Spectrum of Cytogenetic Abnormalities in Adolescent and Young Adult Patients of B-Cell Acute Lymphoblastic Leukemia in a Tertiary Care Hospital in Pakistan
Sana Brohi, Israr A Shaikh, Fatima Tariq, Ammarah Tahir, Imran Iftikhar, Imran A Siddiqui, Syed W Bokhari, Muhammad Tariq Mahmood, Romena Qazi, Usman Ahmad

TL;DR
This study identifies common cytogenetic abnormalities in young adult B-cell ALL patients in Pakistan, highlighting the importance of genetic testing for better treatment planning.
Contribution
The study provides a detailed analysis of cytogenetic abnormalities in adolescent and young adult B-ALL patients in Pakistan, comparing them to other regions.
Findings
54% of B-ALL patients showed cytogenetic abnormalities.
The most common abnormality was t(9;22), found in 13.4% of patients.
Abstract
Introduction: Acute lymphocytic leukemia (ALL) is a malignancy of infiltration of B or T precursor lymphoid cells, i.e., lymphoblasts, in bone marrow and other lymphoid organs. Detection of various cytogenetic abnormalities in ALL patients is important for the purpose of prognosis and targeted treatment. The aim of this study is to identify the type and frequency of various cytogenetic abnormalities in adolescent and young adult precursor B-cell ALL (B-ALL) patients in Pakistan and compare them with patients of a similar age group in other European and Asian countries. Methods: A total of 134 B-ALL patients (112 male, 22 female), aged 18-40 years, were included in this cross-sectional retrospective study, with data from December 1, 2014, to March 30, 2020, conducted in the Department of Clinical Hematology and Oncology at Shaukat Khanum Memorial Cancer Hospital & Research Center,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
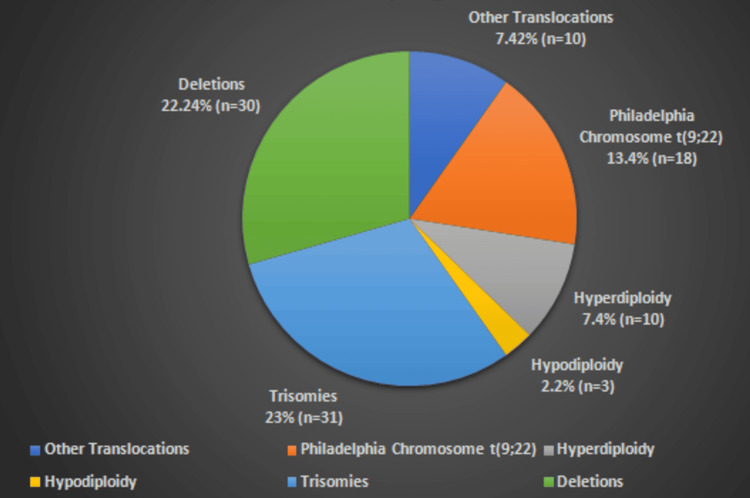 Figure 1
Figure 1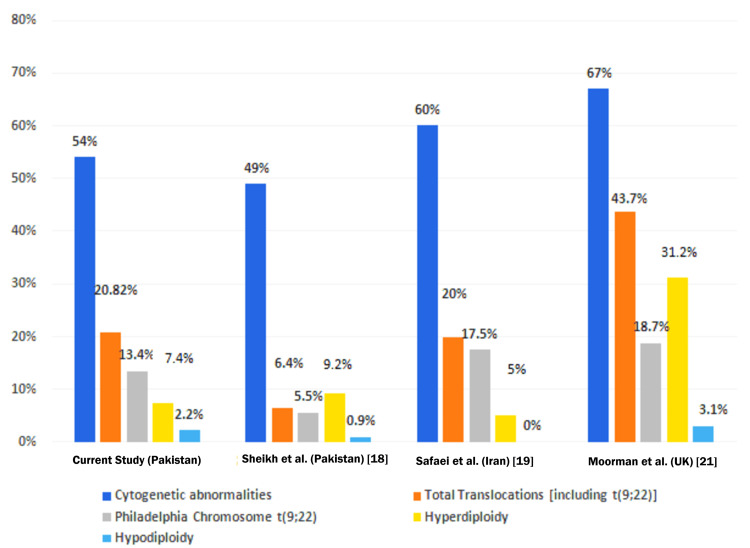 Figure 2
Figure 2| Cytogenetics | Frequency | Percentage |
| Abnormal Cytogenetics | 72 | 54% |
| Normal Cytogenetics | 62 | 46% |
| Translocations | Frequency | Percentage |
| t (9;22) | 18 | 13.4% |
| t (1;19) | 5 | 3.7% |
| t (1;3) | 2 | 1.5% |
| t (9;15) | 1 | 0.74% |
| t (1;2) | 1 | 0.74% |
| t (5;9) | 1 | 0.74% |
| Hyperdiploidy/Hypodiploidy | Frequency | Percentage |
| Hyperdiploidy | 10 | 7.4% |
| Hypodiploidy | 3 | 2.2% |
| Trisomy | Frequency | Percentage |
| Trisomy 21 | 5 | 3.7% |
| Trisomy 2 | 4 | 3% |
| Trisomy 12 | 4 | 3% |
| Trisomy 1 | 3 | 2.2% |
| Trisomy 5 | 3 | 2.2% |
| Trisomy 7 | 3 | 2.2% |
| Trisomy 4 | 2 | 1.5% |
| Trisomy 8 | 2 | 1.5% |
| Trisomy 3 | 1 | 0.74% |
| Trisomy 6 | 1 | 0.74% |
| Trisomy 9 | 1 | 0.74% |
| Trisomy 10 | 1 | 0.74% |
| Trisomy 13 | 1 | 0.74% |
| Deletion | Frequency | Percentage |
| 9p | 7 | 5.2% |
| 5q | 3 | 2.2% |
| 7p | 3 | 2.2% |
| 13q | 3 | 2.2% |
| 3q | 2 | 1.5% |
| 11q | 2 | 1.5% |
| 12p | 2 | 1.5% |
| 13p | 2 | 1.5% |
| 3p | 1 | 0.74% |
| 6q | 1 | 0.74% |
| 7q | 1 | 0.74% |
| 8q | 1 | 0.74% |
| 9q | 1 | 0.74% |
| 1p | 1 | 0.74% |
| Parameters | Current study (Pakistan) | Sheikh et al. (Pakistan) [ | Safaei et al. (Iran) [ | Moorman et al. (United Kingdom) [ |
