Rare metastasis of renal cell carcinoma to the breast: a case report
Aman Saswat Sahoo, Bhuvi Singh, Monther Salman, Lilia Ragad, Rasheed Elayyan

TL;DR
A rare case of kidney cancer spreading to the breast six years after treatment is reported, emphasizing the need for careful diagnosis and further research.
Contribution
This case report documents a rare metastasis of renal cell carcinoma to the breast and emphasizes diagnostic considerations.
Findings
A 54-year-old woman with a history of renal cell carcinoma developed a breast metastasis six years after surgery.
Histopathology and immunohistochemistry confirmed the metastasis, avoiding unnecessary axillary surgery.
The case underscores the importance of distinguishing between primary and metastatic breast neoplasms in cancer survivors.
Abstract
Renal cell carcinoma is an aggressive urological malignancy, accounting for 2%–3% of adult cancers and over 90% of renal cancers. While renal cell carcinoma commonly metastasizes to organs such as the lungs, bones, and liver, breast metastasis is rare, comprising only 0.5% to 2% of all breast neoplasms. This case report describes a 54-year-old female with a history of RCC who developed a metastatic lesion in her breast six years after radical nephrectomy. The lesion, initially detected via routine imaging, was confirmed as renal cell carcinoma through histopathology and immunohistochemistry. A wide local excision was performed, avoiding unnecessary axillary surgery. This case highlights the need for meticulous diagnostic evaluation to distinguish between primary breast carcinoma and metastatic disease, particularly in patients with a history of renal cell carcinoma. The rarity of renal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
