ Moreover, the local recurrence is associated with low cancer-specific survival,^12,13^ which exhibits poor effects of salvage treatment,^9,11–14^ and the median survival is only about 9 months.^9,15^ The clinical trials have shown that NAC reduces the risk of locoregional recurrence,^16^ significantly improves the disease-free survival (DFS),^17,18^ and thus might prolong the survival.
Comparing to conventional radiotherapy, brachytherapy (interstitial implantation of radioactive particles) has definite treatment efficacy and limited side effects in the treatment of solid tumors and hence has already been widely utilized. Hitherto, only a few studies are available on the treatment of UBC by brachytherapy. Therefore, the present study retrospectively analyzed the clinical data of 86 patients with locally advanced (stage T_3_-T_4_) UBC that underwent brachytherapy+ NAC or NAC. Also, the effectiveness and safety of the regimen of brachytherapy + NAC were assessed. This study is a part of a series of studies on the interstitial implantation of radioactive particles for the treatment of UC.^19^
Materials and methods
Clinical data
A total of 86 patients with locally advanced (stage T_3_-T_4_) UBC, according to the TNM staging criteria (8^th^ edition) issued by the Union for International Cancer Control (UICC), were treated in the Department of Urology Surgery, Shanxi Provincial Cancer Hospital between January 2015 and June 2019 were included. The patients were categorized according to the treatments into two groups, i.e. the study group that underwent brachytherapy + NAC and the control group that received only NAC. The Shanxi Provincial Cancer Hospital has been qualified for brachytherapy for the treatment of solid tumors (including UC) in 2001. The study was approved by the Ethics Committee of the hospital and met the requirements of the Standards of Technical Management for Treatment by Radioactive Particle Implantation (2017 edition) (GUOWEIBANYIFA [2017]). Patients in both groups completed four cycles of NAC by the gemcitabine + cisplatin (GC) regimen before the operation. Finally, among 45 patients in the study group, including 30 (66.7%) males and 15 (33.3%) females, with a median age of 62.7 (range: 46–75) y, 9 (20.0%) presented local lymph node metastasis in the pelvic cavity. A total of 41 (65.9%) patients comprised the control group, including 27 (65.9%) males and 14 (34.1%) females, with a median age of 64.1 (47–75) y; of these 8 (19.5%) had local lymph node metastasis in the pelvic cavity. The baseline clinical data of the patients in the two groups did not differ significantly (all p > .05; Table 1).Table 1.Comparison of clinical data between the two groups.Clinical characteristicsControl group (n = 41)Study group (n = 45)χ^2^PAge (years) 00.992≤6021 (51.22)23 (51.11) >6020 (48.78)22 (48.89) Tumor diameter (cm) 0.9850.321<413 (31.71)10 (22.22) ≥428 (68.29)35 (77.78) Pathology 0.0950.758High-grade33 (80.49)35 (77.78) Low-grade8 (19.51)10 (22.22) TNM 0.5610.454T330 (73.17)36 (80) T411 (26.83)9 (20) Lymph node metastasis 0.0030.955N033 (80.49)36 (80) N1-N28 (19.51)9 (20)
The inclusion criteria were as follows: (1) clinical stage of ≥ cT_3_ or N_1_-N_2_; (2) ECOG score of 0–1 point; (3) without distal metastasis before NAC; (4) underwent RC + pelvic lymph node dissection; (5) signed informed consent. The exclusion criteria were as follows: (1) postoperative pathological findings showed < pT_3_; (2) did not complete preoperative NAC.
Patients in both groups underwent radical cystectomy (RC) + pelvic lymph node dissection. We expected to remove at least 10–12 lymph nodes for accurate staging. However, due to the high proportion of late-stage patients, the difficulty of surgery, and considerations for patient safety and quality of life, on average, only four lymph nodes were targeted during the procedures, and the maximal size of the lymph nodes targeted was 12 cm.