| Sample number (n) | 134 | 121 | 46 | 115 |
| Age (years) | 18-40 | 15-29 | 35.36±14.82 | 15-29 |
| Cytogenetic abnormalities (%) | 54% | 49% | 60% | 67% |
| Total translocations Including t(9;22) (%) | 20.82% | 6.4% | 20% | 43.7% |
| Philadelphia Chromosome t(9;22) (%) | 13.4% | 5.5% | 17.5% | 18.7% |
| Hyperdiploidy (%) | 7.4% | 9.2% | 5% | 31.2% |
| Hypodiploidy (%) | 2.2% | 0.9% | 0% | 3.1% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Lymphoblastic Leukemia research · Chronic Lymphocytic Leukemia Research · Immunodeficiency and Autoimmune Disorders
Introduction
Acute lymphocytic leukemia (ALL) is characterized by genetic alterations that disrupt lymphoid precursor cell differentiation and promote proliferation [1]. These alterations are critical for risk stratification and the development of targeted therapies [2], as well as targeted therapies. WHO Classification of Hematolymphoid Tumors, 5th edition (B-cell lymphoid proliferations and lymphomas) classifies precursor B-cell Neoplasms as a separate entity [3]. Conventional cytogenetics has been used to analyze genome modifications that include genomic gains and losses, as well as rearrangements within and between chromosomes [4]. The detection and assessment of cytogenetic abnormalities play a vital role in prognostication and treatment of this aggressive hematologic malignancy [5].
Most ALL cases exhibit an abnormality either in chromosome number (ploidy) or in their structure (i.e., translocations, deletions, or inversions) [6]. Technical challenges, such as poor chromosome morphology and indistinct banding patterns, often complicate cytogenetic analysis in ALL [5,7]. However, with significant improvements in banding techniques, the rate of detection of chromosomal abnormalities in ALL has gone up to 60-85% [8-12]. According to the Third International Workshop on Chromosomes in Leukemia (TIWCL), only 39% of cytogenetic changes occur in T-cell ALL, the rest being associated with B-cell ALL [8].
Secker-Walker et al. first reported the significance of cytogenetics in the prognosis of childhood ALL in 1989 [12]. According to their research, hyperdiploid karyotypes had a better prognosis compared to hypodiploid or pseudodiploid cases. These analytics were further confirmed in the follow-up study [13] as well as by other investigators [10,14,15]. The TIWCL reported that cytogenetic studies can help in the risk stratification of ALL patients, while also giving an insight into their disease-free-survival (DFS), complete remission (CR), and remission duration [8].
Cytogenetic profiling in ALL is crucial for risk stratification and treatment selection, yet limited data exist on adolescents and young adults in Pakistan. Differences in genetic backgrounds may influence the frequency of specific chromosomal abnormalities, impacting prognosis and therapeutic decisions. This study aims to analyze cytogenetic patterns in Pakistani patients and compare them with global data, providing insights into population-specific trends.
