False–positive phenomenon in microbubble testing: unveiling the underlying mechanism
Yumi Yamamoto, Yasuhide Mochizuki, Saaya Ichikawa-Ogura, Rumi Hachiya, Hiroto Fukuoka, Toshiro Shinke

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
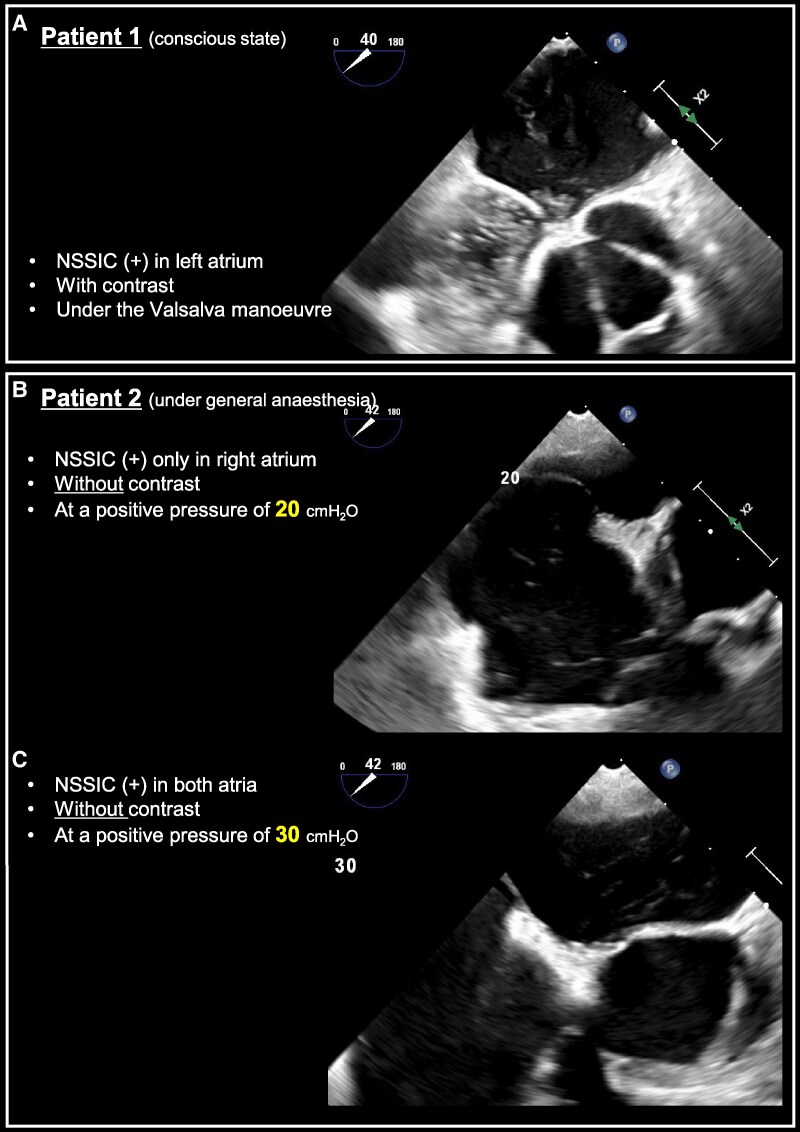 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFluid Dynamics and Mixing
We present two interesting cases of false–negative findings in microbubble tests. A woman in her 50 s (Patient 1), diagnosed with cerebral embolism in the middle cerebral artery, underwent transoesophageal echocardiography (TOE) to investigate embolic stroke of undetermined source. A microbubble test using agitated saline on TOE under the awake state suggested a right-to-left shunt (RLS) of Grade III during the Valsalva manoeuvre (VM) without external abdominal compression, indicating paradoxical embolism due to a patent foramen ovale (PFO). However, microbubble tests using both transthoracic echocardiography and transcranial Doppler were negative for RLS. Careful observation of the TOE revealed that microbubble-like echoes suddenly appeared in the left atrium (LA) within three cardiac cycles immediately after VM release, showing filamentous, high echogenicity resembling a snowstorm without PFO (Figure 1A, Supplementary data online, Video S1). This phenomenon was identified as non-smoke spontaneous individual contrast (NSSIC), characterized by rouleaux formation of blood in the pulmonary veins and appearing in the LA during VM.
In another patient (Patient 2: a man in his 50 s) with PFO, when VM was applied via positive pressure ventilation under general anaesthesia during percutaneous PFO closure, the same phenomenon occurred without microbubble injection. Interestingly, at a positive pressure ventilation of 20 cmH_2_O, this phenomenon was observed only in the right atrium (Figure 1B, Supplementary data online, Video S2), while at 30 cmH_2_O, it appeared in both atria (Figure 1C, Supplementary data online, Video S3). These cases suggest that the intensity of VM may influence the appearance of NSSIC. Patients capable of strong VM should be carefully evaluated for this false–positive phenomenon.
Supplementary Material
qyaf056_Supplementary_Data