Preoperative preparations
Radioactive iodine [^125^I] sealed source (referred to as particles) consisted of central silver bars and imported high-purity titanium tubes. The dimensions of the central silver bar were as follows: diameter 0.5 mm, length 4.5 mm, and thickness 0.55 mm. The iodine [^125^I] has a half-life of 59.43 d and a half-value layer of 0.025 mmPb, which generates γ-rays with the initial dose rate of 7 cGy/h capable of permeating 1.7-cm-thick tissues. The radioactive activities of the single particles vary in the range of 0.1–6.0 mCi. The particles used in this study were produced by Seeds Biological Pharmacy (Tianjin) Ltd.
Cranial, thoracic, and abdominal CT scanning assessed the presence of distal metastases. Imaging examinations, such as pelvic magnetic resonance imaging (MRI), were performed to assess peribladder adipose tissue invasion, pelvic lymph node enlargement, and the clinical stages. Patients with the clinical stages of T_3_-T_4_ received three cycles of NAC before preoperative preparations for brachytherapy. The three-dimensional (3D) visual stereoscopic imaging was performed to reconstruct the bladder tumor and suspected pelvic lymph node metastatic tumor and acquire the tumor-relevant information, such as site, size, shape, and correlation with adjacent viscera. During the operation, RC + pelvic lymph node dissection was performed, and the region surrounding the bladder tumor and pelvic lymph nodes was defined as the tumor bed, which could be residual lesions, i.e. sub-region of the tumor, and deemed as the target region of radiotherapy. The matched peripheral dose, i.e. the peripheral dose of the tumor, was selected as the dose for the target region. The radiation dose for UC was 70–75 Gy, the radiation dose for lymph node metastasis was 50–60 Gy, and the targeting dose was approximately 1/5–1/4 of the dose of radiotherapy for tumors. Therefore, the radiation dose was 14–18 Gy for tumor bed of bladder tumor and 10–15 Gy for tumor bed of lymph node metastases. Particles with the radioactive activity of 0.5 mCi were selected for therapy. The interval between two particles in the arrangement was 1 cm, and the equivalent radioactivity at 0.5 cm between two particles was 4285 cGy; at least four to six particles were implanted in the target region. The normal tissues have far higher radiation tolerance doses than the dose of radiotherapy for tumors.
Surgical methods
Patients in both groups underwent RC + pelvic lymph node dissection. The preoperative preparations in both groups included routine preparations and deciding on the particle implantation plan. During the operation, particle implantation needles were inserted into the tumor bed under the guidance of ultrasound or direct vision, with the interval of 0.5–1.0 cm between the needles and the vertical depth of insertion <1.0 cm; then one particle was implanted at this site. The >2.0-cm implant gun was used to implant two particles with the vertical interval of 1 cm in the backward mode. The particle implantation was performed carefully to avoid injuries to major blood vessels. After the implantation, local compression was performed, followed by hemostasis and fixation of the particles. A self-designed biogel (biological glue) particle blockchain suturing method was used and was employed for the tumor bed on the tissues surrounding the blood vessels, nerves, and the local pelvic wall, which was then wrapped by the surrounding adipose and connective tissues and sutured to fix the particles. The self-designed biogel particle blockchain was as follows: after intraoperative radiation protection was effectuated, one particle was vertically implanted by the implant gun, followed by four to six particles implanted sequentially with the interval of 1 cm on a gelatin sponge. The biogel was applied to the surface of the gelatin sponge, which was wrapped by a hemostatic gauze and sutured for fixation.
Preoperative NAC
Before NAC, cystoscopy was performed, and the lesion was proven as UC by biopsy and pathological examination. Then, neoadjuvant GC chemotherapy was administered as follows: intravenous injection of gemcitabine 100 mg/m^2^ on d 1 and 8, and intravenous injection of cisplatin 70 mg/m^2^ on d 2. A 3-week treatment was considered one cycle, and all patients were treated for four cycles. Surgery was performed 3–4 weeks after the NAC was completed. Blood routine, urine routine, liver function, renal function, and electrocardiography (ECG) were conducted 1 d before chemotherapy and 1, 8, and 14 d after chemotherapy. Complications and adverse events were detected and treated promptly.
