Small airway function in predicting asthma control in preschool children
Liangqin Yi, Yan Zhao, Ziyao Guo, Qinyuan Li, Chunlan Qiu, Jingyi Yang, Sha Liu, Fangjun Liu, Ximing Xu, Zhengxiu Luo

TL;DR
This study found that small airway function can predict asthma control in preschool children, with severe airway hyperresponsiveness and lower lung function measures linked to poor outcomes.
Contribution
The study identifies specific lung function metrics and airway hyperresponsiveness as predictors of short-term asthma control in preschool children.
Findings
Severe airway hyperresponsiveness and decreased FEF50% are significantly associated with poor asthma control in preschool children.
Preschool children with these risk factors face an elevated risk of poor asthma control in the following 2–3 months.
Baseline forced expiratory flow measures were significantly lower in children with poor asthma control.
Abstract
Asthma control in children is often challenging. This retrospective cohort study aimed to investigate the potential contribution of small airway function in predicting asthma control within a 2‐ to 3‐month period following the initial diagnosis in preschool children with asthma. A total of 219 preschool children diagnosed with asthma were enrolled, and their follow‐up was conducted by pediatric pulmonary physicians. Clinical history and lung function results were collected for analysis. To identify risk factors associated with poor asthma control, a multivariable regression model was employed. Sixty‐nine of the patients (31.5%) exhibited poor asthma control. Poor adherence to therapy (14.5% vs. 6.0%, p = 0.038) and the presence of severe airway hyperresponsiveness (AHR) (20.6% vs. 1.6%, p < 0.001) were more prevalent in the group with poor control. Additionally, baseline forced…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
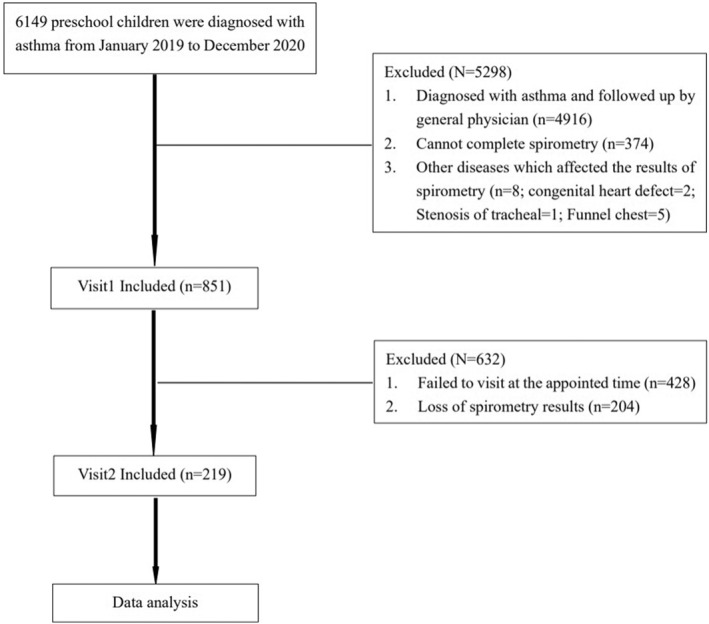 FIGURE 1
FIGURE 1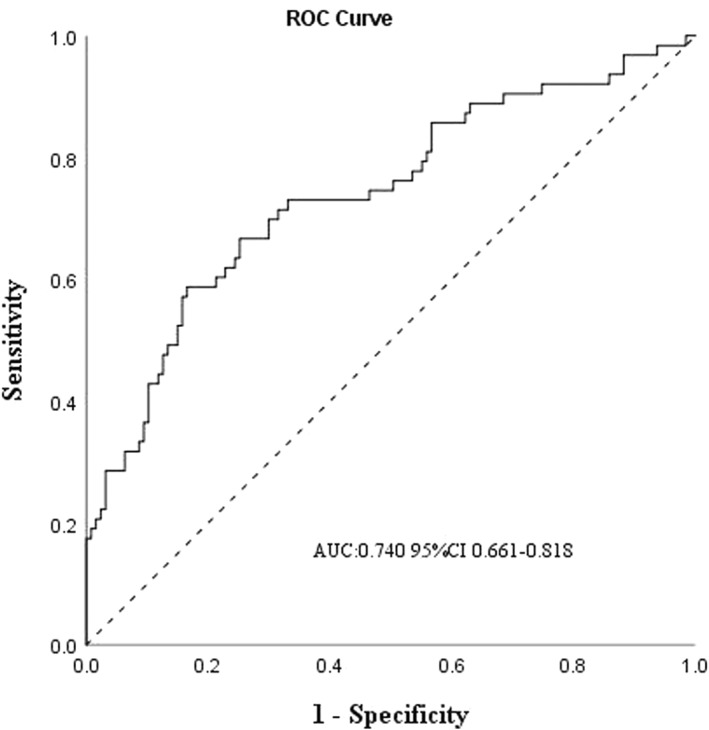 FIGURE 2
FIGURE 2| Total ( | Well‐controlled ( | Poorly‐controlled ( |
| |
|---|---|---|---|---|
| Age of onset (y) | 4.4 (3.9–5.0) | 4.5 (4.0–5.3) | 4.3 (3.9–4.7) | 0.049 |
| Male sex | 127 (58.0%) | 85 (56.7%) | 42 (60.9%) | 0.558 |
| BMI | 15.9 (15.0–16.8) | 15.8 (15.1–16.8) | 15.9 (14.8–16.8) | 0.766 |
| Family asthmatic history | 18 (8.2%) | 15 (10.0%) | 3 (4.3%) | 0.157 |
| Eosinophilia | 53 (24.2%) | 36 (24.0%) | 17 (24.6%) | 0.719 |
| Allergic rhinitis | 110 (50.2%) | 74 (49.3%) | 36 (52.2%) | 0.696 |
| Eczema | 60 (27.4%) | 46 (30.7%) | 14 (20.3%) | 0.110 |
| Atopy | 124 (56.6%) | 85 (56.7%) | 39 (56.5%) | 0.397 |