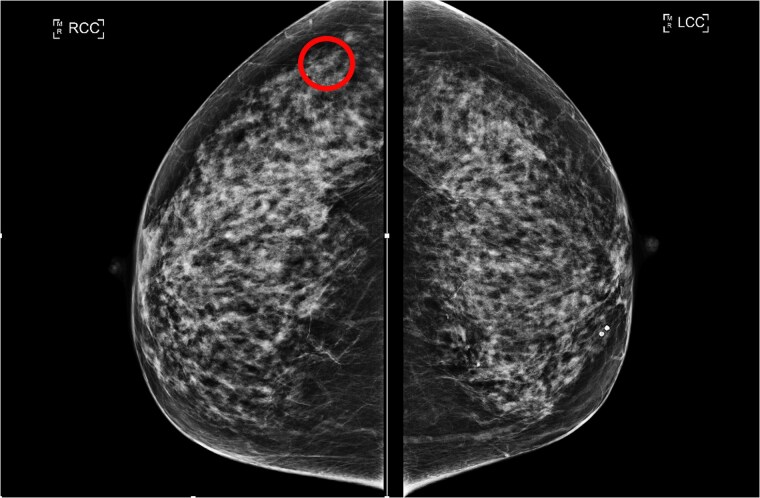 Figure 1
Figure 1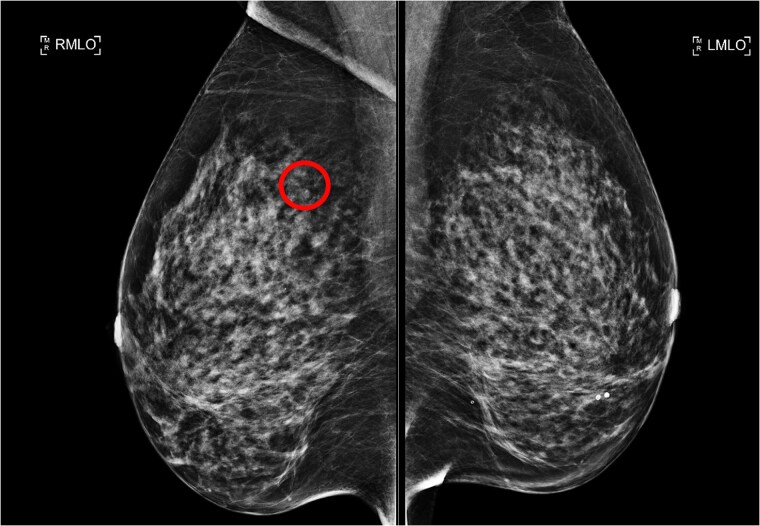 Figure 2
Figure 2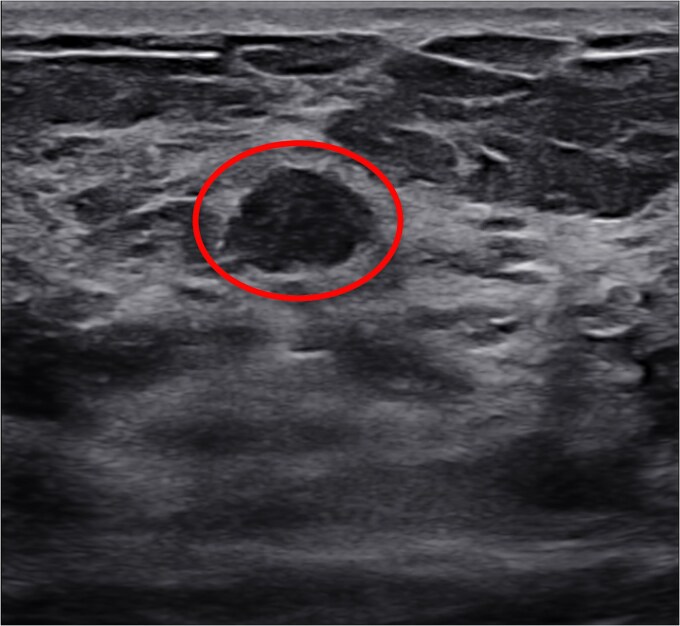 Figure 3
Figure 3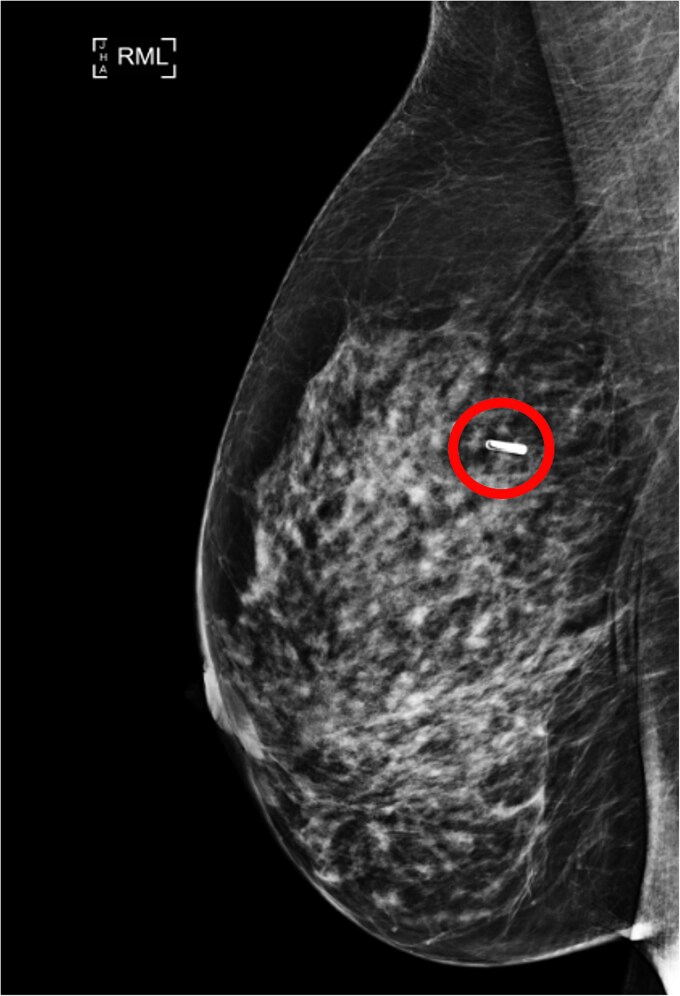 Figure 4
Figure 4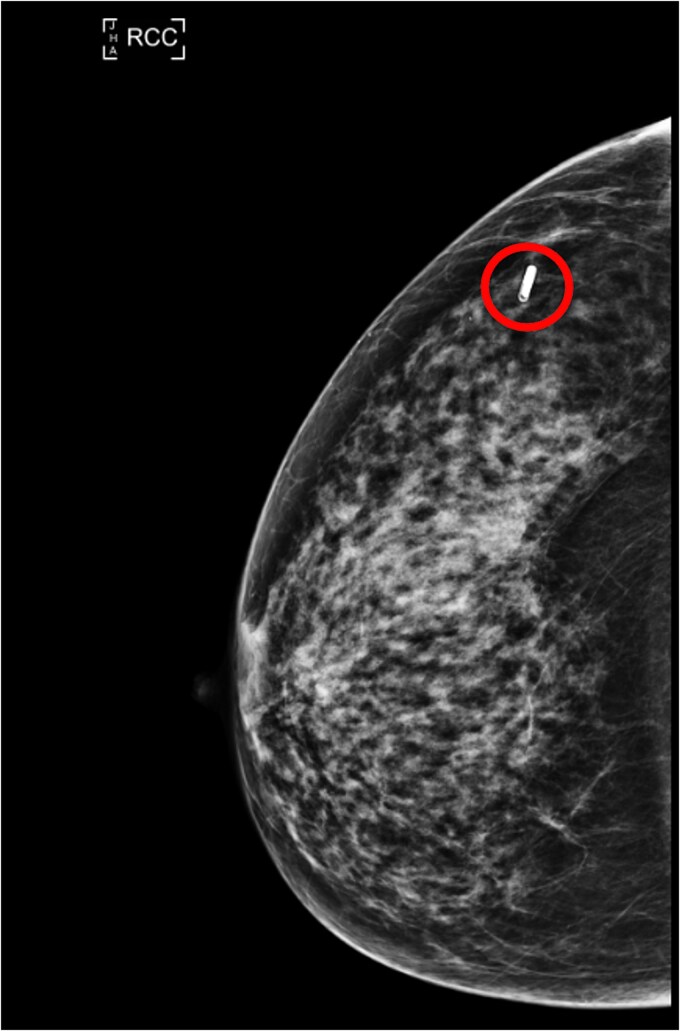 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Cancer Diagnosis and Treatment · Cancer and Skin Lesions
Introduction
Renal cell carcinoma (RCC) is a prevalent and aggressive urological malignancy that accounts for approximately 2%–3% of adult neoplasms and more than 90% of all renal cancers [1]. RCC usually metastasizes to the lungs (70%), bones (42%), lymph nodes (55%), liver (41%), and brain (11%). Metastasis to the breast, however, is a rare phenomenon and accounts for 0.5% to 2% of all breast neoplasms [2].
Breast metastases usually originate from melanoma, lymphoma, or leukaemia making metastasis from RCC an exceptionally rare occurrence [3]. The presence of RCC in the breast indicates widespread dissemination of malignancy. The prognosis of metastatic RCC is generally poor compared to that of localised disease [4, 5]. Due to its rarity the metastasis of RCC to the breast can be overlooked for a primary breast carcinoma, hence necessitating meticulous diagnosis which will avoid extreme surgical interventions such as mastectomy.
We present herein a rare case of a 54-year-old female who presented to us with an RCC metastasis to her breast 6 years after her initial diagnosis.
Case presentation