Follow-up
Plain computed tomography (CT) scanning of the target regions of particle implantation was performed on d 3–5 after the operation in the study group to examine the particle number and shifting. The adverse events were assessed during and 2 weeks after chemotherapy. The complications of particle implantation were assessed 1 week to 1 month as well as 3 months after the operation. The blood and urinary routine, blood biochemistry, ECG, thoracic X-ray, and abdominal color ultrasound were reexamined in both groups, and thoracic and abdominal CT scanning was performed if necessary.
Efficacy and adverse event assessment
The primary endpoint of this study was the 3-y locoregional recurrence-free survival (LRFS). The secondary endpoints included 3-y distant metastasis-free survival (DMFS), disease-free survival (DFS), and overall survival (OS). The safety endpoint was the incidence of short- and long-term adverse events.
LRFS was defined as the time from treatment completion to the appearance of recurrent lesions in the pelvic cavity (lesions of internal/external iliac lymph nodes, obturator lymph nodes, anterior sacral lymph nodes, cystectomy bed, and lateral pelvic wall) within 30 d after the first discovery of distal metastases. DMFS was defined as the time from treatment completion to the discovery of extrapelvic metastases (including lymph nodes outside the true pelvis and viscera). DFS was defined as the time from treatment completion to local recurrence of tumor, distal metastases, or death due to tumor progression. OS was defined as the time from treatment completion to the death of the patient. Adverse events were assessed by the World Health Organization (WHO) classification criteria. The adverse events after treatment were defined as the adverse events from the start of chemotherapy to 2 weeks after one cycle of completed chemotherapy, from 1 week after the operation to 1 month after particle implantation, and within 3 months after the treatment. The LRFS rate, DMFS rate, DFS rate, OS rate, and short- and long-term incidence of adverse events were compared between the two groups. The adverse events of chemotherapy were assessed according to the WHO criteria for adverse events of chemotherapy (1997 edition).
Statistical analysis
SPSS 26.0 software was used for statistical analysis. Median (range) and frequency (%) were used to describe the quantitative and qualitative data, respectively. Continuous data were described by median (range) and compared by Mann–Whitney U test. Categorical data were described by frequency (%) and compared using chi-square test. Kaplan–Meier method was used to estimate LRFS, DMFS, DFS, and OS, which were analyzed by log-rank test. Multivariate Cox regression was used to assess the independent predictors of LRFS, DFS, DMFS, and OS. p < .05 was considered statistically significant.
Results
Approximately 30–48 particles were implanted in the patients in the study group, and the mean number of particles was 36. A total of 36 and 9 patients in the study group and 30 and 11 patients in the control group presented stage T_3_ and T_4_ tumors, respectively. In addition, nine and eight patients in the study and control groups exhibited local lymph node metastases, respectively. The median follow-up time of the patients in the two groups was 32.5 (9–42) months. The 3-y LRFS, DMFS, DFS, and OS after the operation were assessed in both groups. The 3-y LRFS was 88.9% (40/45) and 60.9% (25/41) in the study and control groups, respectively, and the difference between the two groups was statistically significant (hazard ratio (HR) 0.210, 95% confidence interval (CI): 0.08–0.58, p = .003). The 3-y DMFS was 71.1% (32/45) and 73.2% (30/41) in the study and control groups, respectively, and the difference was not significantly different (HR 0.97, 95% CI: 0.43–2.20, p = .945). The 3-y DFS was 64.4% (29/45) and 51.2% (21/41) in the study and control groups, respectively, and the difference between the two groups was not statistically significant (HR 0.54, 95% CI: 0.27–1.06, p = .073). The 3-y OS was 66.7% (30/45) and 58.5% (24/41) in the study and control groups, respectively, and the difference was not statistically significant (HR 0.61, 95% CI: 0.30–1.25, p = .180). The Kaplan–Meier survival curves of the study and control groups are shown in Figure 1. Figure 1.Comparison of Kaplan–Meier survival curves of patients with locally advanced UC in the study group (particle implantation + NAC) vs. control group (NAC).