| AHR | 190 (86.8%) | 127 (84.7%) | 63 (91.3%) | <0.001 |
| Borderline | 16 (7.3%) | 11 (7.3%)† | 5 (7.2%)† | |
| Mild | 64 (29.2%) | 44 (29.3%)† | 20 (29.0%)† | |
| Moderate | 95 (43.4%) | 70 (46.7%)† | 25 (36.2%)‡ | |
| Severe | 15 (6.8%) | 2 (1.3%)† | 13 (18.8%)‡ | |
| LTRAs/ICS | 9/210 | 5/145 | 4/65 | 0.626 |
| Poor adherence to therapy | 19 (8.7%) | 9 (6.0%) | 10 (14.5%) | 0.038 |
| Visit 1 | Visit 2 | |||||
|---|---|---|---|---|---|---|
| Well‐controlled (150) | Poorly‐controlled (69) |
| Well‐controlled (150) | Poorly‐controlled (69) |
| |
| FVC% | 96.7 (87.0–105.3) | 92.4 (83.7–103.5) | 0.093 | 98.2 (90.8–107.1) | 95.3 (86.6–99.7) | 0.009 |
| FEV1% | 101.4 (91.9–109.5) | 94.5 (83.0–104.3) | 0.001 | 104.3 (96.8–112.5)† | 98.0 (91.8–106.3)† | 0.001 |
| FEF50% | 86.0 (67.3–97.4) | 66.1 (54.4–83.4) | <0.001 | 94.3 (74.7–108.9)‡ | 79.6 (65.6–97.6)‡ | 0.001 |
| FEF75% | 75.3 (57.3–92.7) | 60.9 (46.4–83.4) | 0.001 | 85.0 (68.5–103.9)‡ | 69.9 (55.8–95.9)† | <0.001 |
| FEF25–75% | 86.0 (67.2–99.7) | 70.9 (53.9–89.8) | <0.001 | 95.7 (77.0–109.1)‡ | 78.3 (66.3–95.1)† | <0.001 |
| Variables | OR | 95%CI |
|
|---|---|---|---|
| Model 1 | |||
| Age of onset (y) | 0.574 | 0.348–1.946 | 0.129 |
| Adherence | 2.224 | 0.734–6.736 | 0.157 |
| AHR | 0.021 | ||
| Borderline (reference) | |||
| Mild | 0.950 | 0.264–3.418 | |
| Moderate | 0.640 | 0.183–2.242 | |
| Severe | 8.595 | 1.241–59.537 | |
| Baseline FEV1% | 0.995 | 0.961–1.030 | 0.779 |
| Baseline FEF50% | 0.971 | 0.949–0.994 | 0.012 |
| Model 2 | |||
| Age of onset (y) | 0.534 | 0.321–1.889 | 0.116 |
| Adherence | 2.452 | 0.805–7.466 | 0.114 |
| AHR | 0.021 | ||
| Borderline (reference) | |||
| Mild | 0.978 | 0.275–3.475 | |
| Moderate | 0.652 | 0.189–2.251 | |
| Severe | 8.393 | 1.239–56.844 | |
| Baseline FEV1% | 0.983 | 0.952–1.015 | 0.294 |
| Baseline FEF75% | 0.983 | 0.966–1.001 | 0.061 |
| Model 3 | |||
| Age of onset (y) | 0.559 | 0.339–1.921 | 0.123 |
| Adherence | 2.320 | 0.765–7.032 | 0.137 |
| AHR | 0.022 | ||
| Borderline (reference) | |||
| Mild | 0.955 | 0.269–3.395 | |
| Moderate | 0.655 | 0.189–2.263 | |
| Severe | 8.551 | 1.256–58.220 | |
| Baseline FEV1% | 0.988 | 0.954–1.023 | 0.505 |
| Baseline FEF25–75% | 0.979 | 0.958–1.000 | 0.055 |
- —Ministry of Education Key Laboratory of Child Development and Disorders
- —National Clinical Research Center for Child Health and Disorders
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAsthma and respiratory diseases · Chronic Obstructive Pulmonary Disease (COPD) Research · Respiratory and Cough-Related Research
INTRODUCTION
1
