Deep Fungal Stromal Keratitis After Cataract Surgery: A Case Report
Seika Narai, Atsuhiko Fukuto, Tai-ichiro Chikama, Yosuke Harada, Hirokazu Sakaguchi

TL;DR
A rare case of deep fungal eye infection after cataract surgery was successfully treated with amphotericin B after other antifungal treatments failed.
Contribution
Highlights the diagnostic role of in vivo confocal microscopy and treatment success with amphotericin B in deep stromal fungal keratitis.
Findings
In vivo confocal microscopy identified filamentous structures in deep stromal fungal keratitis.
Amphotericin B via multiple routes resolved the infection when other treatments failed.
Therapeutic keratoplasty was avoided through effective antifungal treatment.
Abstract
Fungal keratitis is a vision-threatening infection that typically originates at the ocular surface and gradually invades the deeper layers of the cornea. We report a rare fungal keratitis confined to the deep stromal layer that developed following cataract surgery. An 81-year-old woman presented with a creeping white opacity on the posterior corneal surface in the right eye. Anterior segment optical coherence tomography revealed a hyper-reflective lesion at the posterior cornea, and in vivo confocal microscopy showed filamentous structures in the deep stroma, supporting the diagnosis of fungal keratitis. Corneal scraping was not feasible because the lesion was deep within the cornea. Initial treatment with natamycin and fluconazole was ineffective, and the infection progressed despite topical and systemic voriconazole. Ultimately, the infection resolved after administering amphotericin…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
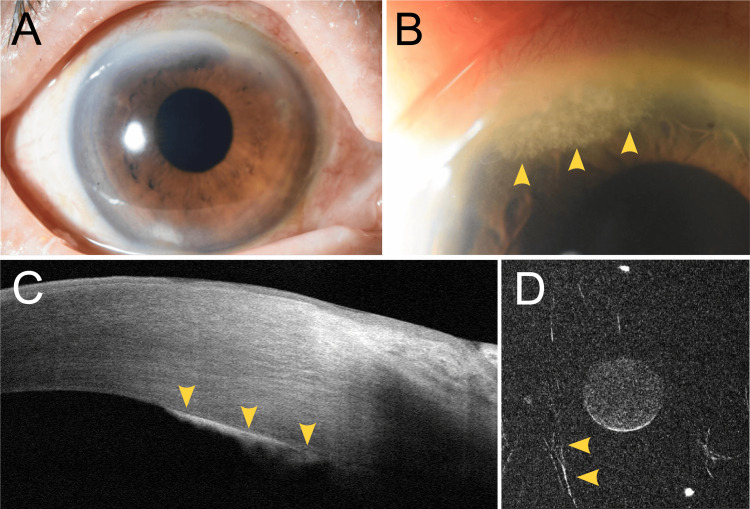 Figure 1
Figure 1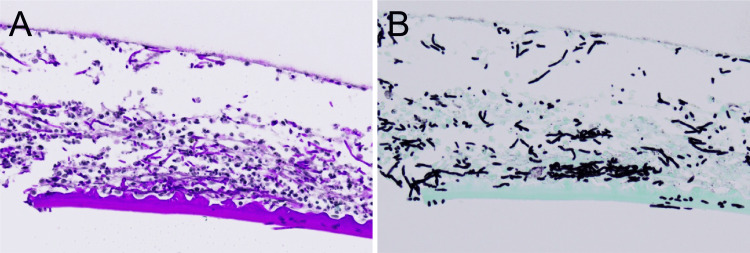 Figure 2
Figure 2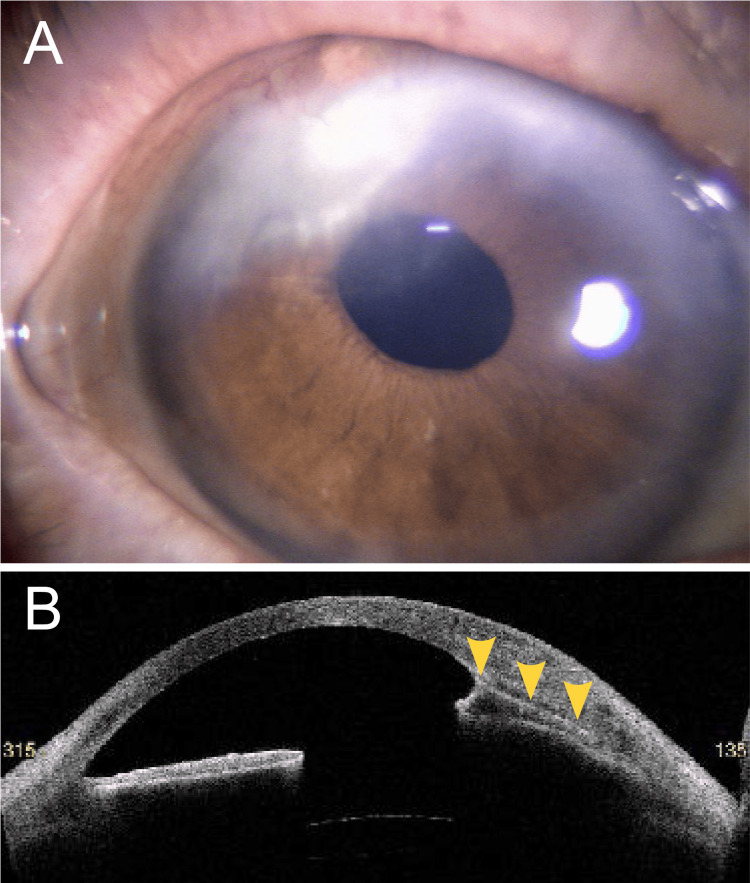 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Infections and Treatments · Ocular Surface and Contact Lens · Intraocular Surgery and Lenses
Introduction
Fungal keratitis is a severe ocular infection that can cause irreversible vision loss if not promptly treated [1]. It originates at the ocular surface and gradually extends into the deeper corneal layers [2]. Cases of fungal keratitis confined solely to the deep corneal stroma are rare and pose diagnostic challenges, as corneal scraping often fails to identify the causative organism [3]. Here, we report a rare fungal keratitis localized to the deep corneal stroma that developed following cataract surgery.
Case presentation
The patient was an 81-year-old woman with a medical history of hypertension, diabetes mellitus, and bilateral dacryocystitis. She underwent bilateral cataract surgery at a local ophthalmology clinic. Two months later, conjunctival injection and anterior chamber inflammation were observed in her right eye, raising suspicion of endophthalmitis. Pars plana vitrectomy was subsequently performed. Culture of the vitreous sample obtained during surgery yielded negative results. Postoperatively, she was prescribed topical betamethasone phosphate 0.1%. Two months after the vitrectomy, a feathery white infiltrate