Hemolytic uremic syndrome in severe acute pancreatitis
Jayaraj Hasvi, Inder Preet Singh Bhatia, Saurabh Dawra, Amulyajit Singh, Siddharth Tripathi

TL;DR
A rare case of hemolytic uremic syndrome occurred in a patient with severe acute pancreatitis, leading to a fatal outcome despite aggressive treatment.
Contribution
This case report highlights hemolytic uremic syndrome as an atypical and severe complication of acute pancreatitis.
Findings
Hemolytic uremic syndrome was diagnosed in a 36-year-old male with acute pancreatitis.
The patient had low C3, normal C4, and positive anti-complement factor H antibody.
Despite plasmapheresis, hemodialysis, and immunoglobulin therapy, the patient succumbed to the illness.
Abstract
Introduction: Hemolytic Uremic Syndrome is characterized by Coombs negative microangiopathic hemolytic anemia, severe thrombocytopenia, and acute kidney injury. Case Report: Here, we report a 36-year-old male, a case of alcohol related acute pancreatitis. On day 5, he developed fever and tachycardia. Evaluation revealed thrombocytopenia, hemolytic anemia, and acute kidney injury with low C3, normal C4 & ADAMTS13 activity and positive anti-complement factor H antibody. He was diagnosed as a case of Hemolytic Uremic Syndrome and managed with plasmapheresis, hemodialysis, and Intravenous immunoglobulin. He was administered Rituximab on day 15, considering the refractory nature of the disease. Despite the aggressive management, he succumbed to his illness. Conclusion: This case highlights atypical Hemolytic Uremic Syndrome as a rare complication of Acute Pancreatitis. Our patient, despite…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
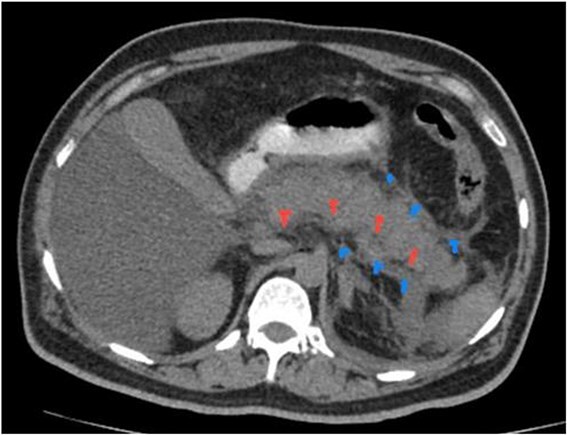 Figure 1
Figure 1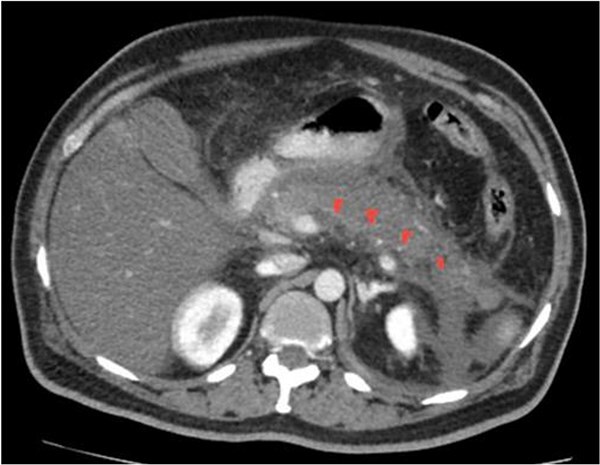 Figure 2
Figure 2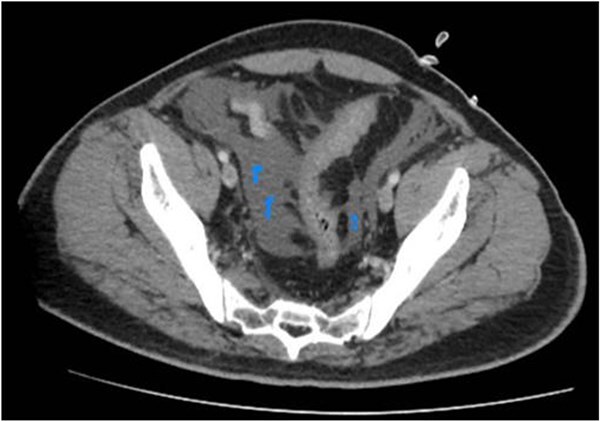 Figure 3
Figure 3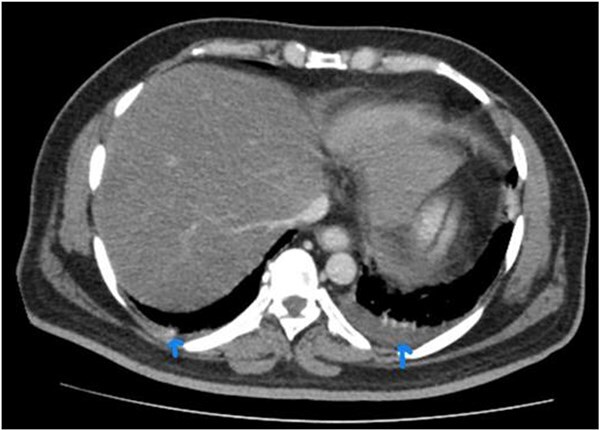 Figure 4
Figure 4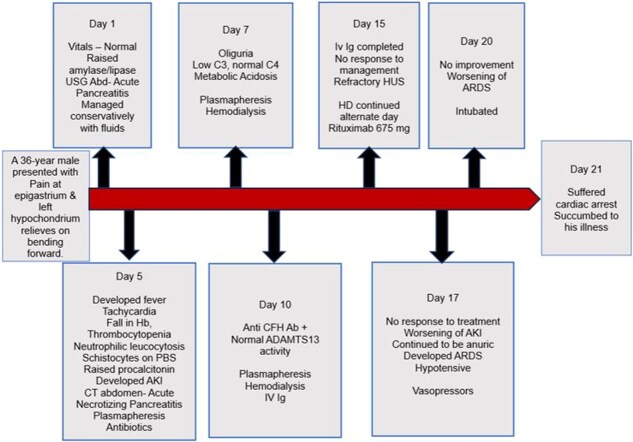 Figure 5
Figure 5| Lab | On | Day 5 | Day 07 | Day 10 | Day 15 | Day 20 |
|---|---|---|---|---|---|---|
| Parameters | admission | |||||