Asthma represents a prevalent chronic condition affecting individuals of all age groups worldwide, with preschool children exhibiting the highest prevalence rate.1 While randomized controlled trials have demonstrated the achievability of asthma control,2 real‐world clinical practice frequently falls short in achieving optimal control levels. The prevalence rate of inadequately controlled asthma in children varies significantly ranging from 20% to 60%.3, 4
The evaluation of asthma control in children heavily relies on subjective reports provided by patients and their parents. However, differences in caregivers' comprehension of the disease can lead to over‐ or underestimation of symptoms, resulting in limited correlations between subjective reports and objective measurements.5 Hence, there is a critical necessity to identify dependable markers for assessing asthma control in children.
Forced expiratory volume in 1 s (FEV_1_) serves as the gold standard for clinically evaluating airway obstruction and treatment response.6 However, FEV_1_ primarily reflects large airway obstruction and may not be strongly associated with asthma control, particularly in pediatric patients.7, 8 Growing evidence underscores the pivotal role of small airways in asthma control.9, 10 Studies have indicated that both current symptoms and small airway dysfunction are predictive of future asthma exacerbations.10, 11 Spirometry measurements of forced expiratory flows (FEFs) taken at the mid‐portion of the flow‐volume loops, specifically forced expiratory flow at 50% of forced vital capacity (FVC) (FEF_50_), forced expiratory flow at 75% of FVC (FEF_75_), and forced expiratory flow between 25% and 75% of FVC (FEF_25_ – 75) provide effective means of assessing small airway function. These parameters are considered less dependent on patient effort compared to FEV1.12
Despite the significance of small airway function in forecasting asthma control, there has been a paucity of studies specifically examining its role in pediatric populations. The potential incorporation of small airway function into a comprehensive assessment of pediatric asthma control remains uncertain.6 Consequently, this study aims to explore the relevance of spirometry‐based small airway function measurements in predicting asthma control among preschool children with asthma.
METHODS
2
Patients
2.1
This retrospective cohort study obtained approval from the Institutional Review Board of the Children's Hospital of Chongqing Medical University (File No. [2022] 186). Due to the retrospective nature of the study, the necessity for informed consent was waived.