The multivariate regression showed that brachytherapy + NAC was a significant predictor of LRFS (HR 0.210, 95% CI: 0.08–0.58, p = .003). Other factors, such as age, tumor size, tumor types, pathological stages, and lymph node metastases, could not predict LRFS. Local lymph node metastases are associated with local recurrence. Therefore, although lymph node metastasis was not a statistically significant covariate, it was still included as an adjustment factor and could be a marginal predictor of LRFS (HR 2.54, 95% CI: 0.92–7.00, p = .073; Table 2). Multivariate regression analysis did not find any significant predictor of DMFS in this study. The 3-y DMFS was not significantly different between the brachytherapy + NAC group (71.1%; 32/45) and NAC group (73.2%; 30/41) (HR 0.97, 95% CI: 0.43–2.20, p = .945). Lymph node metastases were a significant independent predictor of DMFS (HR 2.48, 95% CI: 1.01–6.13, p = .048; Table 2). Multivariate regression did not find any significant predictor of DFS in this study. Moreover, the 3-y DFS was not significantly different between the brachytherapy + NAC group (64.4%; 29/45) and NAC group (51.2%; 21/41) (HR 0.54, 95% CI: 0.27–1.06, p = .073). However, particle implantation + NAC and lymph node metastases could be marginal predictors of DFS (HR 2.17, 95% CI: 0.97–4.89, p = .061; Table 2). Multivariate regression did not find any significant predictor of OS in this study. The 3-y OS was not significantly different between the brachytherapy + NAC group (66.7%; 30/45) and the neoadjuvant chemotherapy group (58.5%; 24/41) (HR 0.61, 95% CI: 0.30–1.25, p = .180); however, particle implantation + NAC and lymph node metastases were marginal predictors (HR 2.25, 95% CI: 0.99–5.1, p = .052; Table 2).Table 2.Multivariate Cox regression analysis: LRFS, DFS, DMFS, and OS.VariableHRPLRFS Operation0.210 (0.08–0.58)0.003Age0.49 (0.19–1.23)0.127Tumor diameter0.61 (0.25–1.49)0.282Pathology1.39 (0.5–3.83)0.527TNM1.09 (0.38–3.12)0.867Lymph node metastases2.54 (0.92–7.00)0.073DFS Operation0.54 (0.27–1.06)0.073Age0.67 (0.34–1.31)0.239Tumor diameter0.74 (0.36–1.5)0.402Pathology0.99 (0.43–2.26)0.972TNM1.15 (0.53–2.47)0.730Lymph node metastases2.17 (0.97–4.89)0.061DMFS Operation0.97 (0.43–2.20)0.945Age0.73 (0.32–1.65)0.442Tumor diameter0.56 (0.24–1.3)0.176Pathology1.53 (0.61–3.81)0.363TNM1.32 (0.52–3.4)0.56Lymph node metastases2.48 (1.01–6.13)0.048OS Operation0.61 (0.30–1.25)0.180Age0.69 (0.34–1.41)0.309Tumor diameter0.63 (0.3–1.32)0.220Pathology1.08 (0.45–2.59)0.856TNM1.28 (0.59–2.81)0.532Lymph node metastases2.25 (0.99–5.1)0.052
Assessment of adverse events: Local particle shifting was detected in three patients in the study group at 1 week to 1 month after the operation (criteria of local particle shifting: findings of abdominal and pelvic plain CT scanning 1 d after operation were compared to those of abdominal and pelvic plain CT scanning at 1 week to 1 month after the operation), while no related complications occurred. Also, no intestinal canal or blood vessel damage was detected, but other complications of particle implantation, such as no poor incision union, were observed. The incidence of particle implantation-related adverse events, such as bearing down sensation, was significantly higher in the study group than in the control group (p < .01); most of these events were grade 