| Hb g/dl | 13.3 | 8.8 | 8.2 | 7.7 | 8.3 | 7.8 |
| TLC/uL | 9300 | 28 300 | 22 300 | 19, 400 | 17 500 | 22 500 |
| DLC | N-78%, | N- 94% | N- 89% | N- 90% | N- 86% | N- 92% |
| L- 18% | L- 02% | L- 07% | L—07% | L – 06% | L – 04% | |
| Platelets 103/ul | 1,75 000 | 29 000 | 36 000 | 32 000 | 48 000 | 38 000 |
| PT | 14.2 | 14.8 | 16.4 | 17.5 | ||
| INR | 1.0 | 1.1 | 1.2 | 1.3 | ||
| aPTT | 34 | 33 | 35 | 36 | ||
| Urea/Creatinine mg/dl | 43/1.0 | 74/3.5 | 89/5.5 | 112/7,2 | 138/7.9 | 170/9.2 |
| Na+/K+ mEq/L | 137/3.9 | 142/4.2 | 137/5.3 | 140/5.9 | 138/5.4 | 135/4.9 |
| Ca2+/Po43− mg/dl | 9.2/2.9 | 8.7/3.5 | 9.0/3.7 | 8.6/5.5 | 8.9/4.1 | 9.1/4.7 |
| Bilirubin (D/I) | 1.3/0.9 | 4.8/1.2 | 3.8/0.9 | |||
| mg/dl | ||||||
| SGOT/SGPT | 37/49 | 327/816 | 180/550 | |||
| IU/L | ||||||
| ALP/GGT | 110/278 | |||||
| Amylase | 1575 | |||||
| Lipase | 12 500 | |||||
| Procalcitonin | 58.01 | 28.7 | ||||
| Serum LDH | 181 | 1251 | 1130 | 1470 | ||
| Serum fibrinogen | 250 | |||||
| 200–500 mg/dl | ||||||
| D-Dimer ng/ml | 780 | |||||
| Urine C/S | No growth | |||||
| Blood C/s | No growth | |||||
| ABG | ||||||
| pH | 7.37 | 7.29 | 7.22 | 7.18 | 7.15 | 6.93 |
| pCo2 mm Hg, | 38 | 36 | 30 | 24 | 20 | 18 |
| HCO3− mmol/L | 21 | 20 | 17 | 12 | 09 | 05 |
| HbsAg | Negative | |||||
| Anti HCV | Negative | |||||
| HIV | Negative | |||||
| C3 mg/dl (82–160) | 47 | |||||
| C4 mg/dl (12–36.0) | 28 | |||||
| Anti CFH Ab AU/mL | 298.35 | |||||
| by ELISA (0–150) | ||||||
| ADAMTS13 Activity | 110% | |||||
| (60–130) |
| S. No | Year | Age, Sex | Etiology | Hb | Platelet | Creatinine | Treatment | Renal Replacement Therapy | Hematological remission | Renal outcome | Death |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1978 | 18, M | Idiopathic | 10.6 | 2 | 2.3 | SPLENECTOMY | No | Yes | CR | NO |
| 2 | 1981 | 32, M | Alcohol | 7.7 | 24 | 5.8 | FLUIDS | Yes | Yes | CR | No |
| 3 | 1989 | 55, F | Idiopathic | 8.0 | 24 | 1.7 | PLEX | No | Yes | CR | No |
| 4 | 1991 | 36, M | Alcohol | 9.2 | 45 | - | - | - | - | - | - |
| 5 | 1992 | 55, M | GSD | 10 | 20 | 7.9 | PLEX | Yes | Yes | CR | No |