suggestive of fungal infection was noted at the posterior corneal surface of the right eye, and she was referred to the Department of Ophthalmology at Hiroshima University Hospital. Her best-corrected visual acuity in the right eye at the initial visit was 20/20. There was no conjunctival hyperemia, and no inflammatory cells were observed in the anterior chamber or vitreous (Figure 1A). A white, creeping infiltrate was observed on the posterior surface of the cornea, and anterior segment optical coherence tomography revealed a corresponding hyper-reflective lesion at the posterior cornea (Figures 1B, 1C). Fungal keratitis was suspected at the initial visit, prompting immediate discontinuation of betamethasone eye drops and initiation of natamycin 5% eye drops, fluconazole 0.2% eye drops, and oral fluconazole 200 mg twice daily. Two days later, marked conjunctival hyperemia and anterior chamber inflammation developed in the right eye. In vivo confocal microscopy revealed filamentous structures, confirming the diagnosis of fungal keratitis (Figure 1D).
Anterior segment findings of the right eye.(A) Diffuse illumination. (B) Scleral scatter illumination revealed a posterior corneal opacity (yellow arrowheads). (C) Anterior segment optical coherence tomography (AS-OCT) image of the superior cornea revealed a hyper-reflective lesion at the posterior corneal surface (yellow arrowheads). (D) In vivo confocal microscopy of the deep corneal stroma revealed filamentous structures (yellow arrowheads).
Due to worsening conjunctival injection and anterior chamber inflammation, fluconazole eye drops were discontinued. Voriconazole 1% eye drops (six times daily) and oral voriconazole 400 mg/day were initiated. Despite treatment, the posterior corneal infiltrate enlarged, conjunctival hyperemia worsened, and hypopyon developed. On day seven after the initial visit, anterior chamber irrigation was performed. During surgery, Descemet’s membrane at the lesion site was detached and excised. Histopathological examination of the excised tissue revealed fungal hyphae within the deep stroma and Descemet’s membrane, which stained positively with periodic acid-Schiff and Grocott stains (Figure 2).
Histopathological images of the excised tissue.Top: stromal side; bottom: endothelial side. (A) Periodic acid–Schiff stain. (B) Grocott stain. All images were taken at ×20 magnification.
Culture of the excised tissue was negative. Following surgery, intravenous voriconazole 400 mg/day, topical voriconazole 1%, and intrastromal voriconazole injections were administered. However, the infection did not improve. On day 16, a second anterior chamber irrigation was performed, and on day 20, antifungal treatment was switched to intravenous amphotericin B 120 mg/day, topical amphotericin B 0.1%, and intrastromal amphotericin B injections. Conjunctival hyperemia gradually improved, and one month after the initial visit, the posterior corneal infiltrate had resolved. Amphotericin B was then discontinued. No recurrence of fungal infection was observed during the three-month follow-up period after cessation of antifungal therapy (Figure 3).