The study was conducted at the Children's Hospital of Chongqing Medical University, a 2000‐bed tertiary teaching hospital located in Chongqing, China. The research focused on preschool children who received an initial diagnosis of asthma and underwent two consecutive visits with pediatric pulmonologists between January 1, 2019, and December 31, 2020. Patients were included based on the following criteria: (i) age between 3 and 5 years old; (ii) diagnosis of asthma confirmed by at least one pediatric pulmonologist at the Children's Hospital of Chongqing Medical University, following the GINA guidelines (2018)6; (iii) completion of a standard lung function test with technically acceptable flow‐volume curves13; (iv) free from respiratory infections for a minimum of 4 weeks preceding the lung function test. Patients were excluded from the study if they met any of the following criteria: (i) presence of acute and/or chronic diseases that could potentially impact the results of the lung function test (including conditions like bronchopulmonary dysplasia, bronchiectasis, pulmonary tuberculosis, interstitial lung disease, congenital heart disease, severe psychiatric disorders, etc.); (ii) insufficient quality of spirometry data; (iii) lack of medical records for the 2–3 months of the follow‐up period.
Definitions
2.2
According to the GINA guidelines (2018),6 well‐controlled asthma is defined as the absence of the following conditions: (i) experiencing daytime asthma symptoms for more than a few minutes, more than once a week; (ii) encountering any limitations in activities, such as reduced running or playing compared to other children, or experiencing easy fatigue during physical activities due to asthma; (iii) requiring reliever medication more than once a week; (iv) experiencing nighttime awakenings or coughing due to asthma. Partly controlled asthma is defined as meeting 1 to 2 of the aforementioned conditions, and uncontrolled asthma is defined as meeting 3 to 4 of the mentioned conditions. For this study, poorly‐controlled asthma encompasses both partly controlled and uncontrolled asthma.
Children were classified as atopic types if they demonstrated at least one positive response to common aeroallergens (such as house dust mites, cotton, fur, etc.) or food allergens (such as peanut, milk, egg, etc.) during a skin prick test.3 Eosinophilia was defined as a peripheral blood eosinophil count equal to or greater than 0.5 × 10^9^/L with eosinophils constituting at least 5% of leukocytes.14
Poor adherence to therapy was defined as meeting any of the following criteria15: (i) not utilizing a medication controller device, (ii) employing an incorrect inhalation method, and (iii) consuming less than 80% of the prescribed doses.
Lung function
2.3
Spirometry (Masterscreen Pead, Germany JAEGER) was performed following the guidelines set forth by the American Thoracic Society (ATS) and/or the European Respiratory Society (ERS).13 Trained technicians administered the lung function tests within the dedicated laboratory setting. Each test underwent a minimum of three repetitions to ensure the reproducibility of both FVC and FEV_1_. The most successful FVC maneuver out of the three attempts was selected. A qualified investigator meticulously reviewed the volume‐time and flow‐volume tracings, excluding any measurements of subpar quality.
Airway hyperresponsiveness (AHR) was categorized into four degrees based on methacholine concentration (cMch) according to a previously published study16: Borderline AHR: 8 g/L* < cMch ≤16 g/L, Mild AHR: 2 g/L < cMch ≤ 8 g/L, Moderate AHR: 0.5 g/L < *cMch ≤ 2 g/L, Severe AHR: cMch ≤ 0.5 g/L.
Data collection
2.4
The data were obtained through a review of electronic medical databases of the Department of Respiratory Medicine. Two trained researchers independently extracted information from the medical records using a standardized data collection form. In cases where discrepancies arose, a third researcher was consulted for resolution. The following demographic characteristics were gathered: gender, age, weight, height, and body mass index (BMI), along with maternal and paternal histories of asthma, comorbidities (such as allergic rhinitis and eczema), peripheral eosinophil count and proportion, results of the skin prick test, and measurements of FVC, FEV1, FEFs, and cMch at baseline (Visit 1) and follow‐up (Visit 2). All spirometry parameter were expressed as percentages of predicted values (%pred).