| 6 | 1992 | 48, M | Alcohol | 8 | 40 | 2.1 | CS | No | No | - | Yes |
| 7 | 1995 | 18, M | Alcohol | 6 | 30 | 15.0 | PLEX | Yes | Yes | CR | No |
| 8 | 1997 | 25, M | Alcohol | 5 | 53 | 5.3 | PLEX | - | - | - | - |
| 9 | 1997 | 23, M | Alcohol | 7.6 | 45 | 6.9 | PLEX, CS | Yes | Yes | CR | NO |
| 10 | 1998 | 28, F | Idiopathic | 9.2 | 9 | 1.3 | - | - | - | - | - |
| 11 | 1998 | 65, M | GSD | 10.3 | 32 | 2.2 | PLEX | No | Yes | CR | No |
| 12 | 1998 | 37, M | Alcohol | 11.7 | 22 | 4.8 | PLEX | No | Yes | CR | No |
| 13 | 2000 | 70, M | Idiopathic | 7.7 | 22 | 2.4 | - | - | - | - | - |
| 14 | 2000 | 30, M | Alcohol | 7.6 | 63 | 8.3 | PLEX, CS, IVIg | No | Yes | CR | No |
| 15 | 2002 | 38, M | Alcohol | - | 28 | - | PLEX | Yes | Yes | CR | No |
| 16 | 2002 | 35, M | ERCP | 5.3 | 15 | 2.2 | PLEX, CS | No | Yes | CR | No |
| 17 | 2002 | 58, M | Alcohol | 8.3 | 14 | 3.2 | PLEX | Yes | Yes | CR | No |
| 18 | 2003 | 38, F | Alcohol | 9 | 24 | 7.7 | PLEX | Yes | Yes | CR | No |
| 19 | 2004 | 35, M | Alcohol | 4.6 | 30 | 1.45 | PLEX | No | No | CR | No |
| 20 | 2004 | 33, M | Alcohol | 5.8 | 90 | 7.0 | PLEX | Yes | - | - | - |
| 21 | 2005 | 55, F | ERCP | 12.1 | 50 | - | PLEX, RTX | Yes | Yes | - | No |
| 22 | 2005 | 19, M | GSD | 8.8 | 32 | 6.7 | PLEX | Yes | Yes | CR | No |
| 23 | 2005 | 43, M | Alcohol | 10.1 | 53 | 2.0 | - | No | Yes | CR | No |
| 24 | 2005 | 37, F | Sarcoidosis | 9.6 | 74 | 4.1 | PLEX | No | Yes | CR | No |
| 25 | 2006 | 35, F | GSD | 8.0 | 35 | 2.1 | PLEX | No | Yes | CR | No |
| 26 | 2010 | 74, M | Idiopathic | 6.4 | 20 | 6.4 | PLEX | Yes | Yes | PR | No |
| 27 | 2011 | 23, M | ERCP | 8.7 | 24 | 1.7 | PLEX | No | Yes | CR | No |
| 28 | 2011 | 40, F | Idiopathic | 5.9 | 11 | 5.7 | PLEX | No | Yes | CR | No |
| 29 | 2014 | 38, F | Alcohol | 8.8 | 32 | 1.45 | PLEX | Yes | Yes | CR | No |
| 30 | 2016 | 21, M | ERCP | 6.2 | 7.0 | 1.6 | PLEX, ECZ | No | Yes | CR | No |
| 31 | 2017 | 61, F | Alcohol | 9.3 | 25 | 1.8 | PLEX | No | Yes | PR | No |
| 32 | 2019 | 37, M | Alcohol | 7.3 | 28 | 7.1 | ECZ | No | Yes | CR | No |