A 54-year-old female had a history of RCC treated Initially by radical nephrectomy and no chemotherapy.
The patient has had regular computer tomography (CT) imaging since her surgery. 3 years ago, a routine CT identified a 4 mm lesion in the lower outer quadrant of the right breast.
Following this CT scan, a triple assessment has been performed. A clinical examination revealed no palpable abnormalities in both breasts. However, mammography highlighted a 6 mm circumscribed nodule in the posterolateral aspect of the right breast, which was not present in prior imaging 4 years ago (Figs 1 and 2).
RCC (lesion circled) and LCC mammogram of the lesion.
RMLO (lesion circled) and LMLO mammogram of the lesion.
Ultrasound evaluation correlated these findings with a 5 mm benign-appearing nodule (Fig. 3).
Ultrasound scan of the lesion (circled).
Core Biopsy was performed, and histopathological evaluation showed an inflammatory lesion, characterised by cells with clear cytoplasm and macrophages. Keeping in mind the initial known diagnosis; immunohistochemical staining provided crucial diagnostic clarity, with positive results for PAX8, CD10, and MNF116 markers, confirming the presence of metastatic RCC.
The patient was informed of the diagnosis of metastatic RCC to the right breast. Further assessment of distant sites and the potential for systemic therapy were discussed at this stage; however, it was later decided that no systemic interventions would be pursued. While the lesion was considered minor in terms of surgical intervention, its identification was crucial as an indicator of metastatic disease.