Statistical analysis
2.5
The normality of continous variables was evaluated using the Shapiro‐Wilk test. Continuous variables were expressed as median and interquartile range, while categorical variables were presented as frequencies and percentages (%). Disparities in continuous variables between groups were assessed using the non‐parametric Mann‐Whitney U test. The paired Wilcoxon signed‐rank test was employed to analyze differences in continuous variables between the two consecutive visits within each group. Categorical variables were compared using the Chi‐square test supplemented by Fisher's exact test when necessary, and Bonferroni correction was applied to account for multiple comparisons. Interdependencies among variables (FVC%, FEV_1_%, and FEF_S_%) were assessed through collinearity diagnostics and Spearman's correlation analysis. The correlation coefficient |r| < 0.400 indicated a weak correlation, 0.400–0.700 suggested a moderate correlation, and >0.70 indicated a strong correlation.17 The logistic regression model was applied for multivariable analyses to determine independent factors associated with poor asthma control. Variables demonstrating significance with a p‐value <0.050 in univariate analysis were subsequently included in the multivariate logistic regression analysis using the entering selection method. Receiver‐operating characteristic (ROC) curves were constructed to evaluate the predictive performance of the models for asthma control. Independent variables, including age, BMI, FVC%, FEV1%, and FEF_S_%, were considered as continuous variables. Categorical variables, such as a history of allergic rhinitis, eczema, atopy and poor adherence to therapy, were coded as 1 (present) or 0 (not present). AHR was categorized into four degrees and coded as 0 (borderline), 1 (mild), 2 (moderate), and 3 (severe) for the analysis. All data analyses were conducted by IBM SPSS software for Windows (version 26.0 SPSS Inc.), and p‐values less than 0.050 (two‐tailed) were considered statistically significant.
RESULTS
3
Characteristics of children with poor asthma control
3.1
In this retrospective cohort study, a total of 851 preschool children who had confirmed asthma at the initial visit (Visit 1) met the inclusion criteria. Among them, 428 patients did not attend the follow‐up visit within the subsequent 2–3 months (Visit 2), and spirometry data of 204 patients were missing. Consequently, 219 preschool children with asthma were included in the study (see Figure 1). The median age of the participants was 4.4 years. Out of the 219 patients, 150 (68.5%) achieved good asthma control, while 69 (31.5%) experienced poor asthma control. Children in the poorly‐controlled group were slightly younger than those in the well‐controlled group (4.3 years vs. 4.5 years, p = 0.049). The prevalence of poor adherence (14.5% vs. 6.0%, p = 0.038) and severe AHR (20.6% vs. 1.6%, *p < *0.001) were remarkably higher in the poorly‐controlled group than the well‐controlled group. However, there were no statistically significant differences in terms of gender (p = 0.558), BMI (p = 0.766), family history of asthma (p = 0.157), eczema (p = 0.110), allergic rhinitis (p = 0.696), eosinophilia (p = 0.719), atopic status (p = 0.397), and medication management (p = 0.626) between the two groups (Table 1).
Flow diagram of study progression.
Decreased lung function was associated with poor asthma control in preschool children with asthma
3.2
At the baseline, the poorly‐controlled group exhibited significantly lower values for FEV_1_% (94.5 vs. 101.4, p = 0.001), FEF_50_% (66.1 vs. 86.0, *p < *0.001), FEF_75_% (60.9 vs. 75.3, p = 0.001), and FEF_25–75_% (70.9 vs. 86.0, *p < *0.001) compared to the well‐controlled group. However, there was no statistically significant difference in FVC% (92.4 vs. 96.7, p = 0.093) between the two groups. Throughout the study, spanning from visit 1 to visit 2, spirometry parameters, including FEV_1_%, FEF_50_%, FEF_75_%, and FEF_25–75_% exhibited statistically significant improvements in both groups. Nevertheless, the extent of improvement in these spirometry parameters did not differ significantly between the two groups. For detailed data, please refer to Table 2.
Risk factors in predicting poor asthma control in preschool children with asthma
3.3
The univariable analysis revealed that factors, such as the age of onset, adherence, baseline FEV_1_%, FEF_50_%, FEF_75_%, FEF_25–75_%, as well as AHR, were associated with short‐term poor asthma control in preschool children with asthma (*p < *0.050 for each factor, detailed information can be found in Supplement Table 1). Collinearity diagnostics identified interdependencies among these variables, notably a strong correlation between baseline FEF_50_% and FEF_75_% (correlation coefficient: 0.872, p < 0.010) and between baseline FEF_50_% and FEF_25–75_% (correlation coefficient: 0.963, p < 0.010, refering to Supplement Table 2 for detailed information). Given these strong correlations among FEFs, it was advisable to include only one of them in the logistic regression model at a time. Therefore, we conducted three separate multivariate regression models to determine the independent predictors of poor asthma control at visit 2 (Model 1 included age, adherence, AHR, baseline FEV_1_, and baseline FEF_50_%; Model 2 included age, adherence, AHR, baseline FEV_1_, and baseline FEF_75_%; Model 3 included age, adherence, AHR, baseline FEV_1_, and baseline FEF_25–_ 75%. Please refer to Table 3 for details).