| 33 | 2022 | 17, F | GSD | 6.6 | 16 | 2.98 | PLEX | Yes | Yes | CR | No |
| 34 | 2023 | 68, M | Idiopathic | 13.8 | 121 | 1.11 | Ulinastatin | No | Yes | CR | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsComplement system in diseases · Renal Diseases and Glomerulopathies · Blood groups and transfusion
Introduction
Acute Pancreatitis (AP) is an acute inflammatory process of the pancreas which can initiate a systemic inflammatory response syndrome (SIRS) resulting in acute respiratory distress syndrome (ARDS) and multi organ dysfunction. Common etiologies include gall stones, alcohol, hypertriglyceridemia, Endoscopic retrograde cholangiopancreatography, drugs, trauma, post-operative. Uncommon causes include hypercalcemia, infections, cystic fibrosis, autoimmune and hereditary causes. It is associated with various hematological complications like fall in serial values of hemoglobin, coagulation abnormalities, disseminated intravascular coagulation (DIC), acute hemolytic anemia, thrombocytopenia and thrombotic thrombocytopenic purpura or hemolytic uremic syndrome [1]. Hemolytic Uremic Syndrome (HUS) secondary to Acute Pancreatitis is a rare presentation [2] and total of 38 cases have been reported in the past [3–6]. HUS is characterized by a Coombs negative microangiopathic hemolytic anemia (MAHA), severe thrombocytopenia and acute kidney injury (AKI), and is associated with high mortality [7]. Hence, prompt diagnosis and timely initiation of appropriate management would result in favourable outcome.
Case report
36-year-old male, known case of pulmonary tuberculosis (2018, completed ATT) presented with a history of severe epigastric and left hypochondriac pain of 01-day duration, which was radiating to the back, relieved on bending forward. The patient gave a history of consumption of alcohol 2 days before the onset of symptoms. At the time of presentation, the patient gave no history of fever, palpitations, breathlessness, decreased urine output, any bleeding manifestations, any chest pain, breathlessness, cough, or hemoptysis.