Materials and methods
This was a cross-sectional retrospective study conducted at the Department of Clinical Hematology and Oncology at Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore, Pakistan. The study was approved by the Institutional Review Board of Shaukat Khanum Memorial Cancer Hospital & Research Center (approval number: EX-13-10-20-20).
A total of 134 patients with B-cell ALL, aged 18-40 years, were recruited from December 1, 2014, to March 30, 2020. Inclusion criteria were patients who presented through the walk-in clinic and were diagnosed with B-ALL via immunophenotyping using flow cytometry at our hospital. Patients within the specified age range were excluded only if cytogenetic analysis was not performed for any reason.
Karyotyping procedure
Our laboratory’s Cytogenetics Section receives samples for the detection of different chromosomal abnormalities by conventional karyotyping from hospital-registered and outside patients diagnosed with B-ALL on immunophenotyping by flow cytometry. Conventional karyotyping is performed on bone marrow samples with ≥20% blast cells by laboratory technologists. Samples are collected in green top sodium/lithium heparin tubes to prevent clotting and maintain sample viability for analysis. The temperature for transport is maintained at 15-25°C, which helps preserve the sample’s integrity until it reaches the laboratory, while ensuring it’s delivered within 24 hours, which is crucial for optimal culture conditions. The bone marrow aspirate sample is then cultured in duplicates/triplicates, depending on the request. Samples are cultured within 48 hours of receipt to optimize metaphase yield from blast cells. Specimens are then stored at 2-8^ o^C after culture and harvested using the hypotonic solution potassium chloride (KCl) at 37°C for swelling the cells, allowing chromosomes to spread out properly for analysis. After that, the slides are prepared using the Hanabi PVI metaphase spreader, a common tool in cytogenetics for ensuring even distribution of the cells. Staining with Dulbecco’s phosphate-buffered saline (PBS) pH 7.0, trypsin, and Harleco Giemsa stain is performed to enhance visibility of the chromosomal structures, ensuring that they are clear and identifiable under the microscope.
Chromosomal analysis
For chromosomal analysis, Cyto-Vision MB8 (Leica Biosystems, Nussloch, Germany), a dedicated software tool for capturing and analyzing cytogenetic data, was used. Neoplastic disorders, like ALL, require the analysis of at least 20 cells (preferably with a minimum of 400 bands level resolution), ensuring that enough data is available to detect any structural or numerical chromosomal abnormalities that may be contributing to the leukemia. Scoring and interpretation of cytogenetics was performed using the International System for Human Cytogenomic Nomenclature (ISCN 2020) [16], as the reference standard, allowing standardization of reports and comparisons with global data.
Results
Out of 134 patients diagnosed with B-ALL by flow cytometry, 72 (54 %) showed different cytogenetic abnormalities, while 62 (46 %) showed normal karyotype, as shown in Table 1. The summary of all chromosomal abnormalities in B-ALL patients is given in Figure 1.
Spectrum of cytogenetic abnormalities in the B-cell acute lymphocytic leukemia patients
Translocations
Of all the screened cytogenetics, translocation between chromosomes 9 and 22, t (9;22), was the commonest abnormality. Translocation between chromosomes 9 and 22, t(9;22), was found in 18 (13.4 %) patients, while translocation between chromosome 1 and 19, t(1;19), was found in five (3.7 %) patients. Other translocations found were t(1;3), t(9;15), t(1;2) and t(5;9), as shown in Table 2.
Hyperdiploidy and hypodiploidy
Out of 134 patients analyzed, 10 (7.4%) were hyperdiploid while three (2.2%) showed hypodiploidy, as shown in Table 3.
Trisomy
Trisomy 21 (n=5, 3.7%) was the most prevalent anomaly found in this group, followed by trisomy 2 and 12 (n=4, 3%). Other anomalies are shown in Table 4.
Deletions
Deletion 9p was observed in seven (5.2%) patients, followed by deletion 5q, 7p, and 13q, which were found in three (2.2%). Other deletions are shown in Table 5.
Complex karyotype
The WHO defines complex karyotype as the presence of more than or equal to three chromosomal abnormalities [17]. Out of 134 B-ALL patients, 19 (14.1%) showed complex karyotypes.
Discussion
In our study, 54% (n=72) of patients exhibited chromosomal abnormalities, including structural and/or numerical changes. This aligns closely with findings from another local study (49%) [18], suggesting consistent cytogenetic patterns in Pakistani B-ALL patients. However, Safaei et al. [19] reported the incidence at 61.7% while Lazaryan et al. [20] found chromosomal anomalies in 36.5% of patients.