The predictive model for poor asthma control in preschool children with asthma over the next 2–3 months revealed that baseline severe AHR (OR 8.595, 95%CI 1.241–59.537, p = 0.029) and decreased FEF_50_% (OR 0.971, 95%CI 0.949–0.994, p = 0.012) were significantly associated with short‐term poor asthma control (Table 3). Preschool children with asthma who had baseline severe AHR were approximately 9 times more likely to experience poor asthma control within the next 2–3 months compared to those with baseline borderline AHR. Additionally, for each unit decrease in baseline FEF_50_%, the odds of future poor asthma control increased by 3% in preschool children with asthma (Table 3). The ROC curve demonstrated that the multivariable model, which included baseline AHR and FEF_50_%, exhibited good predictive ability for poor asthma control in preschool children with asthma (area under the curve: 0.740, 95%CI 0.661–0.818; Figure 2).
ROC of the model in predicting subsequent 2‐ to 3‐months of poorly‐controlled asthma. A model including baseline AHR and FEF50%. AHR, airway hyperresponsiveness; AUC, area under the curve; FEF50%, forced expiratory flow at 50% of forced vital capacity predicting; ROC, receiver‐operating characteristic.
DISCUSSION
4
Our study aimed to investigate the correlation between current clinical status, spirometry parameters, and asthma control in preschool children with asthma over a 2‐ to 3‐month period. The results revealed that severe AHR and a lower FEF_50_% value at the initial visit were significantly linked to poor asthma control during the subsequent 2–3 months.
Recent research has increasingly emphasized the pivotal role of small airways in the pathogenesis of asthma. Studies consistently indicate that inflammatory cell infiltration and airflow limitation predominantly manifest in these smaller airways.18, 19 The persistence of inflammation within these small airways has been identified as a primary contributor to poor asthma control.20 The results of our study align seamlessly with these findings as we have demonstrated that a spirometric parameter reflecting small airway function serves as a significant predictor of future asthma control in preschool children. Notably, our findings corroborate a study conducted by Shi et al.,10 providing additional compelling evidence for the relevance of small airway function in predicting asthma outcomes.
Remarkably, our multivariate analysis uncovered that an initial decrease in FEF_50_% played a significant role in poor asthma control, while the impact of FEV_1_% on asthma control within the model was not as pronounced. Previous studies have reported relatively weak correlations between FEV_1_ and symptoms, respiratory status, and dyspnea in patients with asthma.9 In contrast, small airway function has been associated with nocturnal asthma, heightened asthma symptoms, and exercise‐induced asthma.21 Moreover, airway dysfunction in children with asthma is not uniformly distributed throughout the airways22 with inflammation often being more evident in the small airways than the larger ones.18 The decline in FEFs may be more common in the early stage of childhood before a noticeable decrease in FEV_1_. This suggested that preschool patients with decreased small airway function may be at a heightened risk of asthma exacerbation.8 Furthermore, Turner's study has indicated that FEV_1_ in the majority of preschool children with asthma falls within the normal range, and FEV_1_ may not be sufficiently sensitive for detecting abnormalities in asymptomatic individuals.7 In our study, despite a significant improvement in spirometry parameters, including FEV_1_% >80%, in the poorly‐controlled group's following treatment, varying degrees of impairment in small airway function persisted. This highlights the limited capacity of FEV_1_ to effectively gauge asthma control and airflow limitation in preschool children. Conversely, small airway function parameters demonstrate greater reliability in reflecting airway dysfunction and predicting poor asthma control. In contrast, FEV_1_ and FEFs have shown a significant association with the Asthma Control Questionnaire in adults.9 This difference may be attributed to increased asthma duration, the persistence of airway inflammation, and airway remodeling occurring in both large and small airways with age, ultimately leading to airflow limitation. Thus, this highlights the importance of considering both large and small airways when assessing asthma control.