On examination, his vitals (at admission) included a pulse of 84/minute, a blood pressure of 108/90 mm of Hg, a temperature of 98.7°F, respiratory rate of 18/minute and oxygen saturation of 97% at room air. There was no evidence of pallor, icterus, clubbing, lymphadenopathy or edema. Abdominal examination revealed tenderness over the left hypochondrium, with decreased bowel sounds. The rest of the general and systemic examination was normal, without any evidence of hepatosplenomegaly.
On further evaluation, he was found to have increased amylase (1575 IU/l) and lipase (12 500 IU/l) and Ultrasound abdomen was suggestive of Acute Pancreatitis. The rest of the hematological and biochemical parameters were normal. He was initially managed with parenteral fluids, analgesics, proton pump inhibitors and supportive care.
He underwent a CT abdomen on day 3 of admission, which revealed Acute Necrotizing Pancreatitis, with a modified CTSI score of 10/10 ([Figs 1](#f1 f2 f3)–4).
NCCT with oral contrast. It reveals bulky pancreas, peripancreatic fluid and fat stranding.
CECT with pancreatic phase. It reveals non enhancement of body and tail of pancreas, indicating necrotizing pancreatitis.
Further caudal scans reveal ascites.
CECT abdomen with visualized chest cuts in the same patient indicating bilateral pleural effusion.
On day 5 of admission, the patient developed fever. Evaluation revealed tachycardia (heart rate − 124/minute) with neutrophilic leucocytosis (total leucocyte count of 28 300; polymorphs- 94%, lymphocytes- 2%). He was also found to have a drop in haemoglobin (13.3 to 8.8 gm/dL) with thrombocytopenia (Platelets—1,75 000 to 29 000/mm^3^). Peripheral blood smear (PBS) showed toxic changes along with the presence of schistocytes (3.5%). Direct coombs test (DCT) and indirect coombs test (ICT) were negative. His serum procalcitonin was elevated (58.01 ng/ml, normal < 0.1 ng/ml). Renal parameters were found to be deranged (Urea/creatinine- 43/1.0 to 74/3.5 mg/dl) with abnormal liver function tests (bilirubin-1.3/0.9 to 4.8/1.2 mg/dl) and raised serum lactate dehydrogenase (LDH) (181 to 1251 IU/l). He was started on plasmapheresis (considering the possibility of hemolytic uremic syndrome), parenteral empirical antibiotics and was transfused with packed red blood cells and continued on parenteral fluids & other conservative measures.
On further evaluation, it was found that hemolytic anemia was pertaining to be complement mediated [decreased C3, normal C4, anti-compliment factor H antibody-positive; 298.35 AU/ml (0–150)]. ADAMTS13 activity was normal. He was managed as a case of Severe Acute Pancreatitis (Alcohol related), Atypical HUS with plasmapheresis, Intravenous Immunoglobulin (IVIg) (2 gm/kg body weight over 5 days) and alternate day hemodialysis. The patient had no response to the plasmapheresis & IVIg, continued to have schistocytes on PBS, thrombocytopenia and elevated LDH. He was administered Rituximab 675 mg (500 mg/m^2^) on day 15 of admission, considering the refractory nature of the disease. Despite intensive interventions, his condition continued to deteriorate, and he ultimately succumbed to his illness on the 21^st^ day of admission.
The timeline of the events and lab parameters of this case report have been summarized in Fig. 5 and Table 1 respectively.
Timeline of events.
Discussion
AP is an acute inflammatory process of the pancreas that can trigger a systemic inflammatory response. It is associated with various hematological complications like serial fall in hemoglobin, coagulation abnormalities, disseminated intravascular coagulation, acute hemolytic anemia, thrombocytopenia, and thrombotic thrombocytopenic purpura or hemolytic uremic syndrome [1].