Anterior segment findings at four months after the initial visit.(A) The superior corneal lesion had healed with scarring. (B) Anterior segment optical coherence tomography (AS-OCT) shows anterior synechiae (yellow arrowheads).
Discussion
The significant risk factors for fungal keratitis include soft contact lens wear, a history of corneal transplantation, ocular surface diseases, and ocular trauma [1,2]. Fungal infection occurring at or near the site of a cataract surgery incision, as observed in this case, has been infrequently documented in the literature [4-10]. Most reported pathogens have been of Aspergillus species [4,6,8-10], and some cases have ultimately required therapeutic keratoplasty [6-9]. Although the causative organism could not be identified in our case, antifungal therapy proved effective, allowing us to avoid corneal transplantation. There is no consensus regarding the optimal choice of antifungal agents for treating fungal keratitis. However, natamycin is generally considered the first-line treatment, and voriconazole has been reported to be effective, particularly for non-Fusarium infections [11]. In the present case, topical natamycin showed minimal efficacy, prompting the addition of topical and systemic voriconazole. Despite two anterior chamber irrigations, the infection relapsed. Subsequently, treatment was switched to amphotericin B via topical administration, intrastromal injection, and intravenous infusion, ultimately leading to the infection's resolution. Although amphotericin B is generally not preferred as a first- or second-line agent due to its potential for serious adverse effects such as nephrotoxicity and hypokalemia, it proved effective in this case. In vivo confocal microscopy enables real-time diagnosis of fungal keratitis and allows visualization of fungal hyphae located in the deep corneal stroma [3]. When used for the diagnosis of fungal keratitis, in vivo confocal microscopy has been reported to have a sensitivity of 94% and a specificity of 78% [12]. Corneal scraping could not be performed in the present case because the lesion was confined to the deep stroma. However, in vivo confocal microscopy facilitated early diagnosis and confidently supported the continued administration of antifungal agents.
Conclusions
This case demonstrates that fungal keratitis can occur in the deep corneal stroma following cataract surgery, even without surface involvement. In vivo confocal microscopy, a real-time and noninvasive imaging modality, was instrumental in establishing an early diagnosis and guiding antifungal therapy when conventional scraping was not feasible. Prompt initiation of appropriate antifungal treatment, including amphotericin B, led to successful resolution without the need for keratoplasty.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fungal keratitis: changing pathogens and risk factors Cornea Jurkunas U Behlau I Colby K 6386432820091951290810.1097/ICO.0b 013e 318191695 b · doi ↗ · pubmed ↗
- 2Fungal keratitis: emerging trends and treatment outcomes Eye Contact Lens Iyer SA Tuli SS Wagoner RC 2672713220061709938610.1097/01.icl.0000249595.27520.2e · doi ↗ · pubmed ↗
- 3Role of confocal microscopy in the diagnosis of fungal and acanthamoeba keratitis Ophthalmology Vaddavalli PK Garg P Sharma S Sangwan VS Rao GN Thomas R 293511820112080151510.1016/j.ophtha.2010.05.018 · doi ↗ · pubmed ↗
- 4Aspergillus terreus infection in a sutureless self-sealing incision made during cataract surgery Mycopathologia Erdem E Kandemir H Arıkan-AkdağlıS Esen E Açıkalın A Yağmur M İlkit M 12913417920152536253610.1007/s 11046-014-9829-2 · doi ↗ · pubmed ↗
- 5Alternaria keratitis and hypopyon after clear-cornea phacoemulsification J Cataract Refract Surg Espósito E Maccio JP Monti R Cervi L Serra HM Urrets-Zavalía JA 3313344020142446150610.1016/j.jcrs.2013.12.003 · doi ↗ · pubmed ↗
- 6Fungal infection of sutureless self-sealing incision for cataract surgery Ophthalmology Garg P Mahesh S Bansal AK Gopinathan U Rao GN 2173217711020031459752610.1016/S 0161-6420(03)00861-3 · doi ↗ · pubmed ↗
- 7Nocardia infection following phacoemulsification Indian J Ophthalmol Gokhale NS Garg P Rodrigues C Haldipurkar S 59615520071718989010.4103/0301-4738.29498 · doi ↗ · pubmed ↗
- 8Spectrum of clear corneal incision cataract wound infection J Cataract Refract Surg Kehdi EE Watson SL Francis IC Chong R Bank A Coroneo MT Dart JK 170217063120051624677110.1016/j.jcrs.2005.02.033 · doi ↗ · pubmed ↗