In 1975, Dosman's study demonstrated that a decrease in FEF_50_ was a sensitive method for detecting small airway obstruction.23 The validation study of ATS/ERS spirometry guidelines also showed high sensitivity and specificity for FEF_50_ in identifying airway obstruction in 5‐year‐old children with asthma.7 Our results further reinforce the role of decreased baseline FEF_50_% as a risk factor for short‐term poor asthma control. However, the debate surrounding FEF_50_ versus FEF_25–75_ in assessing airway function in asthma, particularly in children, remains unresolved.24, 25 We acknowledge the significant contribution of small airway function to asthma control. However, in our study, we observed that despite these improvements in spirometry parameters, some patients continued to experience poor asthma control. This finding underscored the complexity of asthma and suggested that while spirometry parameters like FEF_50_% were important components of asthma control assessment, they alone may not provide a comprehensive representation of asthma control. Asthma control is influenced by a multitude of factors, and our study highlighted the importance of considering a comprehensive set of clinical and physiological variables when assessing asthma outcomes. As spirometry is a convenient and practical method for evaluating airflow limitation, further studies exploring the impact of FEFs on airway function in preschool children with asthma would be both valuable and necessary, especially in economically disadvantaged areas where more advanced pulmonary function tests, such as impulse oscillometry (IOS), fractional exhaled nitric oxide (FENO), and multiple breath nitrogen washout (MBNW), may not be readily available.
Contrary to other studies,26, 27 our study did not identify a significant relationship between rhinitis, eczema, family asthmatic history, and short‐term asthma control in preschool children with asthma. These discrepancies may be attributed to variations in the study population, sample size, and follow‐up periods. Results on adherence were also found to be heterogeneous,27, 28 potentially due to the relatively brief follow‐up period or improvements in lung function resulting from treatment, which may overshadow the influence of adherence on asthma control. Nonetheless, emphasizing good adherence remains crucial for achieving optimal asthma control.
AHR is a fundamental component of asthma pathophysiology6 and is closely linked to heightened airway inflammation.29 Evidence suggests that asymptomatic AHR in the general population serves as an important risk factor for the subsequent development of wheezing or asthma.30 Furthermore, severe AHR in infancy has been identified as a predictor of asthma development in adulthood.31 Our study further underscored the significance of severe AHR as a risk factor for future poor asthma control, emphasizing its potential as a predictor of asthma outcomes. Nevertheless, additional research is needed to confirm the relevance of AHR in the development of asthma.
In summary, our study revealed that initial severe AHR and decreased FEF_50_ are associated with short‐term poor asthma control in preschool children. By incorporating these indicators into routine assessments, healthcare providers can identify high‐risk individuals who may require personalized treatments. This approach holds the potential to optimize asthma control and reduce the likelihood of exacerbations.32, 33 The regular monitoring of AHR and FEF50 may aid in the early identification of asthma in preschool children who are at risk of poor asthma control, enabling the timely implementation of tailored treatments. Additionally, advancements in technology may lead to the development of portable monitoring devices, such as home electronic peak flowmeters, which could broaden the application of these indicators in various settings. This, in turn, would provide clearer guidance to parents and caregivers regarding medication use, trigger avoidance, and the prompt recognition of worsening symptoms. Furthermore, ongoing research endeavors are essential for enhancing the utilization of non‐invasive tests, ultimately improving the care and outcomes for preschool children with asthma.
Strength and limitation
4.1
Our study has provided valuable insights into the relationship between small airway function and asthma control in preschool children, specifically highlighting the association between decreased small airway function and poor asthma control in the 2–3 months following the initial diagnosis. However, we must acknowledge several limitations. First, there was a potential risk of collinearity between FEV_1_% and the FEFs%, which may weaken the statistical analysis. Although we addressed multicollinearity through residual analysis and conducted sensitivity analysis (see Supplement Tables S3–S7), caution is warranted when comparing the predictive value of FEV_1_ and the FEFs in assessing asthma control. Second, due to the overlap of the COVID‐19 pandemic with our study period, a significant number of patients were lost to follow‐up, and the follow‐up duration was relatively short, which could pose challenges in interpreting certain results. Additionally, the retrospective design and relatively small sample size may limit the generalizability of our findings. Therefore, further prospective studies with larger cohorts are necessary to validate these results. Furthermore, the 2‐ to 3‐month follow‐up period may not capture longer‐term asthma control outcomes, necessitating future research to investigate the predictive value of these factors over an extended follow‐up duration. Moreover, our study exclusively focused on spirometry parameters when assessing the correlation between small airway function and asthma control without considering other pulmonary function tests, such as IOS, FENO, and MBNW. Given the varying sensitivity of different methods, combining multiple techniques to assess small airway function may offer additional information for predicting asthma control. Lastly, in our study cohort, some preschool children with poor asthma control continued to exhibit small airway dysfunction despite receiving standard therapy. Further research is required to determine the prognostic role of persistent small airway dysfunction in asthma.