1–2. Patients in both groups completed the GC chemotherapy, and the adverse events were assessed. Blood events (anemia, leukocytopenia, and thrombocytopenia), liver and renal dysfunction, vomiting, diarrhea, and weakness were the major adverse reactions, which were alleviated after symptomatic treatments. The results of the incidence of adverse events in the two groups are shown in Table 3.Table 3.Comparison of adverse events in UC patients between the study and control groups [n (%)].Adverse eventStudy group (n = 45)Control group (n = 41)P value Grade 1-2Grade 3-4Grade 1-2Grade 3-4 Anemia24 (53.3)13 (28.9)20 (48.8)5 (12.2)0.532Leukocytopenia35 (77.8)4 (8.8)30 (73.1)3 (7.3)0.132Thrombocytopenia36 (80.0)6 (13.3)30 (73.3)5 (12.2)0.346Liver dysfunction11 (24.4)0 (0)14 (29.3)0 (0)0.165Renal dysfunction16 (35.5)2 (4.4)12 (29.2)0 (0)0.361Malignant vomit28 (62.2)17 (37.8)22 (53.7)14 (34.1)0.532Diarrhea21 (46.7)7 (15.6)8 (19.5)3 (7.3)0.062Weakness31 (68.9)5 (11.1)20 (48.8)1 (2.4)0.072Bearing down sensation2 (4.4)0 (0)0 (0)0.00215 (33.3)
Discussion
Pathological stage is the major influencing factor of the prognosis of UBC patients after RC; the 5-y OS is <40% for patients with locally advanced UBC (T_3_-T_4_)^8^ and is about 30% for patients with positive lymph nodes.^20^ How to improve the postoperative survival of patients with locally advanced UBC (T_3_-T_4_) has been a clinical research hotspot. Several studies have demonstrated that Platinum-based combination NAC has a high response rate for bladder cancer. Platinum-based NAC in combination with RC + pelvic lymph node dissection is the standard treatment for MBIC in clinical practice.^21–24^ NAC improves the survival by about 5–10% and reduces the risk of death by 16–33% compared to patients who underwent only RC.^24–28^ In this study, all 86 patients with stage T_3_-T_4_ UBC underwent NAC in combination with RC + pelvic lymph node dissection.
Local recurrence after operation for pT_3_-T_4_ UBC significantly influences the treatment effects, which is associated with the low cancer-specific survival.^12,13^ For such patients, the effects of salvage treatment are poor,^9,11–14^ and the median survival was only about 9 months.^9,15^ Various retrospective studies on surgical treatments have demonstrated^29^ that although no lymph node metastases were detected by postoperative pathological examinations, extensive lymph node dissection could improve the survival rate. These findings indicated that preoperative NAC + intraoperative radioactive particle implantation could clear the hidden lymph node micro-metastases to reduce the local recurrence and distal metastases and consequently improve the survival of patients. The findings of clinical studies have demonstrated that NAC reduces the risk of local recurrence. Compared to adjuvant chemotherapy alone, radical cystectomy + chemoradiotherapy significantly improves the DFS and might prolong the OS.^16–18,30^ Zaghloul et al.^31^ provided adjuvant chemoradiotherapy for patients with locally advanced bladder cancer who underwent RC and compared the findings with patients who received only adjuvant chemotherapy. The results showed that patients had a high tolerance to adjuvant chemotherapy + radiotherapy, which significantly improved the LRFS and prolonged the DFS compared to patients who received only chemotherapy.