HUS is a rare disease characterized by a Coombs negative microangiopathic hemolytic anemia (MAHA), severe thrombocytopenia and AKI [8]. The main pathology is thrombotic microangiopathy associated with endothelial cell injury and platelet activation, which mainly affects the kidney, as well as other organs [9]. HUS is usually categorized as typical, caused by Shiga toxin-producing Escherichia coli (STEC) infection and as atypical HUS (aHUS), usually caused by complement dysregulation due to mutations or autoantibodies, disorders of the degradation of von Willebrand factor (VWF), or secondary to a coexisting condition like cobalamin metabolism disorders, pregnancy/HELLP Syndrome, certain drugs (Chemotherapeutic drugs, immunosuppressants, antiplatelets etc) and other disorders (e.g. systemic diseases appearing as HUS, such as systemic lupus erythematosus and rejection after transplantation) [8]. These share a common pathogenetic mechanism of complement hyperactivation causing a prothrombotic and proinflammatory state on the endothelial cell surface, leading to endothelial damage and microvascular thrombosis [10].
Atypical HUS itself, is extremely rare, seen in adults with an incidence of 1 to 7 per 1 000 000 in the U.S. and Europe [7]. aHUS triggered by pancreatitis is definitely a very rare complication. Atypical HUS secondary to AP has previously been published in only a few case reports. It is generally accepted that pancreatitis can occur in TTP-HUS. But the occurrence of AP preceding the development of HUS with a short interval (1–13 days; median, 3 days) between the onset of pancreatitis and the development of HUS, suggests that the inflammatory response (secondary to pancreatitis) leading to endothelial damage is causally associated with the pathogenesis of TTP-HUS. The systemic inflammatory response mediated by IL-6, IL-8, TNF-α, and other cytokines, contributes to the development of HUS in Acute Pancreatitis [11].
Outcome is mostly good in childhood onset, Shiga toxin-associated HUS. But the renal complications are more common in adult, atypical and familial forms of HUS with a high mortality rate as well. End-stage renal disease (ESRD) or death occurs in about 33% to 40% of patients during the first clinical manifestation of atypical HUS. Within 1 year after a diagnosis of aHUS, up to 65% of patients treated with plasma exchange or infusion develop permanent renal damage and progression to ESRD, or die [12].
The treatment of HUS following AP is primarily supportive. Exchange plasmapheresis has been reported to be effective, with a response rate of 79% [13]. Rituximab (anti-CD20 antibody) is beneficial in refractory or relapsing HUS [14].
Long-term treatment with the anti-C5 monoclonal antibody, Eculizumab has been proven to be effective in aHUS. Furthermore, the current evidence suggests that Eculizumab, is effective in both aHUS and STEC-HUS and may have some benefit in TTP as well [10]. Eculizumab, a terminal complement inhibitor, is a humanized monoclonal antibody that acts by binding to the human C5 complement protein, with high affinity and blocks the generation of proinflammatory C5a and C5b-9. Thereby, inhibiting the complement-mediated thrombotic microangiopathy, decreases the need for thrombotic microangiopathy–related interventions. It also significantly improves the platelet count and renal functions. The earlier the intervention, the greater will be the clinical benefits.
Our case presented with features suggestive of AP. He underwent CT abdomen, findings of which were suggestive of Acute Necrotizing Pancreatitis, with a modified CTSI score of 10/10. On day 5, the patient developed features of SIRS. He was found to have neutrophilic leucocytosis with significant schistocytes on PBS. Furthermore, he was found to have raised procalcitonin, AKI, indirect hyperbilirubinemia and raised serum LDH. He was started with plasmapheresis on day 5 based on high suspicion of HUS. Further evaluation revealed low C3 levels, normal C4 levels with positivity for anti-Complement Factor H antibody. He was diagnosed with Atypical HUS. In addition to Plasmapheresis, IVIg (2 gm/kg body weight over 5 days) and alternate day hemodialysis were initiated. He received total of 8 sessions of plasmapheresis and considering the refractory nature of the disease, he was administered Rituximab on day 15 of admission. DIC was also considered as differential diagnosis, but normal fibrinogen, near normal values of D-Dimer & INR ruled out the possibility of DIC. Because of non-availability of eculizumab in our centre, this patient was managed with other modalities, initially with plasmapheresis (as it remains the first line of management at the centre where Eculizumab is not available), followed by plasmapheresis with IVIg and then Rituximab in view of refractory disease. There was no hematological/biochemical response to any of the treatment given. Despite all aggressive measures, he had a continuous downhill course and succumbed to his illness on 21^st^ day of admission. We believe, had the patient been administered Eculizumab, the result would have been favourable.