A wide local excision was performed after tagging the lesion with a radio frequency identification tag located 3 mm inferior to the original site; no axillary surgery was performed (Figs 4 and 5).
RMLO view of the localiser placement (circled).
RCC view of the localiser (circled).
Post-operative Histopathological evaluation revealed a 5 mM well-circumscribed metastatic renal cell carcinoma. No vascular invasion, ductal carcinoma in situ, or lobular carcinoma in situ was identified.
Discussion
RCC is prominent in its ability to spread hematogenously, yet metastasis to the breast is extremely uncommon [3].
The route for metastasis usually includes the migration of tumour cells from the kidneys through the inferior vena cava to the right ventricle of the heart. From here they enter the pulmonary circulation, and eventually to the breast [6].
Breast metastasis from RCC is exceedingly rare, with fewer than 60 cases documented in the literature. Although the risk of RCC recurrence is highest within the first two years following treatment, metastases to uncommon sites, such as the breast, have been reported even a decade after the initial diagnosis and surgical intervention [7]. Similarly, in our case, the metastasis was identified 8 years after nephrectomy.
Metastatic breast cancer typically presents as a rapidly growing painless firm palpable breast mass. They usually have well-defined or close to well-defined margins and are rounded in shape. Multiple tumours in one breast or bilateral tumours are rarely seen [8].
It is important to differentiate primary disease from secondary metastasis due to overlap in clinical and radiological features. A history of malignancy or co-existing tumour should raise suspicions of a secondary tumour. Differentiating between the two will guide the treatment strategy for individual patients. A triple assessment must be carried out for accurate diagnosis [9].
There are no specific guidelines for the management of RCC metastasis of the breast. Surgical excision is often used when the metastasis is isolated, as is the case with most breast metastasis. Regardless of the primary source, metastasis to the breast is associated with poor outcomes with a mean survival of 10.9 months [10].
The limited information available in the literature regarding optimal treatment strategies and patient outcomes for RCC metastasis to the breast highlights the need for further studies to better understand this condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bahadoram S, Davoodi M, Hassanzadeh S. et al. Renal cell carcinoma: an overview of the epidemiology, diagnosis, and treatment. G Ital Nefrol 2022;39. https://pubmed.ncbi.nlm.nih.gov/35819037/35819037 · pubmed ↗
- 2Falco G, Buggi F, Sanna PA. et al. Breast metastases from a renal cell carcinoma. A case report and review of the literature. Int J Surg Case Rep 2014;5:193–5. 10.1016/j.ijscr.2014.01.01924632302 PMC 3980508 · doi ↗ · pubmed ↗
- 3Mun SH, Ko EY, Han BK. et al. Breast metastases from extramammary malignancies: typical and atypical ultrasound features. Korean J Radiol 2014;15:20–8. 10.3348/kjr.2014.15.1.2024497788 PMC 3909857 · doi ↗ · pubmed ↗
- 4Jonasch E, Gao J, Rathmell WK. Renal cell carcinoma. BMJ 2014;349:g 4797–7. 10.1136/bmj.g 479725385470 PMC 4707715 · doi ↗ · pubmed ↗
- 5Pandey J, Syed W. Renal Cancer. Stat Pearls Publishing: Treasure Island (FL), 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 558975/.32644401 · pubmed ↗
- 6Nagata A, Shinden Y, Nomoto Y. et al. Metastasis of breast cancer to the right kidney with a tumor thrombus in the inferior vena cava: a case report. Surg Case Rep 2022;8:13. 10.1186/s 40792-022-01364-235038044 PMC 8762526 · doi ↗ · pubmed ↗
- 7Elouarith I, Bouhtouri Y, Elmajoudi S. et al. Breast metastasis 18 years after nephrectomy for renal cell carcinoma: a case report. J Surg Case Rep 2022;2022. 10.1093/jscr/rjac 116PMC 907133635530427 · doi ↗ · pubmed ↗
- 8Lee AHS . The histological diagnosis of metastases to the breast from extramammary malignancies. J Clin Pathol 2006;60:1333–41. 10.1136/jcp.2006.046078 PMC 209557618042689 · doi ↗ · pubmed ↗