Translocation between chromosome 9 and 22, i.e., t(9;22), BCR-ABL1, which result in Philadelphia chromosome responsible for activation of a tyrosine kinase, was found in 13.4% patients in our study, which is comparable to frequency of 15% as reported by Moorman et al. [21] and 10% as reported by Shaikh et al. [18]. The second most common translocation found in our study was translocation between chromosomes 1 and 19, t(1;19), with a frequency of 3.7%, resulting in the TCF3:PBX1 protein complex. Yilmaz et al. [22] and Uckun et al. [23] reported t(1;19) in 4% of adults, which closely resembles our finding. As reported by Chen et al., the pediatric population with ALL has a high incidence of hyperdiploidy with a frequency of 17.6%, while adult patients with ALL have a lower frequency of 4.4% [24]. In our study, the frequency of hyperdiploidy in adolescents and young adult B-ALL patients was found to be 7.4%, which is higher than the frequency in adults but lower than the pediatric population as reported in the study by Chen et al. [24], but it is comparable to 6.6% as reported by Shaikh et al. [18]. Hypodiploidy in B-ALL, which carries a poor prognosis, was found in 2.2% of the patients in our study, but it was reported to be 0.6% by Shaikh et al. [18].
The frequency of various trisomies in our study was 3.7%, which is higher than the frequency reported in a study by Raimondi et al. (1.8%) [25]. Abnormalities of the short arm of chromosome 9 are found in approximately 9% of adults [26]. In our study, deletion of the short arm of chromosome 9 (del 9p) was found in 5.2%, and deletion of the long arm of chromosome 5 (i.e., del 5q), which is uncommon in ALL [27], was found in 2.2 %of our study population.
Table 6 and Figure 2 show a comparison of cytogenetic abnormalities found in the current study and those found in other studies conducted in Pakistan, Iran, and the United Kingdom in similar age groups. It is to be noted that cytogenetic abnormalities were detected in >50% of the population in each study. Hyperdiploidy is more common than hypodiploidy, and translocations take up to one-third of cytogenetic alterations, with the Philadelphia chromosome t(9; 22) (q34; q11) being the most common abnormality.
Comparison of cytogenetic abnormalities found in acute lymphocytic leukemia in different populationsReferences: [18,19,21]
Limitations
It is noted that conventional cytogenetics cannot detect cryptic chromosomal abnormalities. Therefore, the finding of 46% of patients with normal karyotypes in our study may harbor undetected abnormalities. Additional molecular techniques, such as fluorescence in situ hybridisation (FISH), polymerase chain reaction (PCR), or next-generation sequencing (NGS), are required to fully exclude genetic alterations in these cases.
Conclusions
Our findings highlight the importance of cytogenetic analysis in B-ALL for risk stratification and targeted therapy, particularly in regions with limited access to advanced molecular diagnostics. However, further research is warranted to assess genetic alterations in B-ALL patients using advanced methodologies such as FISH, PCR, or NGS, which could reveal novel mutations and help refine personalized treatment approaches.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute lymphocytic leukemia Stat Pearls [Internet] Puckett Y Chan O Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 459149/
- 2Genetics and prognosis of ALL in children vs adults Hematology Am Soc Hematol Educ Program Roberts KG 137145201820183050430210.1182/asheducation-2018.1.137PMC 6245970 · doi ↗ · pubmed ↗
- 3The 2016 revision of the World Health Organization classification of lymphoid neoplasms Blood Swerdlow SH Campo E Pileri SA 2375239012720162698072710.1182/blood-2016-01-643569 PMC 4874220 · doi ↗ · pubmed ↗
- 4Genetic abnormalities in ALL Cytogenetics - Classical and Molecular Strategies for Analysing Heredity Material Bendari M Sraidi S Khoubila N London, UK Intech Open 2021
- 5Primary chromosome abnormalities in human neoplasia Adv Cancer Res Heim S Mitelman F 143521989266271010.1016/s 0065-230x(08)60209-2 · doi ↗ · pubmed ↗
- 6A direct bone marrow chromosome technique for acute lymphoblastic leukemia Cancer Genet Cytogenet Williams DL Harris A Williams KJ Brosius MJ Lemonds W 239257131984638882110.1016/0165-4608(84)90046-3 · doi ↗ · pubmed ↗
- 7The Third International Workshop on Chromosomes in Leukemia. Lund, Sweden, July 21-25, 1980. Introduction Cancer Genet Cytogenet Mitelman F 969841981 https://pubmed.ncbi.nlm.nih.gov/7332898/7332898 · pubmed ↗
- 8Chromosomal abnormalities in acute lymphoblastic leukemia Cancer Res Bloomfield CD Lindquist LL Arthur D Mc Kenna RW Le Bien TW Nesbit ME Peterson BA 483848431271981 https://pubmed.ncbi.nlm.nih.gov/7028252/7028252 · pubmed ↗