38 cases have been reported in the past as per literature since 1978 [3–6]. Characteristics with respect to patient demography, etiology, laboratory & biochemical parameters, treatment offered and the outcome of the patient of all the cases reported so far has been compiled in Table 2. Atypical HUS has occurred in Acute Pancreatitis of varied etiology, inferring no specific association of aHUS with any particular etiology of AP. The short median interval from onset of Acute Pancreatitis to occurrence of HUS suggests causal association, in the absence of other known potential triggers for aHUS. Likely pathogenesis being profound inflammatory response associated with Severe AP leading to compliment hyperactivation mediated endothelial damage and subsequently its consequences.
We suggest long term Eculizumab with apt supportive care as the mainstay of treatment for aHUS in AP and Exchange Plasmapheresis with IVIg or Corticosteroids as second line alternative therapy. Rituximab can be used in refractory or relapsing HUS cases.
Conclusion
Hemolytic Uremic Syndrome as a complication of Acute Pancreatitis is a rare presentation. Previously reported cases and this case highlights the possibility of aHUS secondary to Acute Pancreatitis. This condition should be diagnosed well in time as it is associated with high mortality. Lack of treatment protocol for aHUS in Pancreatitis makes management decisions difficult, leading to poor outcomes. HUS itself carries high mortality reaching as high up to 25%, but the overall outcome in the so far reported cases has been positive. This might be because of the under reporting of cases with unfavourable outcome. This emphasizes the need for further studies and research to streamline the management in such kind of cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1MW SAIF . DIC secondary to acute pancreatitis. Clin Lab Haematol 2005;27:278–82. 10.1111/j.1365-2257.2005.00697.x 16048498 · doi ↗ · pubmed ↗
- 2Swisher KK, Doan JT, Vesely SK. et al. Pancreatitis preceding acute episodes of thrombotic thrombocytopenic purpura-hemolytic uremic syndrome: report of five patients with a systematic review of published reports. Haematologica 2007;92:936–43. 10.3324/haematol.1096317606444 · doi ↗ · pubmed ↗
- 3Sandino-Pérez J, Gutiérrez E, Caravaca-Fontán F. et al. Haemolytic uraemic syndrome associated with pancreatitis: report of four cases and review of the literature. Clin Kidney J 2021;14:1713–3. 10.1093/ckj/sfab 05134252172 PMC 8264306 · doi ↗ · pubmed ↗
- 4Taner S, Karaçay IET, Arslan İ. Acute pancreatitis complicated by hemolytic uremic syndrome: a pediatric case. Egyptian Pediatric association. Gazette 2022;70:43. 10.1186/s 43054-022-00140-z · doi ↗
- 5Kajiyama T, Fukuda M, Rikitake Y. et al. Atypical Hemolytic uremic syndrome secondary to pancreatitis: a case report. Cureus 2023;15:e 35434. 10.7759/cureus.3543436994293 PMC 10041130 · doi ↗ · pubmed ↗
- 6Le Clech A, Simon-Tillaux N, Provôt F. et al. Atypical and secondary hemolytic uremic syndromes have a distinct presentation and no common genetic risk factors. Kidney Int 2019;95:1443–52. 10.1016/j.kint.2019.01.02330982675 · doi ↗ · pubmed ↗
- 7Noris M, Remuzzi G. Hemolytic uremic syndrome. J Am Soc Nephrol 2005;16:1035–50. 10.1681/ASN.200410086115728781 · doi ↗ · pubmed ↗
- 8Zimmerhackl L, Besbas N, Jungraithmayr T. et al. Epidemiology, clinical presentation, and pathophysiology of atypical and recurrent Hemolytic uremic syndrome. Semin Thromb Hemost 2006;32:113–20. 10.1055/s-2006-93976716575686 · doi ↗ · pubmed ↗