Since vital viscera, such as the small intestine in the abdominal and pelvic cavities, have a low tolerance to routine external radiotherapy, it is not recommended to apply the high dose external radiotherapy to control severe recurrent bladder cancer as the treatment is in close proximity to such viscera.^32^ Although the adjuvant local treatment did not improve the survival, it prevented the local recurrence in the pelvis; the recurrence induces local pain, edema of lower limbs due to compression on veins and lymph vessels, and uronephrosis due to ureteral obstruction.^15,33,34^
Compared to conventional external radiotherapy, brachytherapy by implantation of radioactive particles has the following advantages: (1) broader indications and shorter hospital stay; (2) tumor tissues are exposed to low-dose radioactive rays for a prolonged period, which leads to tumor cell apoptosis, while the effects on the cells of normal tissues are low. Therefore, interstitial implantation of radioactive particles for the treatment of malignant tumors has definite treatment effects and low adverse effects and thus has been extensively applied in clinical practice.^35,36^ Several studies have demonstrated the efficacy of brachytherapy in the treatment of urothelial carcinoma. For instance, a study by Zaghloul et al. highlighted the improved locoregional control in muscle-invasive bladder cancer patients who received brachytherapy. Similarly, Cozzarini et al. reported enhanced disease-free survival (DFS) with the use of brachytherapy in combination with radical cystectomy (RC) and neoadjuvant chemotherapy (NAC). These studies underscore the potential of brachytherapy to reduce local recurrence and improve overall survival in patients with bladder cancer.
In addition to its application in bladder cancer, there is growing interest in the use of brachytherapy for upper tract urothelial cancers (UTUC). Xuebing Han et al. conducted a series of studies on the interstitial implantation of radioactive particles for the treatment of UTUC. Their findings suggested that brachytherapy, combined with surgery and chemotherapy, was safe and effective, resulting in lower adverse events and potential overall survival benefits. This indicates that the principles and advantages of brachytherapy in bladder cancer could be translated to the treatment of UTUC. We emphasize on further research and clinical trials to fully establish the efficacy and safety of brachytherapy in the treatment of upper tract urothelial cancers. Continued discoveries in this field can provide additional treatment options for UTUC patients, potentially improving their prognosis and quality of life.
Furthermore, the use of brachytherapy in UTUC offers several advantages over conventional external radiotherapy. The precise delivery of radiation to the tumor site minimizes damage to surrounding healthy tissues, which is particularly important in the anatomically complex regions of the upper urinary tract. The prolonged low-dose exposure characteristic of brachytherapy leads to effective tumor cell apoptosis with fewer side effects.
Given the success observed in bladder cancer and the initial positive outcomes in UTUC, further research and clinical trials are warranted to fully establish the efficacy and safety of brachytherapy in the treatment of upper tract urothelial cancers. Continued exploration in this area could provide additional therapeutic options for patients with UTUC, potentially improving their prognoses and quality of life.
To date, only a few studies have investigated the radiotherapy of locally advanced UC, and the treatment efficacy was not definite. Herein, the clinical observations of 22 patients with locally advanced UC who received treatment of particle implantation and presented good treatment efficacy have been reported.^37^ The findings of this series of studies^19^ showed that implantation of radioactive ^125^I particles in combination with surgery + chemotherapy for the treatment of locally advanced (stage T_3_-T_4_) UTUC has lower adverse events than the treatment with surgery + chemotherapy; also, it was safe and effective and could achieve OS benefits.
A high incidence of local micro-metastases is recorded in patients with locally advanced (T_3_-T_4_) UBC,^38^ and thus LRFS was selected as the primary endpoint in this study. The findings in this study showed that additional intraoperative particle implantation for brachytherapy could significantly improves the LRFS, and the absolute improvement of 3-y LRFS could be about 28% (88.9% vs. 60.9%), and the difference between the study and control groups was statistically significant (HR 0.210, 95% CI: 0.08–0.58, p = .003).
The 3-y DFS was 64.4% (29/45) and 51.2% (21/41) in the two groups, respectively, and the difference was not statistically significant. However, after additional intraoperative particle implantation for brachytherapy was performed, the substantial benefits of the 3-y LRFS converted to the marginal benefits of the 3-y DFS (64.4% vs. 51.2%, p = .073). The 3-y OS was 66.7% (30/45) and 58.5% (24/41) in the two groups, respectively, and the difference was not statistically significant between the two groups.