CONCLUSION
5
The study aimed to identify factors associated with asthma control in preschool children with asthma, providing valuable predictive information for poor asthma control. The results indicate that preschool children with asthma who have initial severe AHR and/or decreased FEF_50_ are at an elevated risk of experiencing poor asthma control over the subsequent 2–3 months. These findings underscore the importance of assessing small airway function in predicting asthma control and suggest that improving small airway function may be advantageous for managing asthma in this age group. Further research is essential to confirm these results and investigate additional factors that could impact asthma control in preschool children.
AUTHOR CONTRIBUTIONS
Zhengxiu Luo: Conceptualization; supervision; writing—review and editing. Liangqin Yi: Conceptualization; data curation; methodology; formal analysis; writing—original draft preparation. Yan Zhao: Methodology; writing—review & editing. Ziyao Guo: Writing—review and editing. Qinyuan Li: Formal analysis; writing—review and editing. Chunlan Qiu: Investigation. Jingyi Yang: Investigation. Sha Liu: Data curation; investigation. Fangjun Liu: Data curation; investigation. Ximing Xu: Formal analysis; writing—review and editing.
CONFLICT OF INTEREST STATEMENT
All authors declare they have no competing interests.
ETHICS STATEMENT
This study was approved by the Institutional Review Board of the Children's Hospital of Chongqing Medical University (File No. [2022] 186). The requirement of obtaining informed consent was waived due to the retrospective design of the study.
CONSENT TO PARTICIPATE
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
Supporting information
Table S1–S7
Table S8
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Report A . Premium Times. November 1, 2022. Accessed May 5, 2021. https://www.premiumtimesng.com/news/top‐news/459514‐world‐asthma‐day‐339‐million‐people‐affected‐globally‐expert.html#.Y 2px Apb QSC 4.link
- 2Bateman ED , Boushey HF , Bousquet J , et al. Can guideline‐defined asthma control be achieved? The Gaining Optimal Asthma Control study. Am J Respir Crit Care Med. 2004;170(8), 836‐844.15256389 10.1164/rccm.200401-033OC · doi ↗ · pubmed ↗
- 3Papwijitsil R , Pacharn P , Areegarnlert N , et al. Risk factors associated with poor controlled pediatric asthma in a university hospital. Asian Pac J Allergy Immunol. 2013;31(3):253.24053709 · pubmed ↗
- 4Bao Y , Chen Z , Liu E , Xiang L , Zhao D , Hong J . Risk factors in preschool children for predicting asthma during the preschool age and the early school age: a systematic review and meta‐analysis. Curr Allergy Asthma Rep. 2017;17(12):85.10.1007/s 11882-017-0753-729151195 · doi ↗ · pubmed ↗
- 5Green RJ , Klein M , Becker P , et al. Disagreement among common measures of asthma control in children. Chest. 2013;143(1):117‐122.22878380 10.1378/chest.12-1070 · doi ↗ · pubmed ↗
- 6Asthma G If . Global Strategy for Asthma Management and Prevention. 2018. www.ginasthma.org
- 7Turner SW , Craig LC , Harbour PJ , et al. Spirometry in 5‐year‐olds—validation of current guidelines and the relation with asthma. Pediatr Pulmonol. 2007;42(12):1144‐1151.17968994 10.1002/ppul.20709 · doi ↗ · pubmed ↗
- 8Mc Fadden E Jr. , Linden DA . A reduction in maximum mid‐expiratory flow rate. A spirographic manifestation of small airway disease. Am J Med. 1972;52(6):725‐737.5030170 10.1016/0002-9343(72)90078-2 · doi ↗ · pubmed ↗