In this study, examination at 1 week to 1 month after operation in the surgery group showed local particle shifting in three patients, while no related complications were observed. In addition, no damage to the intestinal canal or blood vessels, poor union of incision, or other complications of particle implantation was found. The incidence of particle implantation-related adverse events, such as bearing down sensation, was significantly higher in the study group than in the control group at 3 months after the operation (p < .01); most of these events were grade 1–2. Therefore, the incidence of complications of particle implantation was similar to that reported previously and significantly lower than the adverse events of conventional external radiotherapy.^31,32^
Nevertheless, the present study had some limitations. The sample size of this study was small, and the follow-up time was short. Thus, additional studies with more patients and longer observation times are needed to improve the significance of the series study of interstitial implantation of radioactive particles. Addtionally, the retrospective design inherently carries potential biases, such as selection bias and information bias. Retrospective studies rely on existing records, which may not capture all relevant data consistently. Thirdly, this study was conducted at a single center, which may limit the generalizability of our findings. The patient population and treatment protocols at our institution might differ from those at other centers, potentially affecting the external validity of the results.
Conclusions
In summary, compared to the neoadjuvant chemotherapy alone, intraoperative implantation of radioactive particles + the neoadjuvant chemotherapy for the treatment of patients with locally advanced urothelial bladder carcinoma who underwent radical cystectomy + pelvic lymph node dissection significantly improves the locoregional recurrence-free survival and prolongs the disease-free survival, thus acquiring survival benefits. In addition, the treatment was safe and effective, with only limited adverse events.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel RL, Miller KD, Jemal A. Cancer statistics. CA Cancer J Clin. 2019;69(1):7–8. doi: 10.3322/caac.21551.30620402 · doi ↗ · pubmed ↗
- 2Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi: 10.3322/caac.21834.38572751 · doi ↗ · pubmed ↗
- 3Stein JP, Lieskovsky G, Cote R, Groshen S, Feng A-C, Boyd S, Skinner E, Bochner B, Thangathurai D, Mikhail M, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1054 patients. J Clin Oncol. 2001;19(3):666–675. doi: 10.1200/JCO.2001.19.3.666.11157016 · doi ↗ · pubmed ↗
- 4Stein JP, Quek ML, Skinner DG. Lymphadenectomy fbr invasive bladder cancer: historical perspective and contemporary rationale. BJU Int. 2006;97(2):227–231. doi: 10.1111/j.1464-410X.2006.05896.x.16430618 · doi ↗ · pubmed ↗
- 5Witjes JA, Bruins HM, Cathomas R. European association of urology guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2020 guidelines. Eur Urol. 2020;71. doi: 10.1016/j.eururo.2020.03.055. Apr 29:S 0302- 2838(20)30230-X. Online ahead of print. PMID: 32360052.32360052 · doi ↗ · pubmed ↗
- 6Flegar L, Kraywinkel K, Zacharis A, Aksoy C, Koch R, Eisenmenger N, Groeben C, Huber J. Treatment trends for muscle-invasive bladder cancer in Germany from 2006 to 2019. World J Urot. 2022;40(7):1715–1721. doi: 10.1007/s 00345-022-04017-z.PMC 923700635486177 · doi ↗ · pubmed ↗
- 7Honma I, Masumori N, Sato E, Takayanagi A, Takahashi A, Itoh N, Tamagawa M, Sato M-A, Tsukamoto T. Local recurrence after radical cystectomy for invasive bladder cancer: an analysis of predictive factors. Urology. 2004;64(4):744–748. doi: 10.1016/j.urology.2004.05.003.15491713 · doi ↗ · pubmed ↗
- 8Christodouleas JP, Baumann BC, He J, Hwang W-T, Tucker KN, Bekelman JE, Tangen CM, Lerner SP, Guzzo TJ, Malkowicz SB. Optimizing bladder cancer locoregional failure risk stratification after radical cystectomy using SWOG 8710. Cancer. 2014;120(8):1272–1280. doi: 10.1002/cncr.28544.24390799 · doi ↗ · pubmed ↗